See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/241734999 Clinical outcomes for psychotic and co-morbid patients admitted to acute psychiatric wards in four European centres... Article in Mental Health and Substance Use dual diagnosis · August 2012 DOI: 10.1080/17523281.2012.658081 CITATIONS 0 READS 29 11 authors, including: Alex Baldacchino University of St Andrews 104 PUBLICATIONS 1,993 CITATIONS SEE PROFILE All content following this page was uploaded by Alex Baldacchino on 31 May 2014. The user has requested enhancement of the downloaded file. All in-text references underlined in blue are linked to publications on ResearchGate, letting you access and read them immediately.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Seediscussions,stats,andauthorprofilesforthispublicationat:https://www.researchgate.net/publication/241734999
Clinicaloutcomesforpsychoticandco-morbidpatientsadmittedtoacutepsychiatricwardsinfourEuropeancentres...
ArticleinMentalHealthandSubstanceUsedualdiagnosis·August2012
DOI:10.1080/17523281.2012.658081
CITATIONS
0
READS
29
11authors,including:
AlexBaldacchino
UniversityofStAndrews
104PUBLICATIONS1,993CITATIONS
SEEPROFILE
AllcontentfollowingthispagewasuploadedbyAlexBaldacchinoon31May2014.
Theuserhasrequestedenhancementofthedownloadedfile.Allin-textreferencesunderlinedinbluearelinkedtopublicationsonResearchGate,lettingyouaccessandreadthemimmediately.

For Peer Review O
nly
Clinical Outcomes for Psychotic and Co-morbid Patients
Admitted to Acute Psychiatric Wards in Four European
Centres - Follow up to 6 months
Journal: Mental Health and Substance Use
Manuscript ID: Draft
Manuscript Type: Original Article
Keywords: comorbidity, dual diagnosis, mental health, psychosis
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
For Peer Review O
nly
1
Clinical Outcomes for Psychotic and Co-morbid Patients Admitted to Acute Psychiatric
Wards in Four European Centres - Follow up to 6 months.
Abstract
Background: This study was conducted with the aim of identifying the outcome and
characteristics of patients admitted to acute psychiatric wards with a diagnosis of psychotic
illness and substance misuse. Methods: In this multi-centre collaborative and opportunistic
study patients were allocated into 4 cohorts based on the type of drug use and then were followed
up 1 and 6 months later. Results: The total PANSS score improved significantly by the 6
month follow up in all but the cannabis using cohort, which initially had the lowest symptom
level. All cohorts improved significantly in levels of general symptoms, and 3 out of the 4
groups improved in the levels of positive symptoms (the cannabis and other drug cohort was
nearing significance at p=0.02). The biggest contrast between the groups was in the levels of
negative symptoms. These improved only in the non-drug using cohort; however even with this
significant improvement, levels did not reach the lower levels initially evident in the cannabis
only using cohort. Conclusions: Psychopathology and recovery processes of psychotic patients
admitted to acute psychiatric wards will differ depending on their use of illicit substances. In
particular those who use cannabis but not other illicit substances are likely to have lower levels
of negative symptoms.
Page 1 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
2
Clinical Outcomes for Psychotic and Co-morbid Patients Admitted to Acute Psychiatric
Wards in Four European Centres - Follow up to 6 months.
Introduction
Patterns of co-morbidity of drug use and psychiatric illness have been the subject of much
research taking many approaches. These range from individual case studies (Chaudry et al.,
1991) to the association between specific drugs (Arendt et al.,2005; McGuire et al.,1994;
Zammit et al.,2008; Degenhardt et al.,2007) looking for causal links (Ferdinand et al.,2005;
Fergusson et al.,2005), or substance use patterns in psychotic patients (Verdoux et al.,2005;
Virgo et al.,2001). Much focus on the subject of co-morbidity has been on connections between
drug use and psychosis; at predictors and patterns of drug use and patterns of psychopathology in
co-morbid versus non-co-morbid patients (Dalmau et al.1999; Grace et al.,2000; Kaiser et
al.2005; Pencer & Addington,2003; Sevy et al.,2001). Where patients are co-morbid the
evidence suggests there is a poorer prognosis (Grech et al., 2005). There is also evidence for
poorer treatment compliance in this patient group (Pencer & Addington, 2003). In spite of this
there has been little work done on the clinical outcomes and course of illness in this group of
patients.
The aim of this multi-centre collaborative and opportunistic study was to identify and compare
the clinical characteristics of patients diagnosed with a psychotic illness depending on their illicit
substance use at admission to acute psychiatric wards. In addition to this, patients were followed
up at 1 and 6 months. Outcomes were investigated based on the patterns of illicit substance use
Page 2 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
3
at baseline. Detailed information on the baseline data is reported elsewhere (Baldacchino et al.,
2009).
Methods
Design and settings
Patients were recruited from acute general psychiatric wards during a 12 month period between
2002 and 2005. Four centres participated in the Denmark, Germany, the UK, and Italy. In the
UK this was Springfield Psychiatric Hospital, London serving a population of just over 1 million.
In Germany this was the Department for Psychiatry and Psychotherapy, LVR-Hospital Essen,
serving a population of 210,000. In Italy, this was the Department of Addiction, Ospedali
Riuniti di Bergamo (combined hospitals of Bergamo) serving a population of 500,000. In
Denmark this was the Embedslaege Institutionen, Ringkobing recruiting patients in Holstebro
and Herning, serving populations of 85,000 and 115,000 respectively.
The inclusion criteria were: age between 16 and 65 years; the presence of psychotic symptoms as
defined by ICD-10; ability to provide three locators; not involved in harmful or hazardous
drinking (indicated by an AUDIT score>16); no acute physical pathology; no involvement with
criminal justice systems; and no history of psycho-surgery, epilepsy, or head injury. In the four
countries it was legal to smoke tobacco and drink alcohol at the age of 16, and so the term illicit
substance excludes these.
This study was given the necessary ethical and research governance approvals for each of the
four European sites.
Page 3 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
4
Instruments used and selection process
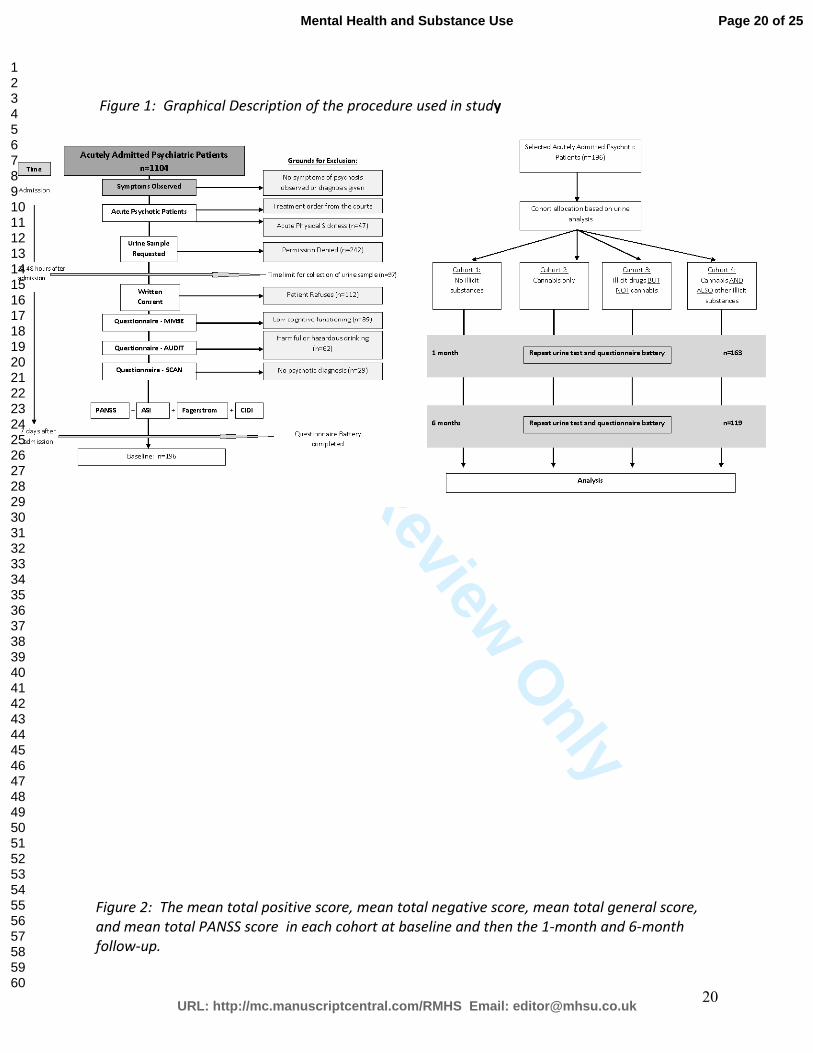
The selection process is outlined in figure 1. The screening instruments were completed within
24 hours of admission. These were the Mini Mental State Examination (MMSE) (Folstein,
Folstein,& McHugh, 1975), Alcohol Use Disorders Identification Test (AUDIT); and the
Schedules for Clinical Assessment in Neuropsychiatry (SCAN) (Bebbington, 1992). All
instruments were administered in the native language of the participant by a researcher trained in
these instruments. Patients with psychotic symptoms were asked for a urine sample within a 48
hour period.
Insert Figure 1 here
The diagnostic instruments were completed within 7 days of admission. This included the
Fagerstrom test for nicotine dependence (Pomerleau et al.,1994), the Positive and Negative
Symptom Severity Scale (PANSS) (Kay, Fizbein & Opler, 1987), the Composite International
Diagnostic Interview (CIDI) (Pull & Wittchen,1991; Wittchen,1994) and the Addiction
Severity Index (Leonhard et al., 2000). These instruments were repeated at 1 and 6 month follow
ups.
Patients were allocated into one of four cohorts depending on their urine tests at baseline. This
was done by automated screening of urine samples by enzyme immunoassay (EMIT) or enzyme-
linked immunosorbent assay (ELISA) to classify any substance present. In the event a positive
finding thin layer (TLC), gas (GC) or liquid (LC) chromatography (Guitton et al., 1993) were
used for confirmation of a specific substance (Simpson et al., 1997).
Page 4 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
5
Those testing negative for all illicit substances (cannabis, amphetamines, cocaine, opiates and
benzodiazepines) were allocated into cohort 1. Those testing positive for cannabis only were
allocated into cohort 2. Those testing positive for illicit substances but not cannabis were
allocated into cohort 3. Those testing positive for cannabis and also other illicit substances were
allocated into cohort 4.
Analyses
Analyses were completed using SPSS, version 18.0. In order to minimise Type 1 error as a
result of multiple testing of effects that could be independent to each other, the significance level
was lowered from p<0.05 to p<0.01.
Repeated measures ANOVA were used to compare changes between baseline, 1 and 6 month
follow up. One-way ANOVA were used when comparing data between cohorts at the same time
point of the study. When comparing the means of only two groupings, t-tests were used in place
of the ANOVA. Chi squares were used to compare categorical data, except where small
numbers did not allow for this when Fishers exact Test was used.
Analyses were completed only on patients who were recruited and followed up to 6 months to
allow comparisons made to be as accurate as possible.
Page 5 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
6
Results
Participants
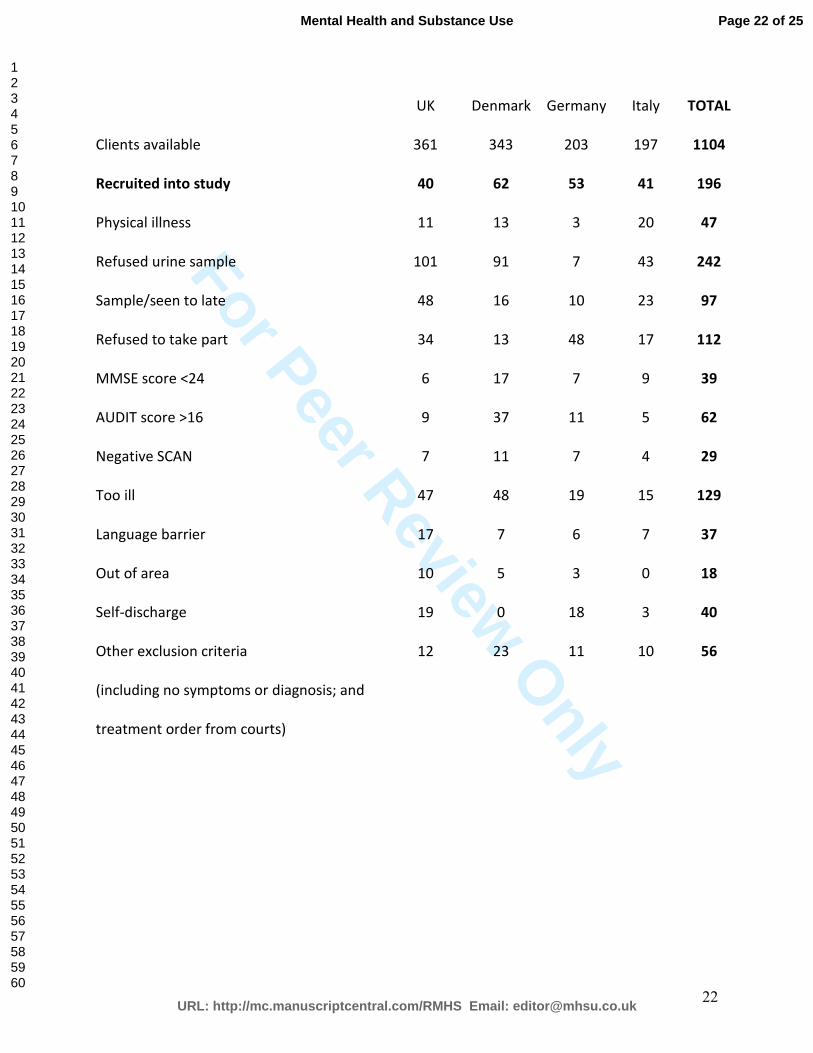
A total of 196 patients were allocated into cohorts at baseline based on urine samples. These were
recruited from a total of 1104 eligible patients who were admitted to the 4 participating centres
during the recruitment period. The level of recruitment was therefore 17.7%. Reasons for non-
participation and exclusion are included in table 1. Further details of the baseline characteristics
of these patients can be found elsewhere (Baldacchino et al., 2009).
Insert Table 1 here
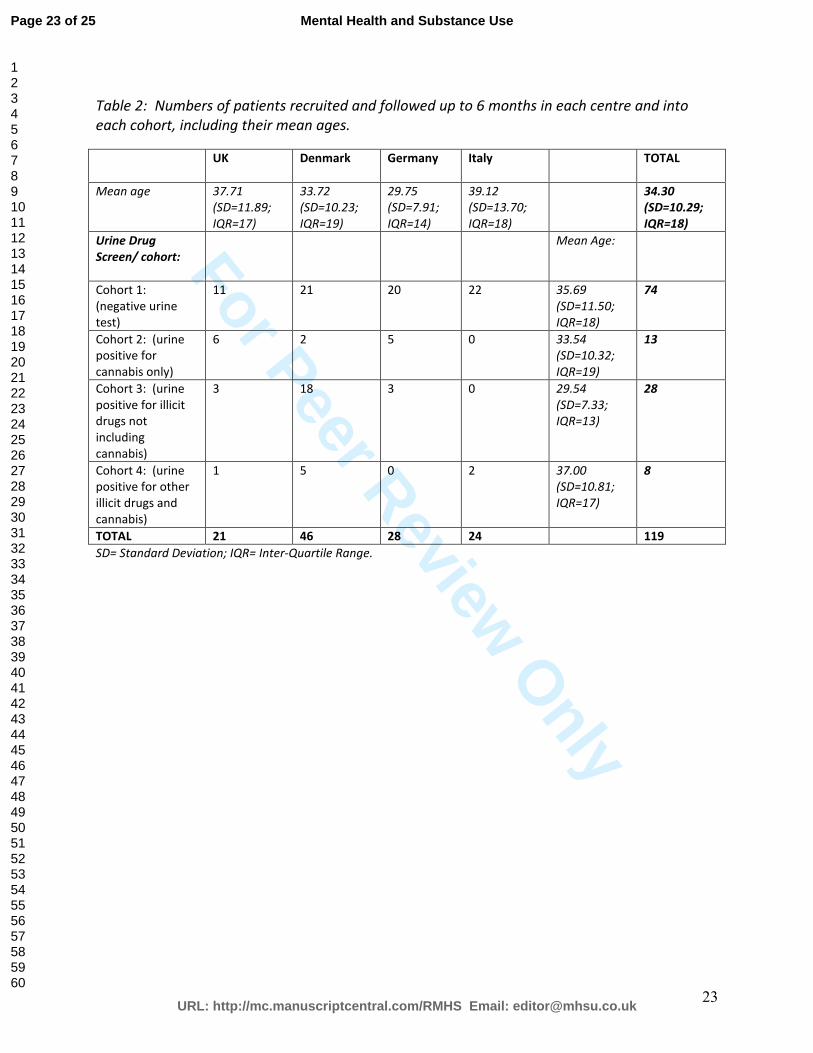
One hundred and nineteen of the original 196 patients were followed up to 6 months (61%). The
numbers of patients recruited in each centre and in each cohort, with their mean ages are
presented in table 2. No significant differences were found between the socio-demographic
characteristics of those patients who were followed up and those who were not.
Insert Table 2 here
Psychopathology
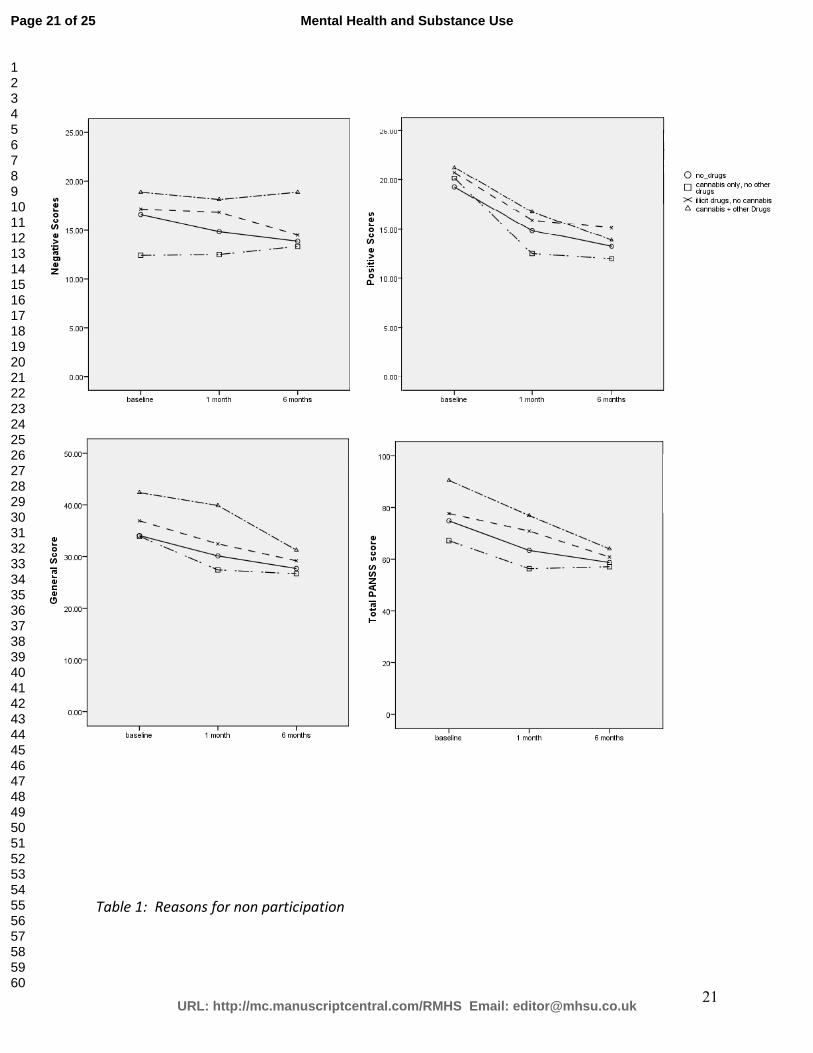
Figure 2 shows the PANSS scores in each cohort over the 3 study time points. No significant
differences were found between the cohorts at baseline in any of the symptoms measured by the
PANSS.
Insert Figure 2 here
Page 6 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
7
At the 1 month follow up there remained no significant differences in the majority of symptoms
between the four cohorts. However, there were significant differences for the symptoms
‘uncooperativeness’ (F(3,113)=4.03, p=0.01) and ‘disorientation’ (F(3,113)=6.72, p<0.001). In
both of these the highest scores were in cohort 4, cannabis and other illicit substances (2.13
(SD=1.13) and 2.13 (SD=1.36) respectively), with the lowest scores in cohort 2, the cannabis
only cohort (1.00 (SD=0.00) and 1.08 (SD=0.29). The scores in cohort 1, no illicit drugs were
1.26 (SD=0.83) and 1.24 (SD=0.59); and in cohort 3, illicit drugs but not cannabis were 1.57
(SD=0.84) and 1.78 (SD=0.95).
At the 6 months follow up there was again no significant differences between the cohorts in the
levels of psychotic symptoms as measured by the PANSS.
Differences in PANSS scores across the study
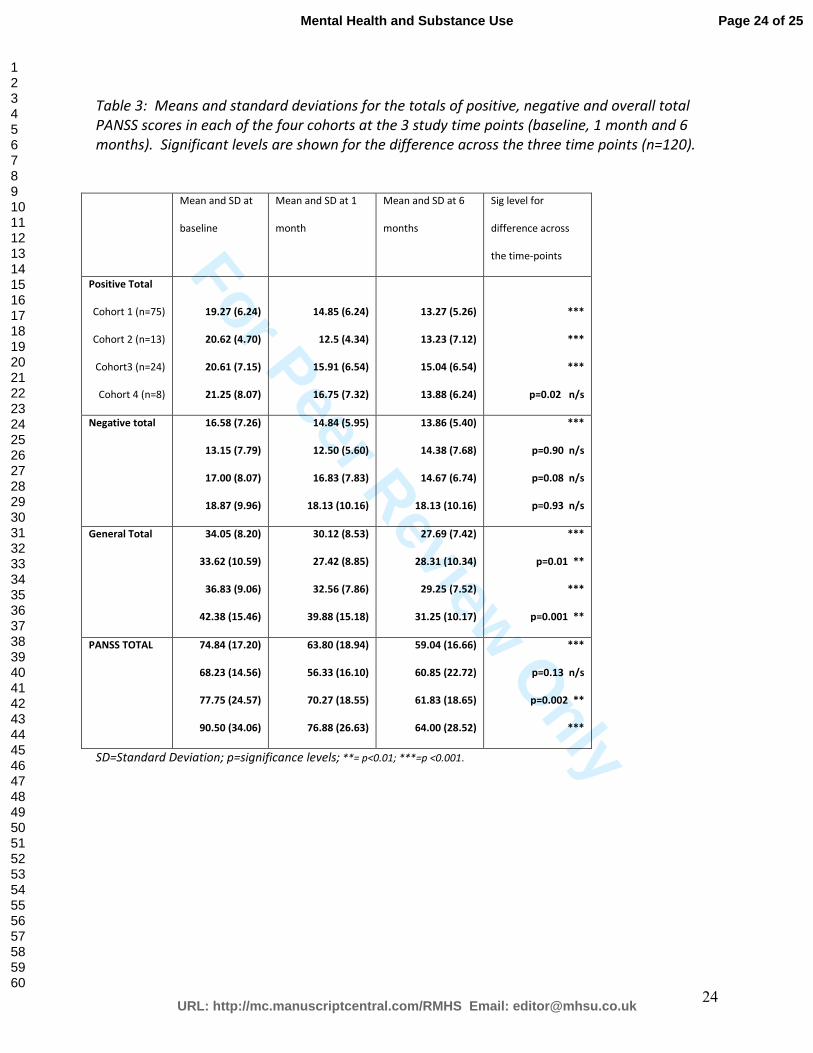
The total PANSS scores decreased across the study in cohorts 1, 3 and 4. This difference was
significant in cohort 1 (F(2, 144)=40.79, p<0.001), cohort 3 (F(2, 40)=7.41, p=0.002), and
cohort 4 (F(2, 14)=17.95, p<0.001), but not cohort 2 (F(2, 22)=2.21, p=0.13).
Refer to Table 3 for the mean total scores for; the PANSS as a whole, the positive symptoms, the
negative symptoms and the general symptoms of patients in each cohort at the different points of
the study.
Insert Table 3 here
Page 7 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
8
Positive Symptoms
The total of positive scores decreased significantly over the 3 points of study (F(2, 230)=74.92,
p<0.001). The level of positive symptoms reduced in all cohorts over the 6 months, the biggest
reduction being between baseline and 1 month. This difference was significant in cohorts 1, 2
and 3 but not in cohort 4, cannabis and other illicit substances (cohort 1; F(2, 146)= 43.52,
p<0.001; cohort 2 F(2, 22)=22.33, p<0.001; cohort 3: F(2, 42)=10.33, p<0.001; cohort 4; F(2,
14)=5.60, p=0.02).
In cohort 1; 6 of the 7 positive symptoms improved significantly (‘delusions’ (p<0.001),
‘conceptual disorganisation’ (p<0.01), ‘hallucinatory behaviour’ (p<0.001), ‘excitement’
(p<0.001), ‘grandiosity’ (p<0.001), and ‘suspiciousness and persecution’ (p<0.001). In cohort 2
those which improved were ‘delusions’ (p<0.001), ‘hallucinatory behaviour’ (p<0.01) and
‘suspiciousness and persecution’ (p<0.001). In cohort 3 the only symptoms improving
significantly over the study were ‘delusions’, and ‘hallucinatory behaviour’ (p<0.001), and
‘excitement’ (p<0.01). In cohort 4 the symptoms which improved significantly were ‘delusions’
(p<0.01) and ‘excitement’ (p<0.01).
Negative Symptoms
The general trend for the negative total across the points of study was a decrease in symptoms.
This was found to differ significantly from baseline to 6 month follow up (F(2, 230)=7.45,
p<0.001). However, the only cohort that individually showed a statistically significant
difference was cohort 1 (F(2, 148)= 8.69, p<0.001). The symptoms which differed in cohort 1
Page 8 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
9
were ‘emotional withdrawal’ (p=0.01), ‘poor rapport’ (p<0.01), and ‘difficulty in abstract
thinking’ (p<0.01).
It should be noted here that although cohort 2 did not differ significantly from the other cohorts
in the levels of negative symptoms it did have lower levels. In comparison to cohort 1 (no drug
use) it had lower levels of negative symptoms even after cohort 1 had made a significant
reduction in levels (see figure 2).
General Symptoms
General scores improved significantly for all patients over the course of the study with an
improvement at each of the follow-up points (F(2, 230)=47.92, p<0.001). Individually all
cohorts also demonstrated significant changes (cohort 1; F(2, 146)= 28.08, p<0.001; cohort 2; (2,
22)=5.64, p=0.01; cohort 3; F(2, 42)= 9.57, p<0.001; cohort 4; F(2, 14)=6.14, p=0.01).
The number of general symptoms showing a significant difference across the points of the study
was greatest in cohort 1 with 6 out of the 16 symptoms. These were ‘anxiety’ (p<0.001),
‘tension’ (p<0.001), ‘depression’ (p<0.001), ‘motor retardation’ (p<0.001), ‘unusual thought
content’ (p<0.001). In cohort 2 no individual general symptoms differed significantly across the
study time points. In cohort 3, 3 out of the 16 general symptoms differed across the points of the
study. These were ‘unusual thought content’ (p<0.001), ‘poor attention’ (p<0.01), and ‘lack of
judgement and insight’ (p<0.001). In cohort 4 no individual general symptom differed
significantly.
Page 9 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
10
Use of illicit substances
At baseline 32.5% of patients in cohort 3 tested positive for opiates with less use of cocaine and
benzodiazepines. This differed from cohort 4 where higher levels of cocaine and amphetamines
were used.
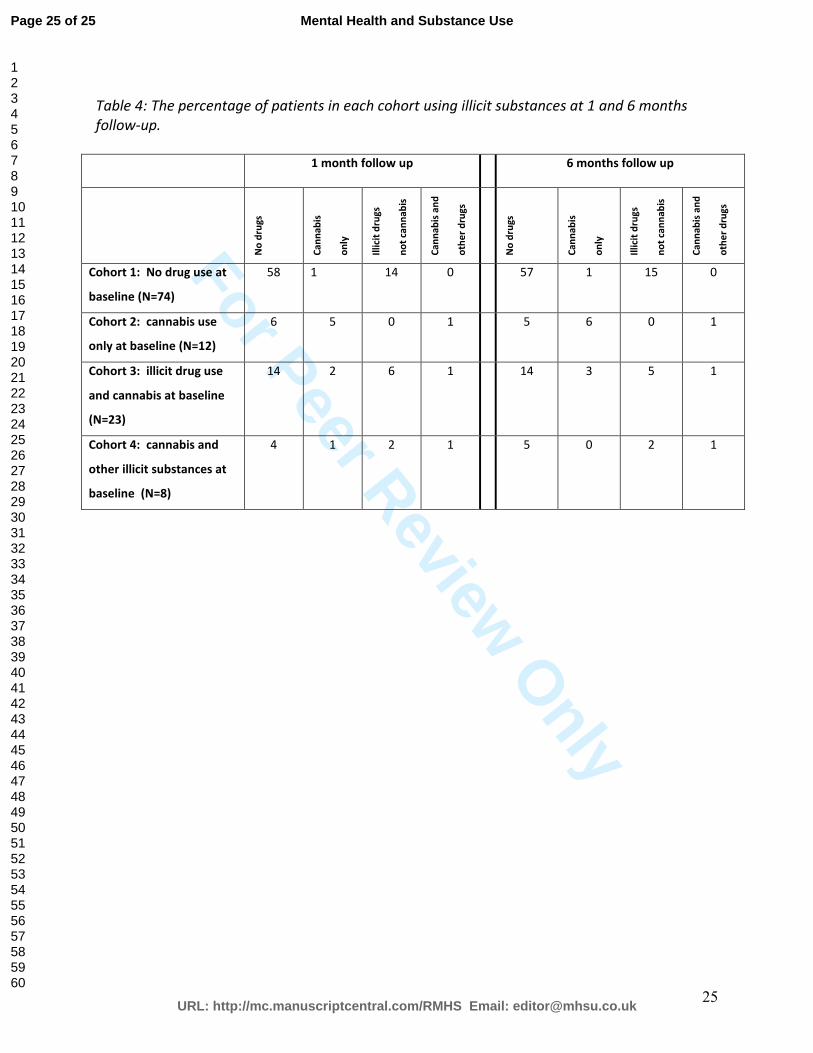
The current illicit substance use by patients at the times of their follow up interviews was tested
by urine analysis (see table 4). In the illicit substance using cohorts, there was a noticeable
reduction in the number of patients testing positive for illegal substances, although it should be
noted that some patients not using drugs at baseline tested positive at follow up.
No differences were found between the socio-demographic characteristics of patients who
changed their drug used patterns and those who did not. These results do, however, show the
potentially transient nature of co-morbidity.
Insert Table 4 here
Discussion
Patients in all four cohorts improved in their levels of psychotic symptoms over the course of the
study. Results from this study suggest that the most notable difference in the outcome of patients
with a diagnosis of psychosis depending on whether or not they use drugs is in the levels of
negative symptoms. A significant improvement in the levels of negative symptoms was only
found in those patients who were not using drugs, despite there being a lack of significant
differences between the cohorts at baseline. There was also a significant improvement in more
Page 10 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
11
positive and general symptoms in patients not using drugs. Cannabis using patients showing an
improvement in the fewest symptoms, but they do tend to have the lowest symptom levels
initially.
Psychopathology
Extreme caution should be used when interpreting the results from this study due to the small
numbers; however some interesting findings seem to be emerging especially with regards to the
levels of negative symptoms.
All cohorts show an improvement in their levels of psychopathological symptoms as indicated
by the PANSS total score with the exception of cohort 2 (cannabis only). Levels of general
symptoms improve significantly in all cohorts at the follow up points. Positive symptoms also
improve in each of the four cohorts, although not significantly in cohort 4 (cannabis and other
illicit substances). However the numbers in this cohort were particularly low (n=8) and the
significance level was nearing significance at p=0.02.
Negative symptoms only improved significantly in cohort 1 (no illicit substances). However, the
level of negative symptoms in cohort 1 were consistently higher than those in cohort 2 (cannabis
only) even after a significant improvement had been made (see figure 2). Interpretation of these
findings are complicated by the fact that a statistically significant difference was not found
between the cohorts at any point of the study, but this is likely to be due to a lack of power owing
to small numbers, especially considering that there is a significant improvement in the levels of
negative symptoms in cohort 1. Lower levels of negative symptoms in psychotic patients using
Page 11 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
12
cannabis reflect previous findings (Bersani et al., 2002; Dubertret et al., 2006; Rottanburg et al.,
1982) which lend support to the idea that there are real differences in the symptoms and recovery
of psychotic patients dependent on their use of illicit substances.
The levels of negative symptoms remained high in those patients who were using other illicit
substances, including those who were using cannabis alongside other substances. This suggest
that cannabis does not provide a protective factor from the negative symptoms of psychosis,
rather there is a difference in the way psychosis manifests in those individuals who are using
cannabis alone.
Drug use by patients at follow-up
Differences in drugs used by patients from baseline to follow-up are noted, but were not taken
into account for the purposes of analysing the differences in the outcomes of the different
cohorts. It is possible that the changes in drug use that do occur at the follow up points of this
study will have some impact on outcome. These findings highlight the fact that co-morbidity of
drug use and psychotic illness is a chronic relapsing condition, making the changing use of illicit
substances a particularly difficult factor to control for.
Limitations of study; methodological dilemmas
This study was designed to provide comprehensive information about the course of illness of co-
morbid patients following admission to an acute psychiatric ward. However, there were some
issues that arose, or, need consideration when interpreting the results.
Page 12 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
13
Firstly, the population being studied is very specific, and while this was to gain as pure a data-set
as possible about this specific patient group it does mean that there is little scope for
generalisation beyond acute psychiatric admissions. Small numbers of patients did not allow for
grouping by country as well as cohort meaning that cultural differences can not be taken into
account which otherwise may have influenced outcome. An issue relating to the cross-cultural
aspect is the differences between service use and provision that may occur in different cultures
(Nilson, Fridell & Griffiths, 2006). Bearing this in mind, interpretation of results should
consider the possibility of these differences, which due to the opportunistic nature of this
research it was not possible to control for. There may have been differences in the treatment
received by participants both on admission and during the follow-up periods. Continued use of
anti-psychotic and anti-depressant medication, or simply inpatient status, at follow up was not
taken into account.
General problems that are evident in identifying a population for this type of study were
applicable, in that the definition of co-morbidity is unclear (Corkery & Baldacchino, 2006;
Crome,2006). In order to provide diagnosis that used standardised and validated measures
providing a consistent diagnostic system across the different centres a combination of measures
were used. This led to some problems as the training of researchers led to delays, as well as
finding measures that were translated and validated in the languages required for this study.
The main weakness of this study is the small numbers recruited. This is not unusual in this
population as they generally have a chaotic life-style and are difficult to follow-up (Corkery &
Baldacchino, 2006) . In this study, rigorous inclusion criteria may have exacerbated this
Page 13 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
14
problem. Studying patients with specific diagnosis, ruling out poor cognitive functioning or
hazardous alcohol use, among other things will mean lower numbers. This problem is difficult
to address, as there is the need to compromise between inclusion criteria and recruitment of
adequate numbers.
Other limiting factors include the lack of monitoring of drug use throughout the follow up period
with only 3 set points of analysis available. This might have shown a change of drug patterns
within the groups and making baseline cohort criteria redundant. Throughout the study period the
study did not monitor treatment care plans including prescribing which might have influenced
the improvement observed in all cohort groups. Given that previous research has found that co-
morbid mental health and substance misuse populations can lead to decreased adherence to
treatment, both drug status and treatment status throughout the study period are important pieces
of information that could help explain the positive result of improved level of psychotic
symptoms (Corkery & Baldacchino, 2006).
Conclusions
The psychopathology and recovery of patients admitted to acute psychiatric wards with
psychosis is likely to be influenced by their drug use on admission. In this study, those using
cannabis had lower levels of negative symptoms, with little change during their recovery period.
Patients not using drug use on admission showed a significant improvement in levels of negative
symptoms by the 6 month follow up, whereas the levels of negative symptoms remained high in
those patients who were using other illicit substances (including those using cannabis alongside
other substances).
Page 14 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
15
Acknowledgements
The authors would like to thank:
• The EU Quality of Life and Management of Living Resources Programme: 1998-2002
(Ref: QLRT-2000-01550) for their funding of this research.
• Researchers in the centres: Billy Boland, Tracy Burrows, Martin Bland, Survjit Cheeta,
Sanjoo Chengappa, Laurence Church, Caterina Criaco, Hamid Ghodse, Rosemary
Jambert-Grey, Ignatius Loubser, Anand Mathilakath, M-C Marelli, Annie McLeod and
Karine Aslanian-MacMillan.
• All the patients who participated in this study and who hopefully sustained their recovery.
References
1 Chaudry, H., Moss ,H., Bashir, A., Suliman,T.(1991). Cannabis psychosis following bhang
ingestion. Br J Addict.,86(9),1075-1081.
2 Arendt,M., Rosenberg, R., Foldager, L., Perto, G., Munk-Jørgensen, P. (2005). Cannabis
induced psychosis and subsequent schizophrenia spectrum disorders: follow up study of
535 incident cases. Br J Psychiatry, 187,510-515.
3 McGuire, P., Jones, P., Harvey, I., Bebbington, P., Toone, B., Lewis, S., et al.(1994).
Cannabis and acute psychosis. Schizophr Res,13,161-168.
4 Zammit, S., Moore, T., Lingford-Hughes, A., Barnes, T., Jones, P., Burke, M., et al.(2008).
Effects of Cannabis Use on Outcomes of Psychotic Disorders: systematic review. The
British Journal of Psychiatry,193,357-563.
Page 15 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
16
5 Degenhardt, L., Tennant, C., Gilmour, S., Schofield, D., Nash, L., Hall, W., et al. (2007).
The temporal dynamics or relationships between cannabis, psychosis and depression
among young adults with psychotic disorders: findings from a 10-month prospective study.
Psychological Medicine, 37,1-8.
6 Ferdinand, R., Sondeijker, F., van der Ende, J., Selton, J.P., Huizink, A., Verhulst,
F.(2005). Cannabis use predicts future psychotic symptoms and vice versa. Addiction, 100,
612-618.
7 Fergusson, D., Horwood, L., Ridder, E.(2005). Tests of causal linkages between cannabis
use and psychotic symptoms.Addiction, 100, 354-366.
8 Verdoux, H., Tournier, M., Cougnard, A.(2005). Impact of substance use on the onset and
course of early psychosis. Schizophr Res, 79, 69-75.
9 Virgo, N., Bennett, G., Higgins, D., Bennett, L., Thomas, P. (2001). The prevalence and
characteristics of co-occurring serious mental illness (SMI) and substance abuse or
dependence in the patients of Adult Mental Health and Addictions Services in Eastern
Dorset. J Mental Health,10(2), 175-188.
10 Dalmau, A., Bergman, B., Brismar, B.(1999). Psychotic Disorders among inpatients with
abuse of cannabis, amphetamine and opiates. Do dopaminergic stimulants facilitate
psychiatric illness? Eur Psychiatry,14,366-371.
11 Grace, R., Shenfield, G., Tennant, C.(2000). Cannabis and Psychosis in acute psychiatric
admissions. Drug and Alcohol Review, 19, 287-290.
Page 16 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
17
12 Kaiser, R., Löhrer, F., Morgan, V., Hambrecht, M.(2005). Changes in the pattern of
substance abuse after the onset of psychosis. Aus NZ J Psychiatr, 39, 467-472.
13 Pencer, A., Addington, J.(2003). Substance use and cognition in early psychosis. J
Psychiatry Neurosci, 28(1),48-54.
14 Sevy, S., Robinson, D., Solloway, S., Alvir, J., Woerner, M., Bilder, R., et al.(2001).
Correlates of substance misuse in patients with first episode schizophrenia and
schizoaffective disorder. Acta Psychiatr Scand, 104(367),374.
15 Grech, A., Van Os, J., Jones, P., Lewis, S., Murray, R.(2005). Cannabis use and outcome of
recent onset psychosis. Eur Psychiat, 20,349-353.
16 Baldacchino, A., Blair, H., Riglietta, M., Tidone, L., Sommer, B., Little, H., et al.(2009).
Drugs and Psychosis Project: a multi-centre European study on comorbidity. Drug and
Alcohol Review, 28,379-389.
17 Folstein, M., Folstein, S., McHugh, P.(1975). 'Mini-mental state': A practical method for
grading the cognitive state of patients for the clinician. J Psychiatry Res, 12,189-198.
18 Bebbington, P. (1992). Welcome to ICD-10 and welcome to SCAN. Soc Psychiatry and
Psychiatric Epidemiol, 27,255-257.
19 Pomerleau, C., Carlton, S., Lutzke, M., Flessland, K., Pomerleau, O.(1994). Reliability of
the Fragerstrom tolerance questionnaire and the Fragerstrom test for Nicotine Dependence.
Addict Behav, 19(1), 33-39.
Page 17 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
18
20 Kay, S., Fizbein, A., Opler, L.(1987). The Positive and Negative Syndrome Scale for
Schizophrenia (PANNS). Schizophr Bull, 13(2), 261-279.
21 Pull, C., Wittchen, H. (1991). CIDI, SCAN and IPDE: structured diagnostic interviews for
ICD-10 and DSM-III-R. Eur Psychiat, 6,277-285.
22 Wittchen, H. (1994).Reliability and validity studies of the WHO-Composite International
Diagnostic Interview (DIDI): A critical review. J Psychiatry Res, 28(1), 57-84.
23 Leonhard, C., Mulvey, K., Gastfriend, D.R., Shwartz, M. (2000).The Addiction Severity
Index - A field study of internal consistency and validity. Journal of Substance Abuse,
Treatment 18(2),129-135.
24 Guitton, J., David, O., Mialon, A., Manchon, M.(1993). Evaluation of an automated liquid
chromatograph permitting toxicologic screening of biological fluids. Ann Clin Biology,
51,611-617.
25 Simpson, D., Brathwaite, R., Jarvie, D., Stewart, M., Walker, S., Watson, I., et al.
(1997).Screening for drugs of abuse (II): Cannabinoids, lysergic acid diethylamide,
buprenorphine, methadone, barbiturates, benzodiazepines and other drugs. Ann Clin
Biochem, 34,460-510.
26 Bersani, G., Orlandi, V., Kotzalidis, G., Pancheri, P.(2002). Cannabis and schizophrenia:
Impact on onset, course, psychopathology and outcomes. Eur Arch Psychiatry Clin
Neurosci, 252, 86-92.
Page 18 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
19
27 Dubertret, C., Bidard, I., Ades, J., Gorwood, P.(2006). Lifetime positive symptoms in
patients with schizophrenia and cannabis abuse are partically explained by co-morbid
addiction. Schizophr Res, 86,284-90.
28 Rottanburg, D., Ben-Arie, O., Robins, A., Teggin, A., Elk, R.(1982). Cannabis-Associated
Psyhosis with Hypomanic Features. Lancet,18;320,1364-1366.
29 Nilson, M., Fridell, M., Griffiths, P. (2006) Definition and Classification in comorbidity.
In: Corkery J, Baldacchino A, editors. European Collaborating Centres on Addiction
Studies (ECCAS) Monograph Series 4: Co-morbidity: Perspectives Across Europe.
ECCAS;. p. 349-61.
30 Corkery, J., Baldacchino, A.(2006). Definition and Classification in co-morbidity. In:
Corkery J, Baldacchino A, editors. European Collaborating Centres in Addiction Studies
(ECCAS) Monograph Series 4: Co-morbidity: Perspectives across Europe. ECCAS. p. 3-
42.
31 Crome I. An epidemiological perspective of psychiatric co-morbidity and substance
misuse: the UK experience/example. In: Corkery J, Baldacchino A, editors. European
Collaborating Centres in Addiction Studies (ECCAS) Monograph Series 4: Co-morbidity:
Perspectives Across Europe. ECCAS; 2006. p. 43-58.
Page 19 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
20
Figure 1: Graphical Description of the procedure used in study
Figure 2: The mean total positive score, mean total negative score, mean total general score,
and mean total PANSS score in each cohort at baseline and then the 1-month and 6-month
follow-up.
Page 20 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
21
Table 1: Reasons for non participation
Page 21 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
22
UK Denmark Germany Italy TOTAL
Clients available 361 343 203 197 1104
Recruited into study 40 62 53 41 196
Physical illness 11 13 3 20 47
Refused urine sample 101 91 7 43 242
Sample/seen to late 48 16 10 23 97
Refused to take part 34 13 48 17 112
MMSE score <24 6 17 7 9 39
AUDIT score >16 9 37 11 5 62
Negative SCAN 7 11 7 4 29
Too ill 47 48 19 15 129
Language barrier 17 7 6 7 37
Out of area 10 5 3 0 18
Self-discharge 19 0 18 3 40
Other exclusion criteria
(including no symptoms or diagnosis; and
treatment order from courts)
12 23 11 10 56
Page 22 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
23
Table 2: Numbers of patients recruited and followed up to 6 months in each centre and into
each cohort, including their mean ages.
SD= Standard Deviation; IQR= Inter-Quartile Range.
UK Denmark Germany Italy TOTAL
Mean age 37.71
(SD=11.89;
IQR=17)
33.72
(SD=10.23;
IQR=19)
29.75
(SD=7.91;
IQR=14)
39.12
(SD=13.70;
IQR=18)
34.30
(SD=10.29;
IQR=18)
Urine Drug
Screen/ cohort:
Mean Age:
Cohort 1:
(negative urine
test)
11 21 20 22 35.69
(SD=11.50;
IQR=18)
74
Cohort 2: (urine
positive for
cannabis only)
6 2 5 0 33.54
(SD=10.32;
IQR=19)
13
Cohort 3: (urine
positive for illicit
drugs not
including
cannabis)
3 18 3 0 29.54
(SD=7.33;
IQR=13)
28
Cohort 4: (urine
positive for other
illicit drugs and
cannabis)
1 5 0 2 37.00
(SD=10.81;
IQR=17)
8
TOTAL 21 46 28 24 119
Page 23 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
24
Table 3: Means and standard deviations for the totals of positive, negative and overall total
PANSS scores in each of the four cohorts at the 3 study time points (baseline, 1 month and 6
months). Significant levels are shown for the difference across the three time points (n=120).
Mean and SD at
baseline
Mean and SD at 1
month
Mean and SD at 6
months
Sig level for
difference across
the time-points
Positive Total
Cohort 1 (n=75)
Cohort 2 (n=13)
Cohort3 (n=24)
Cohort 4 (n=8)
19.27 (6.24)
20.62 (4.70)
20.61 (7.15)
21.25 (8.07)
14.85 (6.24)
12.5 (4.34)
15.91 (6.54)
16.75 (7.32)
13.27 (5.26)
13.23 (7.12)
15.04 (6.54)
13.88 (6.24)
***
***
***
p=0.02 n/s
Negative total 16.58 (7.26)
13.15 (7.79)
17.00 (8.07)
18.87 (9.96)
14.84 (5.95)
12.50 (5.60)
16.83 (7.83)
18.13 (10.16)
13.86 (5.40)
14.38 (7.68)
14.67 (6.74)
18.13 (10.16)
***
p=0.90 n/s
p=0.08 n/s
p=0.93 n/s
General Total 34.05 (8.20)
33.62 (10.59)
36.83 (9.06)
42.38 (15.46)
30.12 (8.53)
27.42 (8.85)
32.56 (7.86)
39.88 (15.18)
27.69 (7.42)
28.31 (10.34)
29.25 (7.52)
31.25 (10.17)
***
p=0.01 **
***
p=0.001 **
PANSS TOTAL 74.84 (17.20)
68.23 (14.56)
77.75 (24.57)
90.50 (34.06)
63.80 (18.94)
56.33 (16.10)
70.27 (18.55)
76.88 (26.63)
59.04 (16.66)
60.85 (22.72)
61.83 (18.65)
64.00 (28.52)
***
p=0.13 n/s
p=0.002 **
***
SD=Standard Deviation; p=significance levels; **= p<0.01; ***=p <0.001.
Page 24 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
25
Table 4: The percentage of patients in each cohort using illicit substances at 1 and 6 months
follow-up.
1 month follow up 6 months follow up
No
dru
gs
Ca
nn
ab
is
on
ly
Illi
cit
dru
gs
no
t ca
nn
ab
is
Ca
nn
ab
is a
nd
oth
er
dru
gs
No
dru
gs
Ca
nn
ab
is
on
ly
Illi
cit
dru
gs
no
t ca
nn
ab
is
Ca
nn
ab
is a
nd
oth
er
dru
gs
Cohort 1: No drug use at
baseline (N=74)
58 1 14 0 57 1
15
0
Cohort 2: cannabis use
only at baseline (N=12)
6
5
0 1
5
6
0 1
Cohort 3: illicit drug use
and cannabis at baseline
(N=23)
14 2
6
1
14 3
5
1
Cohort 4: cannabis and
other illicit substances at
baseline (N=8)
4
1 2
1 5 0 2
1
Page 25 of 25
URL: http://mc.manuscriptcentral.com/RMHS Email: [email protected]
Mental Health and Substance Use
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Related Documents



![[Beyond] morbid (aesthetic) symptoms](https://static.cupdf.com/doc/110x72/62a9fb4db1576f77d233fc5d/beyond-morbid-aesthetic-symptoms.jpg)







