Clinical Immunology Laboratory Handbook Version 14 01/07/15 Department of Biochemistry and Immunology Addenbrooke’s Hospital Cambridge The information contained within this document is subject to regular review, therefore , please ensure that the latest version of this handbook is referred to, when required . Version Number 14 Date of Issue 01.07.15 Review Interval Annual Document History Next Review Due: 01/07/2016 Version Number Issue Date Version Number Issue Date 2005 05/12/05 2011 v8 04/07/11 1.1 03/05/06 2011 v9 13/10/11 2008 v.1 15/03/08 2012 v10 05/01/12 2008 v.2 06/09/08 2012v11 26/06/12 2009 v.1 19/08/09 2013v12 20/05/13 2009 v.2 02/10/09 2014v13 04/04/14 2010 v.1 20/01/10 2015v14 01/07/15 2010 v.2 17/03/10 2010 v.3 08/07/10 2010 v.4 09/07/10 2010 v.5 03/09/10 2011 v.6 11/01/11 2011 v7 01/05/11 Document Location Addenbrooke’s Hospital Intranet Pages( Connect) The Pathology Partnership Website Document Ownership Senior Executive, Dept of Clinical Biochemistry and Immunology

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Clinical Immunology Laboratory Handbook
Version 14 01/07/15
Department of Biochemistry and Immunology
Addenbrooke’s Hospital Cambridge
The information contained within this document is subject to regular review, therefore ,
please ensure that the latest version of this handbook is referred to, when required.
Version Number 14
Date of Issue 01.07.15
Review Interval Annual
Document History
Next Review Due: 01/07/2016
Version
Number
Issue
Date
Version
Number
Issue
Date
2005 05/12/05 2011 v8 04/07/11
1.1 03/05/06 2011 v9 13/10/11
2008 v.1 15/03/08 2012 v10 05/01/12
2008 v.2 06/09/08 2012v11 26/06/12
2009 v.1 19/08/09 2013v12 20/05/13
2009 v.2 02/10/09 2014v13 04/04/14
2010 v.1 20/01/10 2015v14 01/07/15
2010 v.2 17/03/10
2010 v.3 08/07/10
2010 v.4 09/07/10
2010 v.5 03/09/10
2011 v.6 11/01/11
2011 v7 01/05/11
Document Location Addenbrooke’s Hospital Intranet Pages( Connect)
The Pathology Partnership Website
Document Ownership Senior Executive, Dept of Clinical Biochemistry
and Immunology
Contact Information
Telephone numbers – Addenbrooke’s extension number and (number for outside callers)
Laboratory Service
Results 03001032220 [email protected]
General enquiries 2511 (01223 216511)
Consultant Immunologist Dr D S Kumararatne
254256 (01223 254256) mobile 07590485799
Consultant Immunologist Dr H. Baxendale
3159(Monday & Friday) 01223 217159
Consultant Immunologist(locum) Dr S. Pereira
3159 (01223 217159) mobile 077989 14734
Immunology Specialist Lead Mr Graham Wood
3361 (01223 217361) [email protected]
Specialist Registrars 2618 (01223 216618) bleep 154- 406
Duty Doctor 07949 131990 [email protected]
PA To Dr.Kumararatne 6830 (01223 586830)
Safehaven Fax 3794 (01223 217794)
Allergy and Clinical Immunology Service
Director Dr P Ewan Special interest: Allergy & Clinical Immunology
3177 (01223 217777)
Consultant Immunologist, Dr D S Kumararatne Special interest: Immunodeficiency.
3166 (01223 217166) mobile 07740 762829
Consultant in Allergy and Asthma, Dr S Nasser Special interest: allergy, asthma and rhinitis
6978 (01223 586978)
Specialist Nurse Practitioners: 2431 (01223 216431) bleep 152-829
Appointments 2646 (01223 216646)

Introduction
The laboratory part of The Pathology Partnership is based at Addenbrooke’s hospital Cambridge University NHS Foundation Trust, and provides a comprehensive centralised Immunology service for partner Trusts, local GP’s and to other hospitals within the Eastern Region, and across the U.K. It specialises in the diagnosis and monitoring of patients with suspected or confirmed immunodeficiencies, autoimmune diseases, allergy and inflammatory states. It runs a wide range of assays including highly specialised cell function tests. We also carry out a wide range of specialised assays for hospitals outside the region. The medical staff, provide a clinical consultative service for patients with possible or confirmed immunodeficiencies and also provide a specialist care for the treatment of antibody deficient patients. Dr. P.Ewan and Dr.S.Nasser conduct clinics for patients with allergic diseases..
Hours of Service The lab is open Monday to Saturday 08.00- 20.00 hr. Urgent Requests Including Out of Hours Few tests performed by the laboratory are required clinically on an urgent out-of-hours basis. Exceptionally, when circumstances justify a more rapid result, the request should be made personally to the Consultant Immunologist.Outside normal working hours contact is via the hospital switchboard 01223 245151 Medical advice can be obtained from the Consultant Immunologist or Specialist Registrar.
SAMPLE REQUIREMENTS Serum Samples Most tests are performed on serum separated at room temperature. The exceptions are listed below. For serum, blood should be collected in a plain brown top gel tube with no anticoagulant . In most cases samples should be sent to the main pathology sample reception area level 2(external) or level 4 (internal) of the laboratory block at Addenbrookes Hospita, by porter,courier or hospital transport. Serum samples can also be sent by first class post to Clinical Immunology, Box 109, Cambridge University Hospitals NHS Foundation Trust, Hills Road, Cambridge CB2 OQQ or Hayes DX(6050105 Camb 90 CB) Lymphocyte Phenotyping Studies These are performed on a 2.7 ml EDTA (Monovette) sample Neutrophil Function Studies Neutrophil oxidative burst DHR tests are performed on a 2.7 ml EDTA (Monovette) sample taken directly to the laboratory or transported to arrive in the laboratory within 4 hours of collection. Neutrophil tests are time consuming, and can only be done on Monday to Friday if received before 2.00 pm.. Quantiferon TB Gold(Interferon gamma release assay-IGRA) Adults and children: 1ml of blood must be drawn directly into each of the three QuantiFERON-GOLD tubes in order, which must be all labelled with appropriate patient identifying information. (1) Nil control (GREY TOP) (2) TB Antigen (RED TOP) (3) Mitogen Control (PURPLE CAP) (Collection tubes available from outpatients Phlebotomy and directly from the Immunology laboratory) Samples must be incubated at 37º c within 16 hrs of collection, and must be kept at room temperature prior to this. Please contact the laboratory for further information if requesting test from non-Addenbrookes locations. Cytokine studies Please send from Patient and from a healthy control: 5-10 ml Li-heparin blood (3 ml from very small children) 2.7 ml Edta-blood 1-2 ml Serum/clotted (not for very small children ) Samples must be sent by courier at ambient temperature (please do not cool and avoid overheating) to: Dr Rainer Doffinger PhD FRCPath Department of Clinical Biochemistry and Immunology Level E4, Box 109 Addenbrooke’s Hospital Cambridge University Hospitals NHS Foundation Trust Hills Road, Cambridge CB2 0QQ, UK Tel (Office): +44 (0) 1223 217441 (x3441) Tel (Lab): +44 (0) 1223 348145 (x58145) Fax: +44 (0) 1223 217794 Email: [email protected] for same or next day delivery to arrive ideally not later than on a Thursday (exceptions after discussion possible)
Cryoglobulins If cryoglobulins are suspected in autoimmune rheumatoid disorders, a 10 ml blood sample should be collected in a pre-warmed plain white Monovette tube and placed immediately into a vacuum flask
containing water at about 37oC. The sample should be immediately delivered to the Clinical Immunology Laboratory during normal working hours (before 18.00 hr). Please contact the laboratory for further information if requesting test from non-Addenbrookes locations Immunoglobulins Routine tests for total serum IgG, IgA and IgM are performed in the Clinical Biochemistry.Tests for IgG subclasses, IgE, and very low immuno-globulins in hypogammaglobulinaemia are performed in the Clinical Immunology laboratory. Functional Complement Studies including Functional C1 inhibitor Blood taken at Addenbrooke’s Hospital for these assays should reach the laboratory within 30 minutes of being taken and labelled as being urgent. (Do not rely on routine collections!) It should then be separated and frozen to a temperature of at least -40oC within a further 30 minutes. External laboratories must also ensure correct collection of the blood and arrange for it to reach this centre while still deep-frozen. If these procedures are not followed then abnormal low values could be due to in vitro degradation. Functional C1 inhibitor assays should only be performed after initial screening for immunochemical C1 inhibitor concentration in cases where there is a documented normal value of inhibitor but the C4 is low.
Mast Cell Tryptase Blood taken for Mast Cell Tryptase levels should be centrifuged and the serum separated as soon as possible, preferably within 3 hours of venesection.(If the blood is collected into gel separator type tubes centrifugation alone is sufficient) The separated serum or spun tubes should be kept at 4oC and sent to Addenbrookes Immunology. If the samples will not reach Immunology at Addenbrookes within 5 days then separated serum should be frozen at -20 oC or below and then dispatched in a frozen state. If the sample(s) have been taken as part of an anaphylactic/anaesthetic reaction investigation then it is vitally important that sample time and dates are accurately recorded on both sample and request Urine Requests for Bence Jones protein require a 20ml aliquot of urine in a universal container (NO preservative). Storage of Specimens
Sera are stored at 4○C, other than functional complement samples, and retained for about 1month before disposal. If further tests are required on a patient in the light of earlier results, it may be possible to save the inconvenience of a repeat venesection for the patient by contacting the laboratory and arranging further tests on the stored serum. Specimens for cellular immunology tests cannot be retained and are useless after the time of the initial test.

Reporting of Results Reports are issued electronically or printed on paper, when all the tests on a specimen have been completed. Further reports may be issued if other, less frequently performed assays have also been requested. Unexpected or grossly abnormal results will be telephoned to the requesting physician whenever possible. Interpretation of the results of specialised assays will be added but if additional information is required please call the immunology duty doctor who will be pleased to help. Clinical Referrals Please contact the Consultant (Direct line 01223 217166 or ext. 3166. Secretary: 01223 586830) to arrange for a Clinical Immunologist to see a patient. Patients admitted to Addenbrooke’s Hospital under other consultants can be assessed after making a referral in writing or by telephoning. Out patient referrals may be made, by writing or by telephoning (indicating the degree of urgency) to the Consultant.
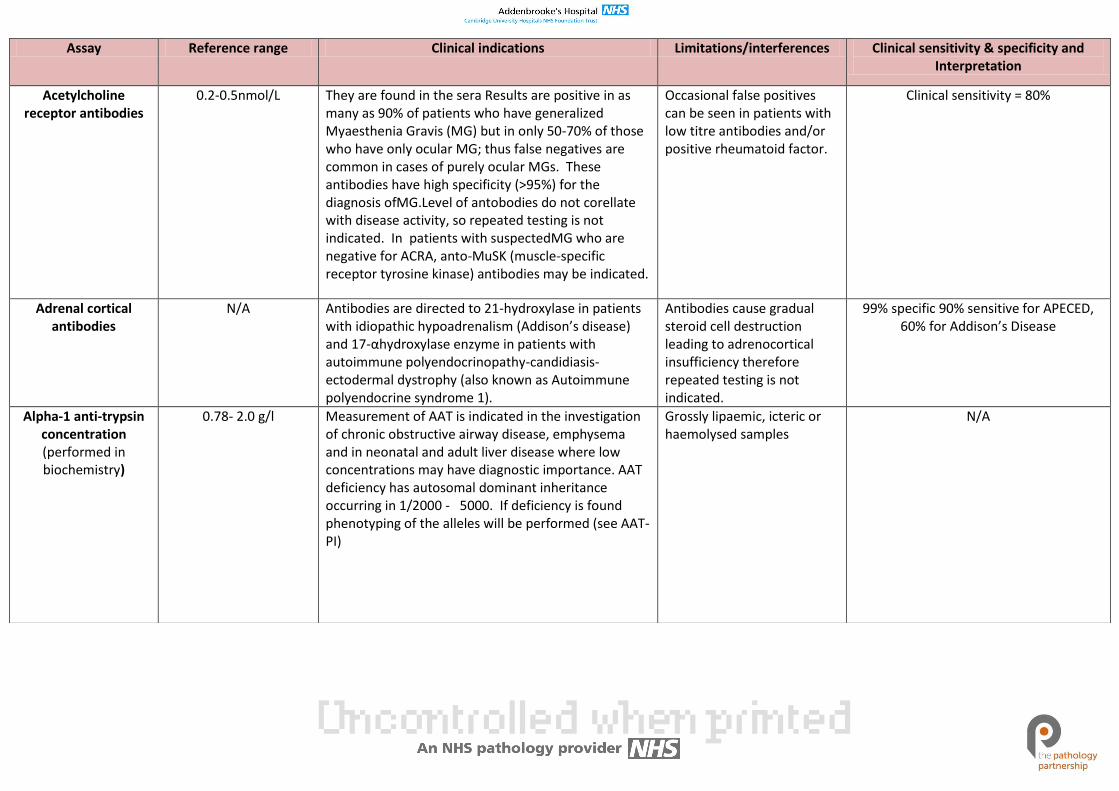
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
Acetylcholine receptor antibodies
0.2-0.5nmol/L They are found in the sera Results are positive in as many as 90% of patients who have generalized Myaesthenia Gravis (MG) but in only 50-70% of those who have only ocular MG; thus false negatives are common in cases of purely ocular MGs. These antibodies have high specificity (>95%) for the diagnosis ofMG.Level of antobodies do not corellate with disease activity, so repeated testing is not indicated. In patients with suspectedMG who are negative for ACRA, anto-MuSK (muscle-specific receptor tyrosine kinase) antibodies may be indicated.
Occasional false positives can be seen in patients with low titre antibodies and/or positive rheumatoid factor.
Clinical sensitivity = 80%
Adrenal cortical antibodies
N/A Antibodies are directed to 21-hydroxylase in patients with idiopathic hypoadrenalism (Addison’s disease) and 17-αhydroxylase enzyme in patients with autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy (also known as Autoimmune polyendocrine syndrome 1).
Antibodies cause gradual steroid cell destruction leading to adrenocortical insufficiency therefore repeated testing is not indicated.
99% specific 90% sensitive for APECED, 60% for Addison’s Disease
Alpha-1 anti-trypsin concentration (performed in biochemistry)
0.78- 2.0 g/l Measurement of AAT is indicated in the investigation of chronic obstructive airway disease, emphysema and in neonatal and adult liver disease where low concentrations may have diagnostic importance. AAT deficiency has autosomal dominant inheritance occurring in 1/2000 - 5000. If deficiency is found phenotyping of the alleles will be performed (see AAT-PI)
Grossly lipaemic, icteric or haemolysed samples
N/A
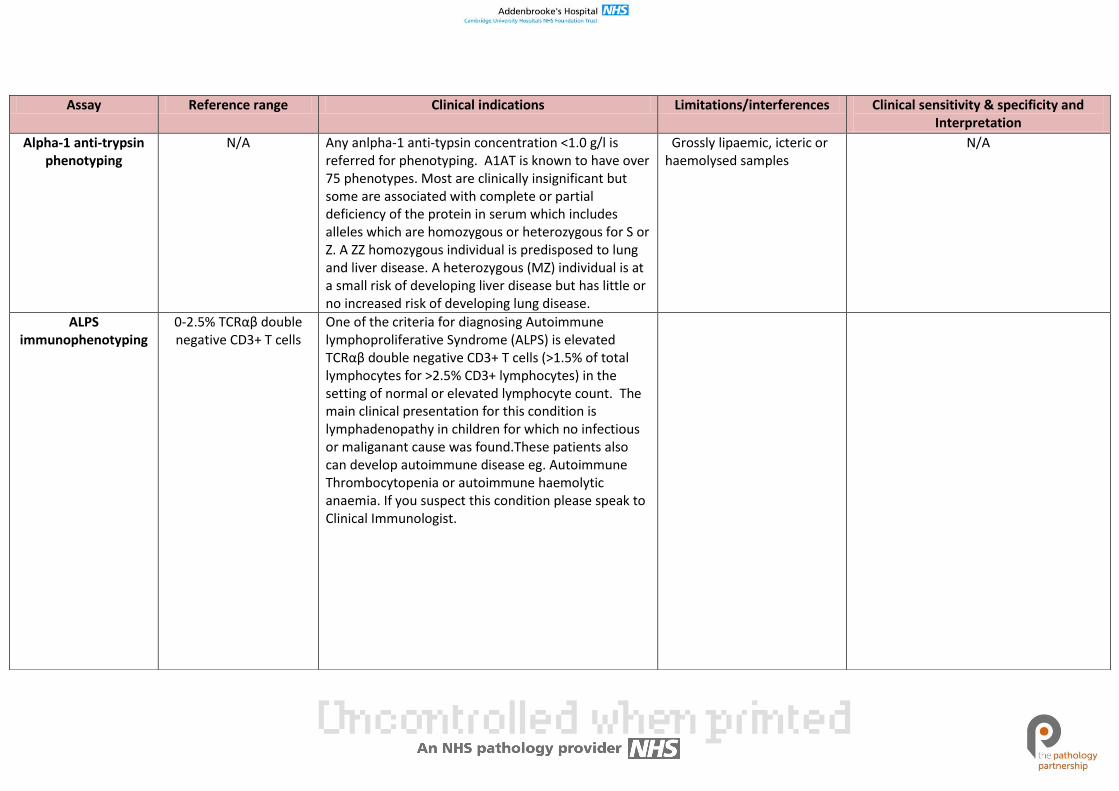
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
Alpha-1 anti-trypsin phenotyping
N/A Any anlpha-1 anti-typsin concentration <1.0 g/l is referred for phenotyping. A1AT is known to have over 75 phenotypes. Most are clinically insignificant but some are associated with complete or partial deficiency of the protein in serum which includes alleles which are homozygous or heterozygous for S or Z. A ZZ homozygous individual is predisposed to lung and liver disease. A heterozygous (MZ) individual is at a small risk of developing liver disease but has little or no increased risk of developing lung disease.
Grossly lipaemic, icteric or haemolysed samples
N/A
ALPS immunophenotyping
0-2.5% TCRαβ double negative CD3+ T cells
One of the criteria for diagnosing Autoimmune lymphoproliferative Syndrome (ALPS) is elevated TCRαβ double negative CD3+ T cells (>1.5% of total lymphocytes for >2.5% CD3+ lymphocytes) in the setting of normal or elevated lymphocyte count. The main clinical presentation for this condition is lymphadenopathy in children for which no infectious or maliganant cause was found.These patients also can develop autoimmune disease eg. Autoimmune Thrombocytopenia or autoimmune haemolytic anaemia. If you suspect this condition please speak to Clinical Immunologist.
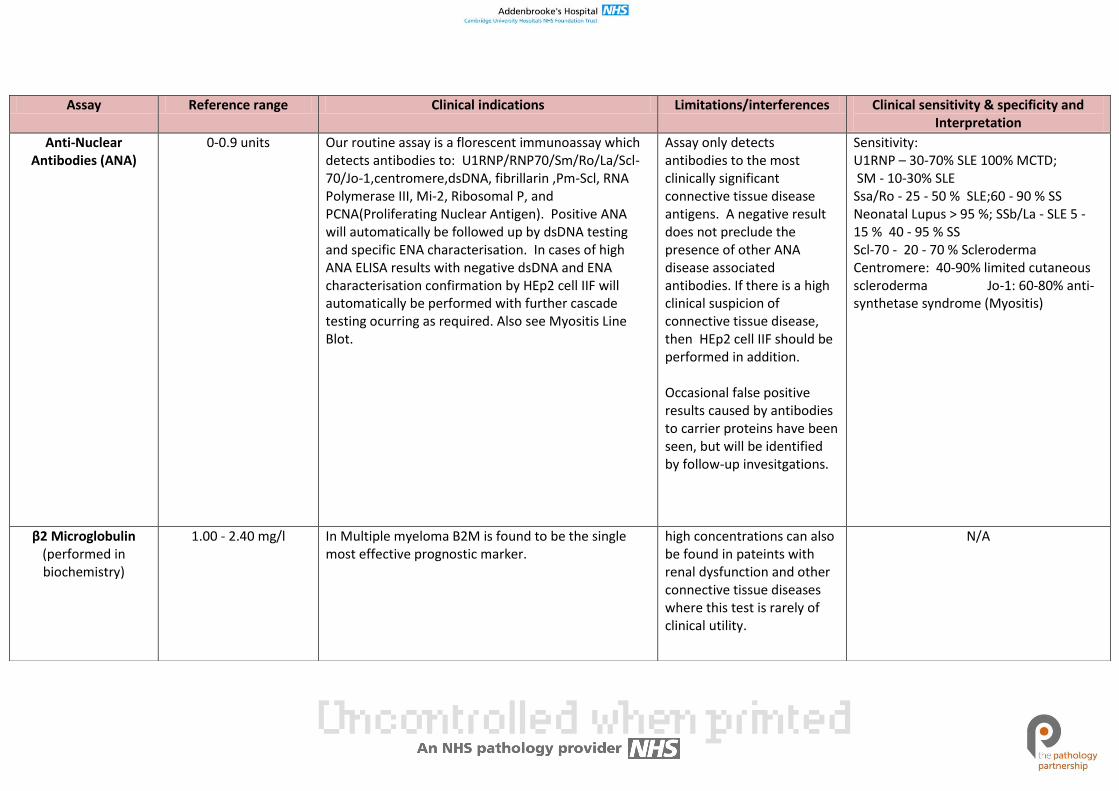
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
Anti-Nuclear Antibodies (ANA)
0-0.9 units Our routine assay is a florescent immunoassay which detects antibodies to: U1RNP/RNP70/Sm/Ro/La/Scl-70/Jo-1,centromere,dsDNA, fibrillarin ,Pm-Scl, RNA Polymerase III, Mi-2, Ribosomal P, and PCNA(Proliferating Nuclear Antigen). Positive ANA will automatically be followed up by dsDNA testing and specific ENA characterisation. In cases of high ANA ELISA results with negative dsDNA and ENA characterisation confirmation by HEp2 cell IIF will automatically be performed with further cascade testing ocurring as required. Also see Myositis Line Blot.
Assay only detects antibodies to the most clinically significant connective tissue disease antigens. A negative result does not preclude the presence of other ANA disease associated antibodies. If there is a high clinical suspicion of connective tissue disease, then HEp2 cell IIF should be performed in addition. Occasional false positive results caused by antibodies to carrier proteins have been seen, but will be identified by follow-up invesitgations.
Sensitivity: U1RNP – 30-70% SLE 100% MCTD; SM - 10-30% SLE Ssa/Ro - 25 - 50 % SLE;60 - 90 % SS Neonatal Lupus > 95 %; SSb/La - SLE 5 - 15 % 40 - 95 % SS Scl-70 - 20 - 70 % Scleroderma Centromere: 40-90% limited cutaneous scleroderma Jo-1: 60-80% anti-synthetase syndrome (Myositis)
β2 Microglobulin (performed in biochemistry)
1.00 - 2.40 mg/l
In Multiple myeloma B2M is found to be the single most effective prognostic marker.
high concentrations can also be found in pateints with renal dysfunction and other connective tissue diseases where this test is rarely of clinical utility.
N/A
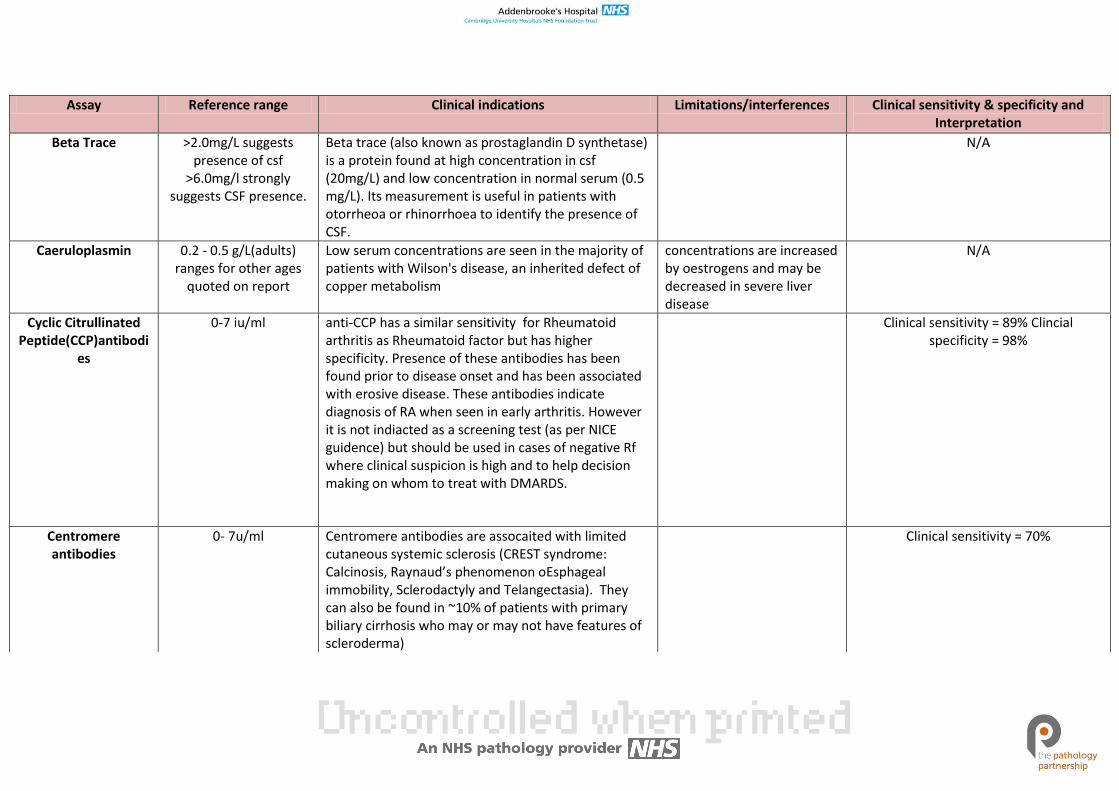
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
Beta Trace >2.0mg/L suggests presence of csf
>6.0mg/l strongly suggests CSF presence.
Beta trace (also known as prostaglandin D synthetase) is a protein found at high concentration in csf (20mg/L) and low concentration in normal serum (0.5 mg/L). Its measurement is useful in patients with otorrheoa or rhinorrhoea to identify the presence of CSF.
N/A
Caeruloplasmin 0.2 - 0.5 g/L(adults) ranges for other ages
quoted on report
Low serum concentrations are seen in the majority of patients with Wilson's disease, an inherited defect of copper metabolism
concentrations are increased by oestrogens and may be decreased in severe liver disease
N/A
Cyclic Citrullinated Peptide(CCP)antibodi
es
0-7 iu/ml anti-CCP has a similar sensitivity for Rheumatoid arthritis as Rheumatoid factor but has higher specificity. Presence of these antibodies has been found prior to disease onset and has been associated with erosive disease. These antibodies indicate diagnosis of RA when seen in early arthritis. However it is not indiacted as a screening test (as per NICE guidence) but should be used in cases of negative Rf where clinical suspicion is high and to help decision making on whom to treat with DMARDS.
Clinical sensitivity = 89% Clincial specificity = 98%
Centromere antibodies
0- 7u/ml Centromere antibodies are assocaited with limited cutaneous systemic sclerosis (CREST syndrome: Calcinosis, Raynaud’s phenomenon oEsphageal immobility, Sclerodactyly and Telangectasia). They can also be found in ~10% of patients with primary biliary cirrhosis who may or may not have features of scleroderma)
Clinical sensitivity = 70%
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
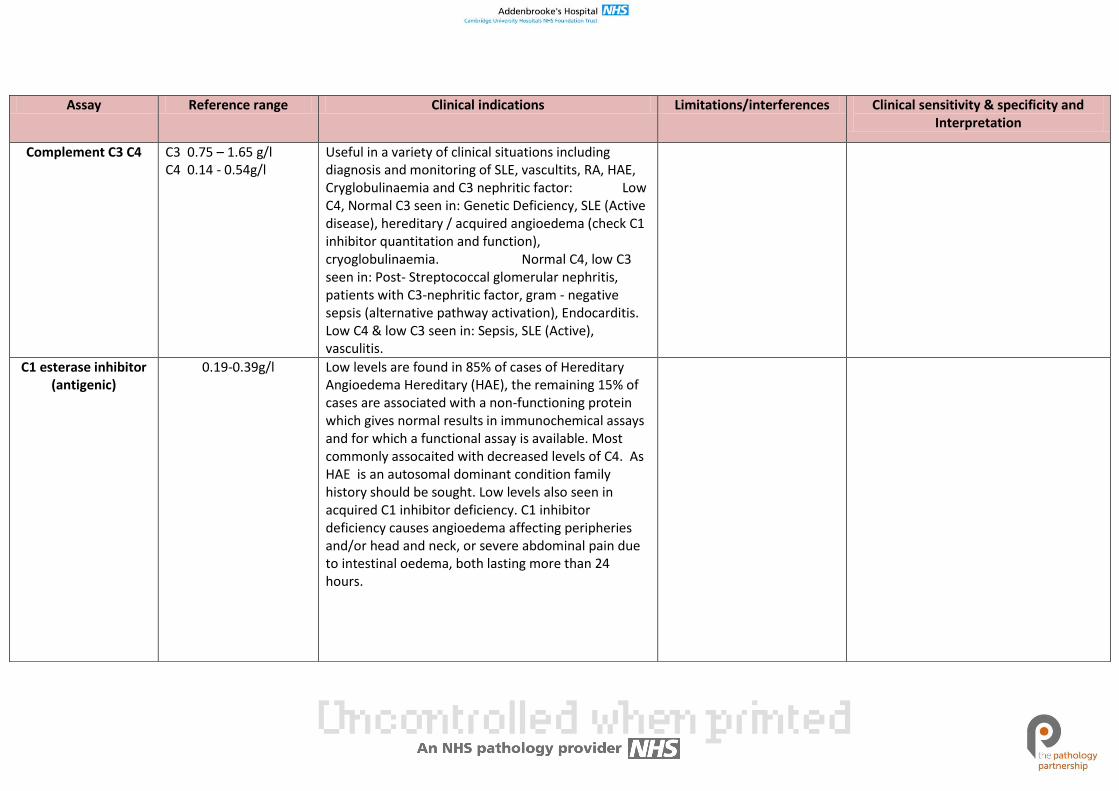
Complement C3 C4 C3 0.75 – 1.65 g/l C4 0.14 - 0.54g/l
Useful in a variety of clinical situations including diagnosis and monitoring of SLE, vascultits, RA, HAE, Cryglobulinaemia and C3 nephritic factor: Low C4, Normal C3 seen in: Genetic Deficiency, SLE (Active disease), hereditary / acquired angioedema (check C1 inhibitor quantitation and function), cryoglobulinaemia. Normal C4, low C3 seen in: Post- Streptococcal glomerular nephritis, patients with C3-nephritic factor, gram - negative sepsis (alternative pathway activation), Endocarditis. Low C4 & low C3 seen in: Sepsis, SLE (Active), vasculitis.
C1 esterase inhibitor (antigenic)
0.19-0.39g/l Low levels are found in 85% of cases of Hereditary Angioedema Hereditary (HAE), the remaining 15% of cases are associated with a non-functioning protein which gives normal results in immunochemical assays and for which a functional assay is available. Most commonly assocaited with decreased levels of C4. As HAE is an autosomal dominant condition family history should be sought. Low levels also seen in acquired C1 inhibitor deficiency. C1 inhibitor deficiency causes angioedema affecting peripheries and/or head and neck, or severe abdominal pain due to intestinal oedema, both lasting more than 24 hours.
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
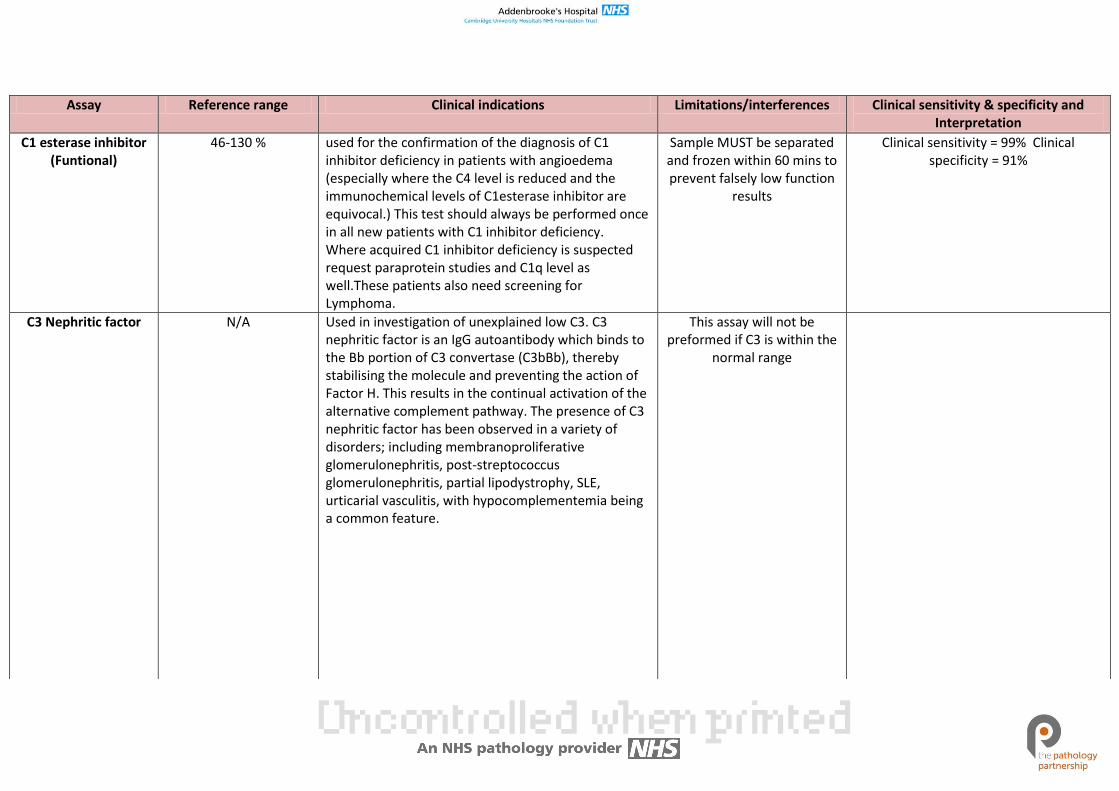
C1 esterase inhibitor (Funtional)
46-130 % used for the confirmation of the diagnosis of C1 inhibitor deficiency in patients with angioedema (especially where the C4 level is reduced and the immunochemical levels of C1esterase inhibitor are equivocal.) This test should always be performed once in all new patients with C1 inhibitor deficiency. Where acquired C1 inhibitor deficiency is suspected request paraprotein studies and C1q level as well.These patients also need screening for Lymphoma.
Sample MUST be separated and frozen within 60 mins to prevent falsely low function
results
Clinical sensitivity = 99% Clinical specificity = 91%
C3 Nephritic factor N/A Used in investigation of unexplained low C3. C3 nephritic factor is an IgG autoantibody which binds to the Bb portion of C3 convertase (C3bBb), thereby stabilising the molecule and preventing the action of Factor H. This results in the continual activation of the alternative complement pathway. The presence of C3 nephritic factor has been observed in a variety of disorders; including membranoproliferative glomerulonephritis, post-streptococcus glomerulonephritis, partial lipodystrophy, SLE, urticarial vasculitis, with hypocomplementemia being a common feature.
This assay will not be preformed if C3 is within the
normal range
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
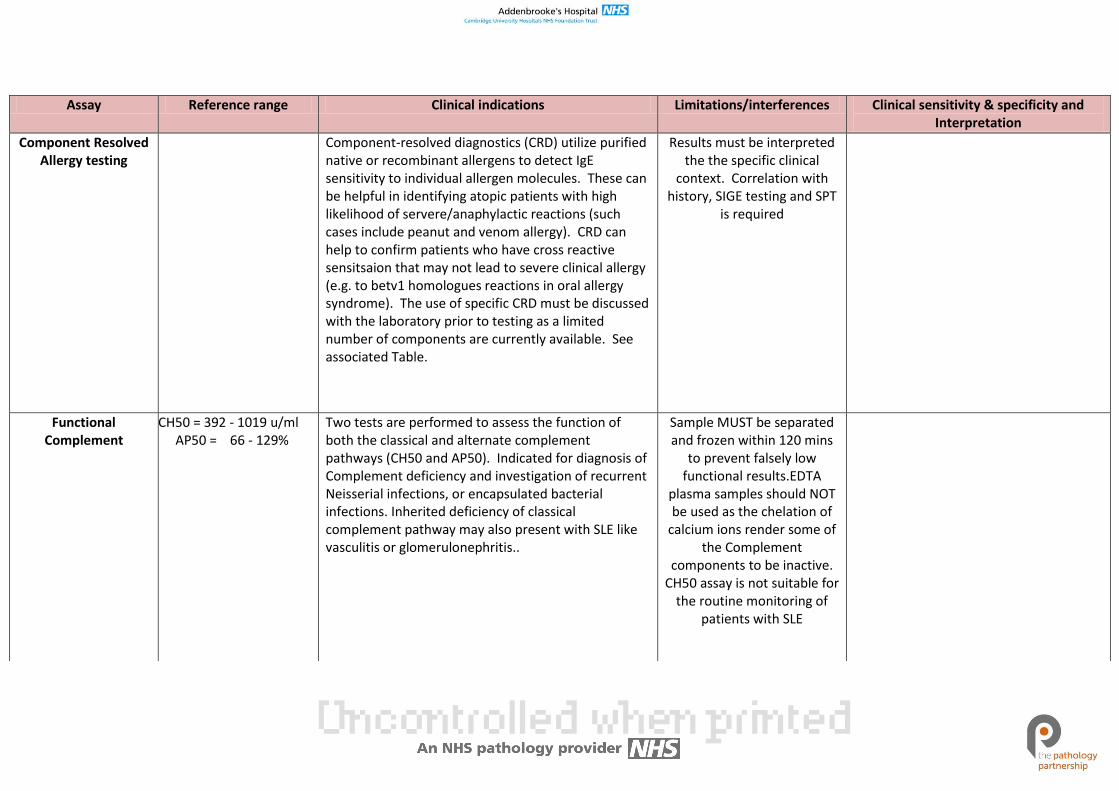
Component Resolved Allergy testing
Component-resolved diagnostics (CRD) utilize purified native or recombinant allergens to detect IgE sensitivity to individual allergen molecules. These can be helpful in identifying atopic patients with high likelihood of servere/anaphylactic reactions (such cases include peanut and venom allergy). CRD can help to confirm patients who have cross reactive sensitsaion that may not lead to severe clinical allergy (e.g. to betv1 homologues reactions in oral allergy syndrome). The use of specific CRD must be discussed with the laboratory prior to testing as a limited number of components are currently available. See associated Table.
Results must be interpreted the the specific clinical
context. Correlation with history, SIGE testing and SPT
is required
Functional Complement
CH50 = 392 - 1019 u/ml AP50 = 66 - 129%
Two tests are performed to assess the function of both the classical and alternate complement pathways (CH50 and AP50). Indicated for diagnosis of Complement deficiency and investigation of recurrent Neisserial infections, or encapsulated bacterial infections. Inherited deficiency of classical complement pathway may also present with SLE like vasculitis or glomerulonephritis..
Sample MUST be separated and frozen within 120 mins
to prevent falsely low functional results.EDTA
plasma samples should NOT be used as the chelation of
calcium ions render some of the Complement
components to be inactive. CH50 assay is not suitable for
the routine monitoring of patients with SLE
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
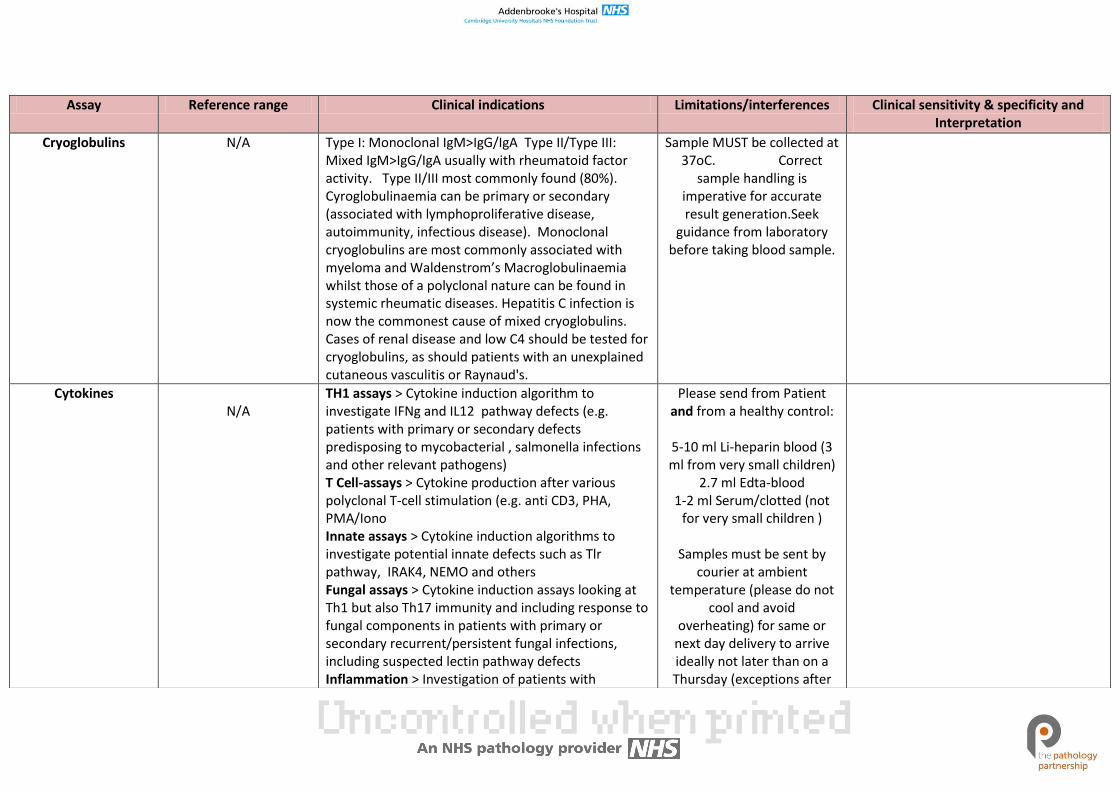
Cryoglobulins N/A Type I: Monoclonal IgM>IgG/IgA Type II/Type III: Mixed IgM>IgG/IgA usually with rheumatoid factor activity. Type II/III most commonly found (80%). Cyroglobulinaemia can be primary or secondary (associated with lymphoproliferative disease, autoimmunity, infectious disease). Monoclonal cryoglobulins are most commonly associated with myeloma and Waldenstrom’s Macroglobulinaemia whilst those of a polyclonal nature can be found in systemic rheumatic diseases. Hepatitis C infection is now the commonest cause of mixed cryoglobulins. Cases of renal disease and low C4 should be tested for cryoglobulins, as should patients with an unexplained cutaneous vasculitis or Raynaud's.
Sample MUST be collected at 37oC. Correct
sample handling is imperative for accurate result generation.Seek
guidance from laboratory before taking blood sample.
Cytokines N/A
TH1 assays > Cytokine induction algorithm to investigate IFNg and IL12 pathway defects (e.g. patients with primary or secondary defects predisposing to mycobacterial , salmonella infections and other relevant pathogens) T Cell-assays > Cytokine production after various polyclonal T-cell stimulation (e.g. anti CD3, PHA, PMA/Iono Innate assays > Cytokine induction algorithms to investigate potential innate defects such as Tlr pathway, IRAK4, NEMO and others Fungal assays > Cytokine induction assays looking at Th1 but also Th17 immunity and including response to fungal components in patients with primary or secondary recurrent/persistent fungal infections, including suspected lectin pathway defects Inflammation > Investigation of patients with
Please send from Patient and from a healthy control:
5-10 ml Li-heparin blood (3 ml from very small children)
2.7 ml Edta-blood 1-2 ml Serum/clotted (not
for very small children )
Samples must be sent by courier at ambient
temperature (please do not cool and avoid
overheating) for same or next day delivery to arrive ideally not later than on a Thursday (exceptions after
suspected auto-inflammatory conditions and related syndromes (e.g. IRIS, or post Transplantation) including suspected IL10 pathway defects such as IBD
discussion possible)
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
Cytokine antibodies Anti-cytokine serology panel > in patients with suspected secondary immunodeficiency due to anti-cytokine antibodies (e.g. anti IFN gamma, anti IL6, ) or conditions known to be associated/aggravated with/by anti-cytokine auto-antibodies such as Polyglandular syndrome (APS1, APECED), Thymoma , Pulmonar alveolar Proteinosis (anti GM-CSF) and others;
ENA Screen 0-0.9 ratio units Follow-up test only to positive ANA FEIA(ELISA) ANA Screen positives are followed up with ENA screening
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
ENA Profile 0 – 7 u/ml
0 – 5 u/ml
0 – 7 u/ml
0 – 7 u/ml
Sm Specific for SLE but found in only 20-30% of SLE patients with a higher incidence in non-Caucasians, especially those of Afro-Caribbean descent. There is no correlation with disease activity. U1RNP A high titre positive result of U1RNP in the absence of other autoantibodies is diagnostic for undifferentiated (mixed) connective tissue disease(MCTD) but these antibodies are also found about 25% of SLE patients. RNP70 is a protein within the U1RNP complex. There are also two other proteins in U1RNP. These.are, RNP A and RNP C. Antibodies to RNP70 are more specific for undifferentiated connective tissue disease(MCTD) being found in only about 12% of patients with SLE. Ro or SS-A The Ro (SS-A) antigen also occurs in the cell cytoplasm and very rarely a serum may be positive for Ro antibodies even in the absence of an ANA. These antibodies can cause congenital heart block and is recommended that all female patients suspected of SLE or Sjögren’s syndrome are screened for anti-SS-A (Ro) antibodies especially if they are considering pregnancy. These antibodies are associated with Sjögren’s syndrome (up to 75% in primary Sjögren’s), Sicca syndrome, and in many cases of Sjögren’s syndrome secondary to a variety of other autoimmune diseases. They are also found in variants of SLE including subacute cutaneous lupus and neonatal lupus with congenital heart block and also in SLE resulting from homozygous C2 or C4 deficiency.
ENA screen positives are followed up and typed for these individual ENA(Extractable nuclear antigens),and other ANA/cytoplasmic specificities
0 – 7 u/ml
0 – 7 u/ml
0 – 7 u/ml
La or SS-B Usually found with anti Ro in both primary and secondary Sjögren’s syndrome and SLE. Sjögren’s patients with anti-La are likely to have more extra-glandular disease. Ro and La antibodies are often found together. La is a phosphoprotein and Ro a ribonucleoprotein and both can bind to the same molecule of a transfer RNA. SLE patients positive for Ro & La are likely to have lower DNA antibody titres and less renal disease. Jo- 1(antibodies to aminoacyl-tRNA histidyl synthetase) Associated with inflammatory muscle disease, especially polymyositis (also called anti-synthetase syndrome). Patients with anti-synthetase syndrome have a characteristic clinical picture comprised of myositis and/or interstitial lung disease and/or chronic arthritis. Raynauds phenomenon is frequently observed in this condition. Scl-7O (antibodies to Topoisomerase-I an enzyme catalysing the breaking and re-joining of ssDNA) Found in 20-40% of patients with systemic sclerosis, it is associated with facial skin, kidney and heart involvement, ischaemic fingertip ulcers and pulmonary fibrosis. Centromere antibodies are assocaited with limited cutaneous systemic sclerosis (CREST syndrome: Calcinosis, Raynaud’s phenomenon oEsphageal immobility, Sclerodactyly and Telangectasia). They can also be found in ~10% of patients with primary biliary cirrhosis who may or may not have features of scleroderma).
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
ENA – others N/A
N/A
N/A
N/A
PM-Scl (antibodies to Pm/Scl proteins which function as exoriboncucleases during RNA Processing) Found almost exclusively in patients with idiopathic myositis(including overlap syndromes) or more rarely systemic sclerosis. Cardiac and renal involvement in these patients is very rare, so the prognosis is therefore relatively good. Fibrillarin (fibrillarin is a 34 Kda protein and is the major component of the nucleolar U3-RNP complex, which is involved in pre-r RNA processing)The antibody is found in about 8% of systemic sclerosis patients overall, in 5% of those with diffuse disease and in 10% of those with limited forms. It is a prognostic marker for small intestine and skeletal muscle involvement, as well as pulmonary hypertension. RNA Polymerase III (antibodies to RNA polymerase III are directed against 2 proteins(111A of 150Kda and 111B of 138 kda )located in the nucleoplasm. RNAPs are responsible for the transcription of genes that code for precursor molecules of r RNA ) The antibody is found in about 12-20 % of patients with systemic sclerosis and are thought to be highly specific. They are associated with diffuse or extensive skin manifestations. Mi-2 (antibodies are thought to be directed against a 235-240 Kda antigen within a macromolecular nuclear complex) The antibody is found in 15-30% of
These ENA specifities may be detected by the ANA ELISA test but will be negative on the standard ENA screen and profile follow up testing. In the appropriate clinical and technical situations these autoantibodies will be confirmed or otherwise by a combination of ANA Hep2 and immunoblotting.
N/A
N/A
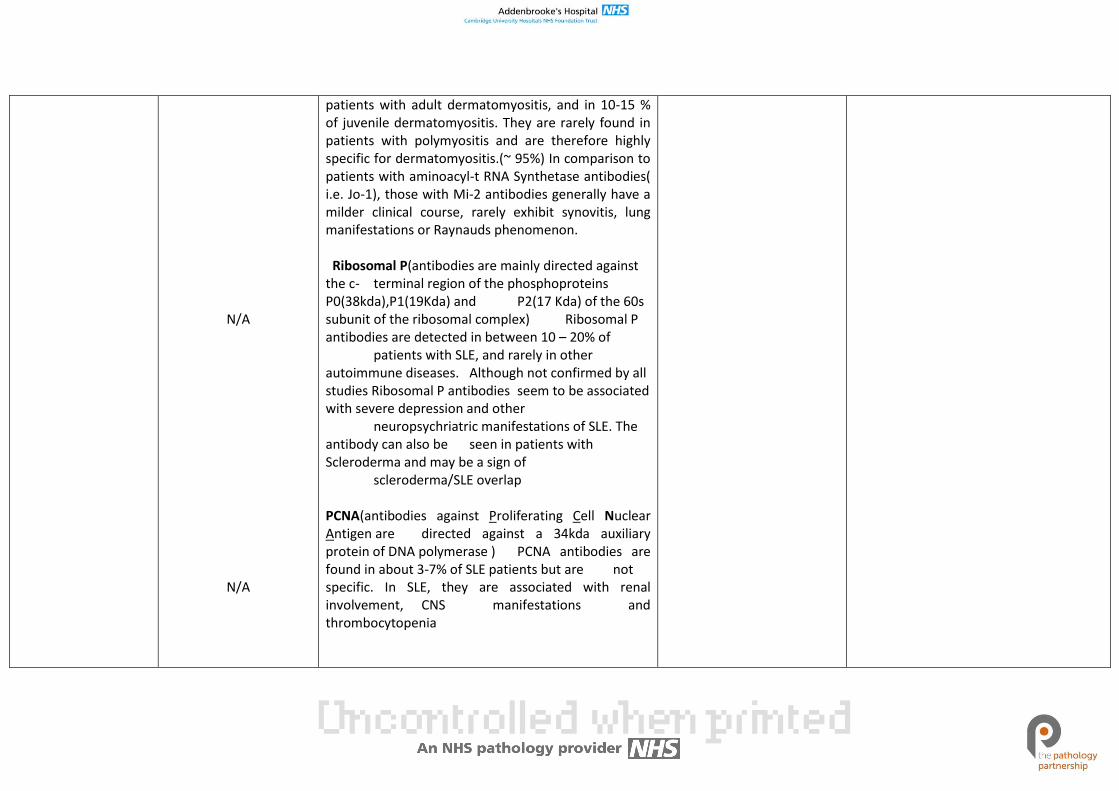
patients with adult dermatomyositis, and in 10-15 % of juvenile dermatomyositis. They are rarely found in patients with polymyositis and are therefore highly specific for dermatomyositis.(~ 95%) In comparison to patients with aminoacyl-t RNA Synthetase antibodies( i.e. Jo-1), those with Mi-2 antibodies generally have a milder clinical course, rarely exhibit synovitis, lung manifestations or Raynauds phenomenon. Ribosomal P(antibodies are mainly directed against the c- terminal region of the phosphoproteins P0(38kda),P1(19Kda) and P2(17 Kda) of the 60s subunit of the ribosomal complex) Ribosomal P antibodies are detected in between 10 – 20% of patients with SLE, and rarely in other autoimmune diseases. Although not confirmed by all studies Ribosomal P antibodies seem to be associated with severe depression and other neuropsychriatric manifestations of SLE. The antibody can also be seen in patients with Scleroderma and may be a sign of scleroderma/SLE overlap PCNA(antibodies against Proliferating Cell Nuclear Antigen are directed against a 34kda auxiliary protein of DNA polymerase ) PCNA antibodies are found in about 3-7% of SLE patients but are not specific. In SLE, they are associated with renal involvement, CNS manifestations and thrombocytopenia
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
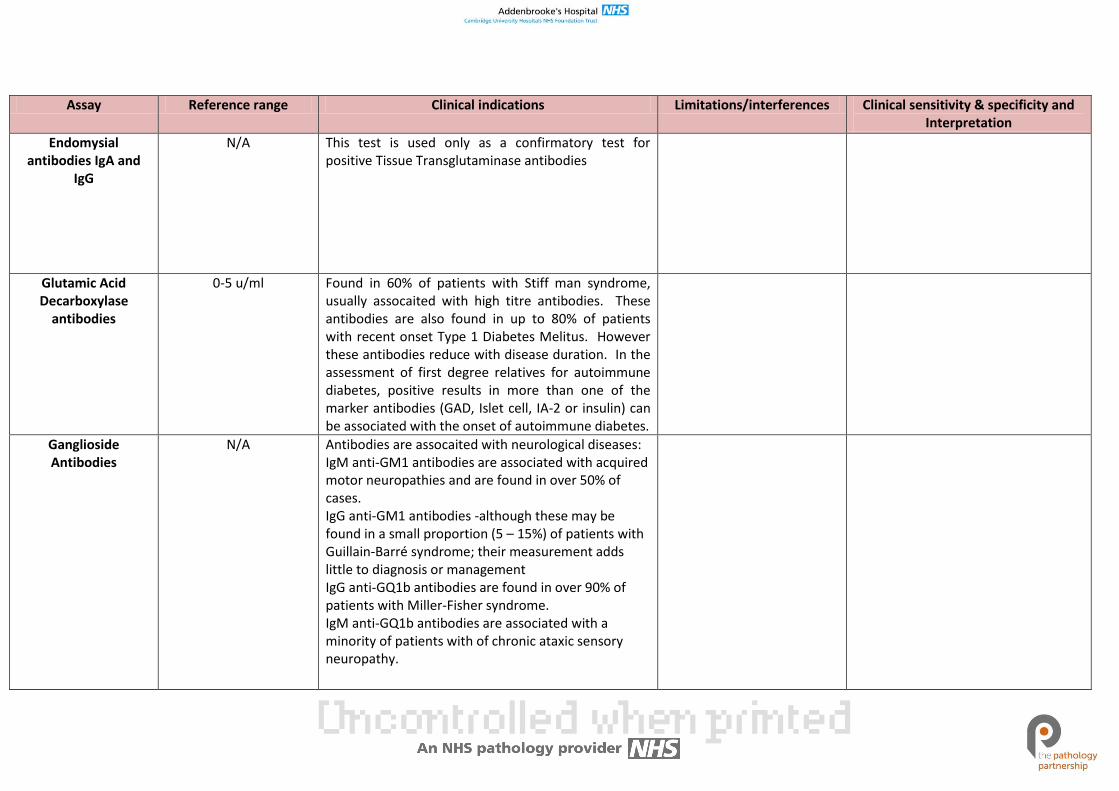
Endomysial antibodies IgA and
IgG
N/A This test is used only as a confirmatory test for positive Tissue Transglutaminase antibodies
Glutamic Acid Decarboxylase
antibodies
0-5 u/ml Found in 60% of patients with Stiff man syndrome, usually assocaited with high titre antibodies. These antibodies are also found in up to 80% of patients with recent onset Type 1 Diabetes Melitus. However these antibodies reduce with disease duration. In the assessment of first degree relatives for autoimmune diabetes, positive results in more than one of the marker antibodies (GAD, Islet cell, IA-2 or insulin) can be associated with the onset of autoimmune diabetes.
Ganglioside Antibodies
N/A Antibodies are assocaited with neurological diseases: IgM anti-GM1 antibodies are associated with acquired motor neuropathies and are found in over 50% of cases. IgG anti-GM1 antibodies -although these may be found in a small proportion (5 – 15%) of patients with Guillain-Barré syndrome; their measurement adds little to diagnosis or management IgG anti-GQ1b antibodies are found in over 90% of patients with Miller-Fisher syndrome. IgM anti-GQ1b antibodies are associated with a minority of patients with of chronic ataxic sensory neuropathy.
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
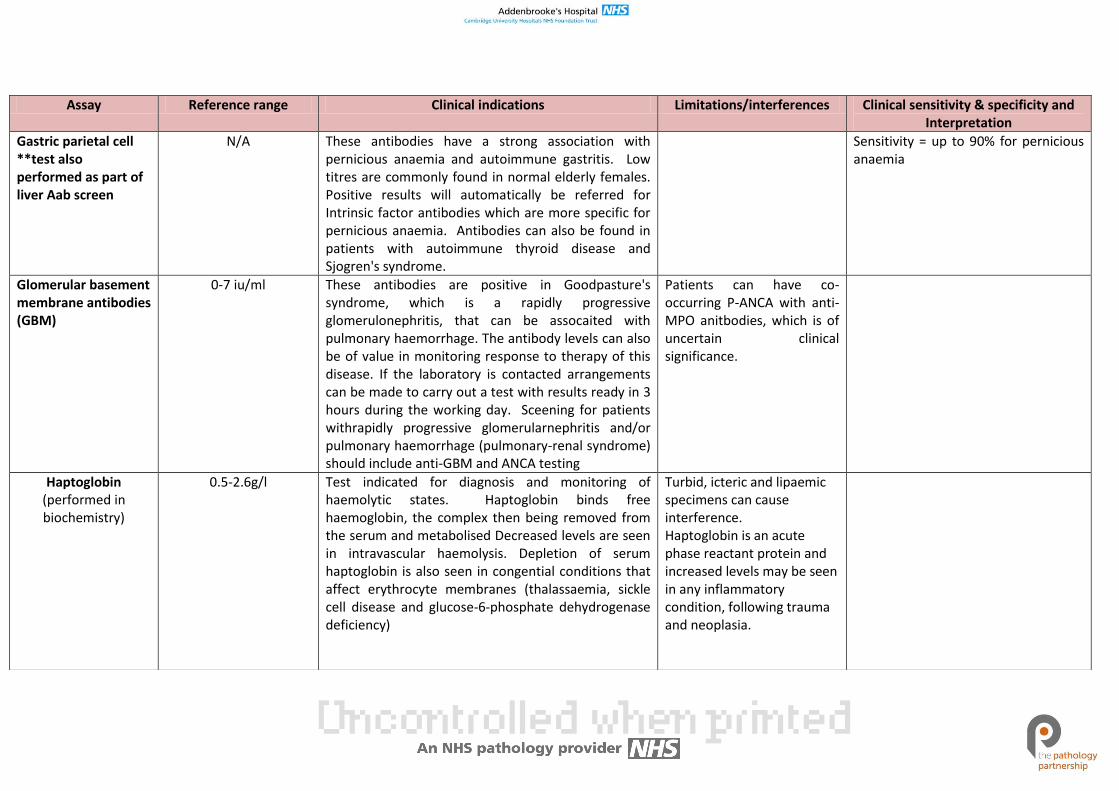
Gastric parietal cell **test also performed as part of liver Aab screen
N/A These antibodies have a strong association with pernicious anaemia and autoimmune gastritis. Low titres are commonly found in normal elderly females. Positive results will automatically be referred for Intrinsic factor antibodies which are more specific for pernicious anaemia. Antibodies can also be found in patients with autoimmune thyroid disease and Sjogren's syndrome.
Sensitivity = up to 90% for pernicious anaemia
Glomerular basement membrane antibodies (GBM)
0-7 iu/ml These antibodies are positive in Goodpasture's syndrome, which is a rapidly progressive glomerulonephritis, that can be assocaited with pulmonary haemorrhage. The antibody levels can also be of value in monitoring response to therapy of this disease. If the laboratory is contacted arrangements can be made to carry out a test with results ready in 3 hours during the working day. Sceening for patients withrapidly progressive glomerularnephritis and/or pulmonary haemorrhage (pulmonary-renal syndrome) should include anti-GBM and ANCA testing
Patients can have co-occurring P-ANCA with anti-MPO anitbodies, which is of uncertain clinical significance.
Haptoglobin (performed in biochemistry)
0.5-2.6g/l Test indicated for diagnosis and monitoring of haemolytic states. Haptoglobin binds free haemoglobin, the complex then being removed from the serum and metabolised Decreased levels are seen in intravascular haemolysis. Depletion of serum haptoglobin is also seen in congential conditions that affect erythrocyte membranes (thalassaemia, sickle cell disease and glucose-6-phosphate dehydrogenase deficiency)
Turbid, icteric and lipaemic specimens can cause interference. Haptoglobin is an acute phase reactant protein and increased levels may be seen in any inflammatory condition, following trauma and neoplasia.
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
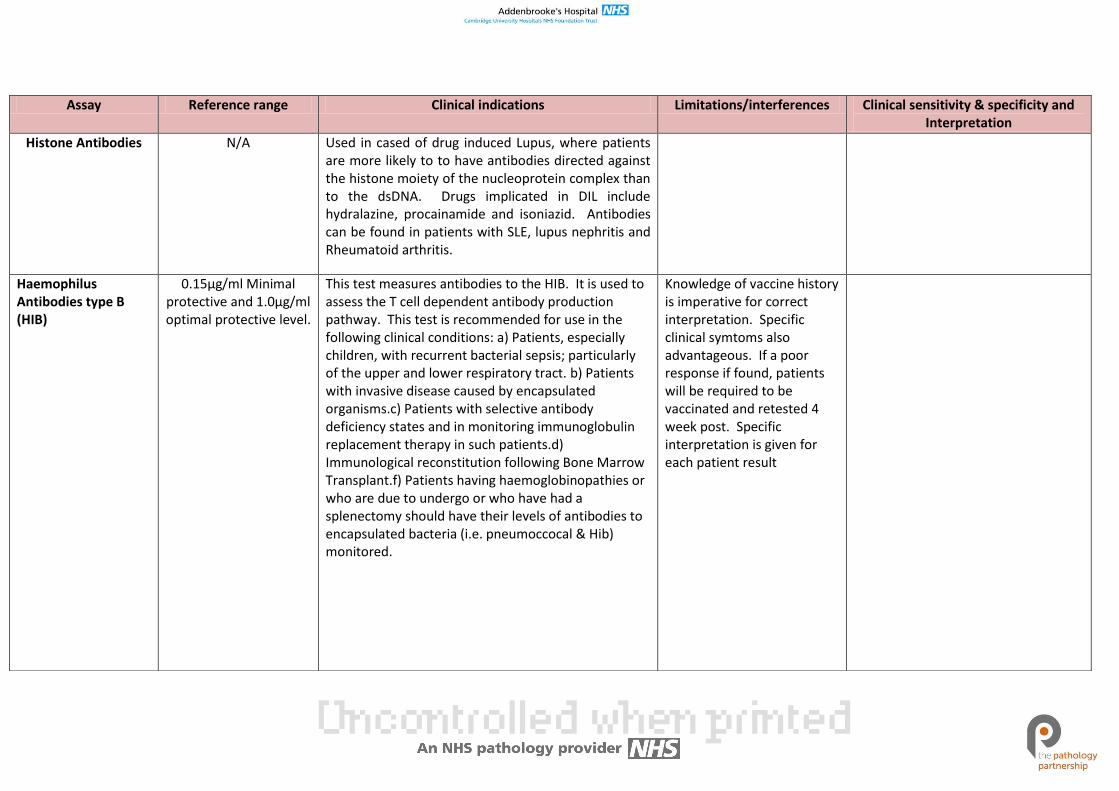
Histone Antibodies N/A Used in cased of drug induced Lupus, where patients are more likely to to have antibodies directed against the histone moiety of the nucleoprotein complex than to the dsDNA. Drugs implicated in DIL include hydralazine, procainamide and isoniazid. Antibodies can be found in patients with SLE, lupus nephritis and Rheumatoid arthritis.
Haemophilus Antibodies type B (HIB)
0.15µg/ml Minimal protective and 1.0µg/ml optimal protective level.
This test measures antibodies to the HIB. It is used to assess the T cell dependent antibody production pathway. This test is recommended for use in the following clinical conditions: a) Patients, especially children, with recurrent bacterial sepsis; particularly of the upper and lower respiratory tract. b) Patients with invasive disease caused by encapsulated organisms.c) Patients with selective antibody deficiency states and in monitoring immunoglobulin replacement therapy in such patients.d) Immunological reconstitution following Bone Marrow Transplant.f) Patients having haemoglobinopathies or who are due to undergo or who have had a splenectomy should have their levels of antibodies to encapsulated bacteria (i.e. pneumoccocal & Hib) monitored.
Knowledge of vaccine history is imperative for correct interpretation. Specific clinical symtoms also advantageous. If a poor response if found, patients will be required to be vaccinated and retested 4 week post. Specific interpretation is given for each patient result
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
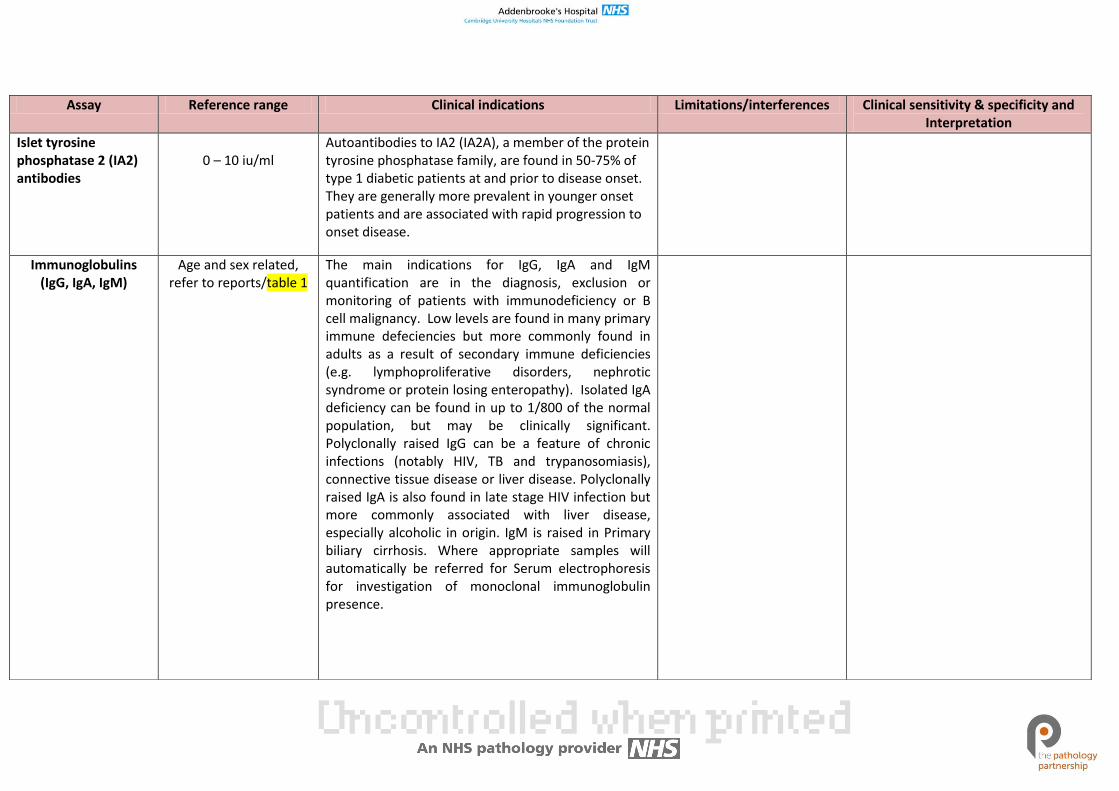
Islet tyrosine phosphatase 2 (IA2) antibodies
0 – 10 iu/ml
Autoantibodies to IA2 (IA2A), a member of the protein tyrosine phosphatase family, are found in 50-75% of type 1 diabetic patients at and prior to disease onset. They are generally more prevalent in younger onset patients and are associated with rapid progression to onset disease.
Immunoglobulins (IgG, IgA, IgM)
Age and sex related, refer to reports/table 1
The main indications for IgG, IgA and IgM quantification are in the diagnosis, exclusion or monitoring of patients with immunodeficiency or B cell malignancy. Low levels are found in many primary immune defeciencies but more commonly found in adults as a result of secondary immune deficiencies (e.g. lymphoproliferative disorders, nephrotic syndrome or protein losing enteropathy). Isolated IgA deficiency can be found in up to 1/800 of the normal population, but may be clinically significant. Polyclonally raised IgG can be a feature of chronic infections (notably HIV, TB and trypanosomiasis), connective tissue disease or liver disease. Polyclonally raised IgA is also found in late stage HIV infection but more commonly associated with liver disease, especially alcoholic in origin. IgM is raised in Primary biliary cirrhosis. Where appropriate samples will automatically be referred for Serum electrophoresis for investigation of monoclonal immunoglobulin presence.
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
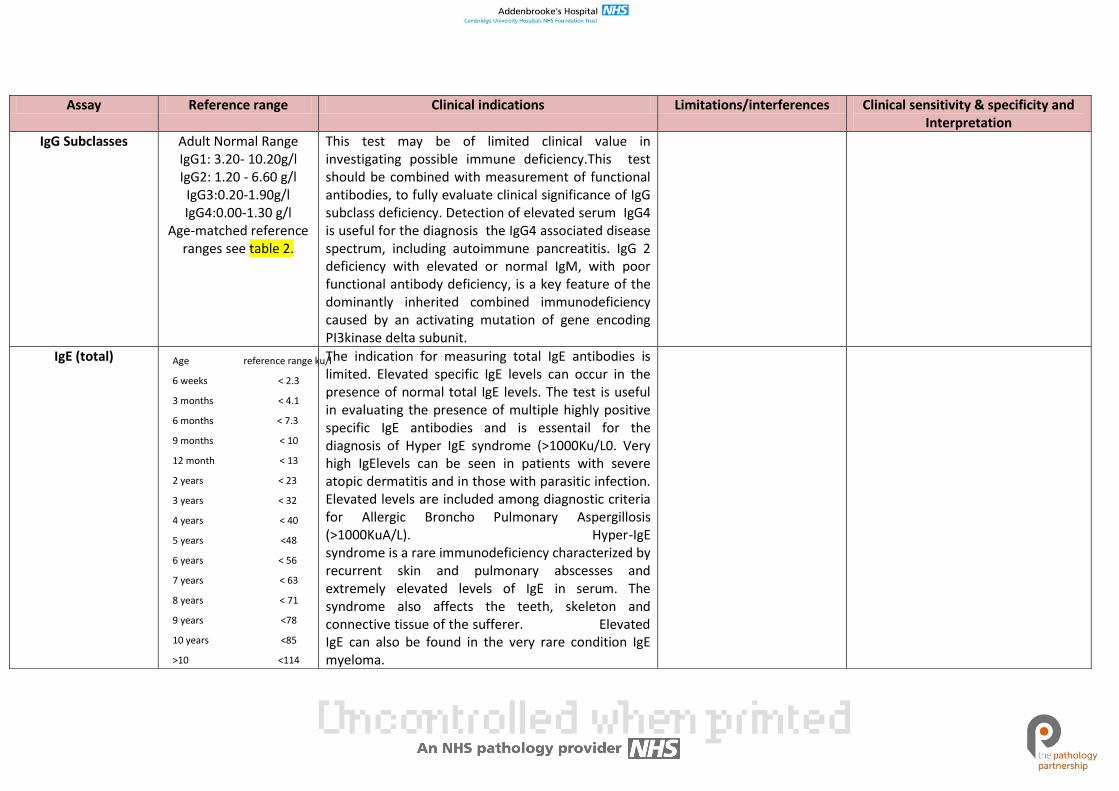
IgG Subclasses Adult Normal Range IgG1: 3.20- 10.20g/l IgG2: 1.20 - 6.60 g/l IgG3:0.20-1.90g/l IgG4:0.00-1.30 g/l
Age-matched reference ranges see table 2.
This test may be of limited clinical value in investigating possible immune deficiency.This test should be combined with measurement of functional antibodies, to fully evaluate clinical significance of IgG subclass deficiency. Detection of elevated serum IgG4 is useful for the diagnosis the IgG4 associated disease spectrum, including autoimmune pancreatitis. IgG 2 deficiency with elevated or normal IgM, with poor functional antibody deficiency, is a key feature of the dominantly inherited combined immunodeficiency caused by an activating mutation of gene encoding PI3kinase delta subunit.
IgE (total) Age reference range ku/l
6 weeks < 2.3
3 months < 4.1
6 months < 7.3
9 months < 10
12 month < 13
2 years < 23
3 years < 32
4 years < 40
5 years <48
6 years < 56
7 years < 63
8 years < 71
9 years <78
10 years <85
>10 <114
The indication for measuring total IgE antibodies is limited. Elevated specific IgE levels can occur in the presence of normal total IgE levels. The test is useful in evaluating the presence of multiple highly positive specific IgE antibodies and is essentail for the diagnosis of Hyper IgE syndrome (>1000Ku/L0. Very high IgElevels can be seen in patients with severe atopic dermatitis and in those with parasitic infection. Elevated levels are included among diagnostic criteria for Allergic Broncho Pulmonary Aspergillosis (>1000KuA/L). Hyper-IgE syndrome is a rare immunodeficiency characterized by recurrent skin and pulmonary abscesses and extremely elevated levels of IgE in serum. The syndrome also affects the teeth, skeleton and connective tissue of the sufferer. Elevated IgE can also be found in the very rare condition IgE myeloma.
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
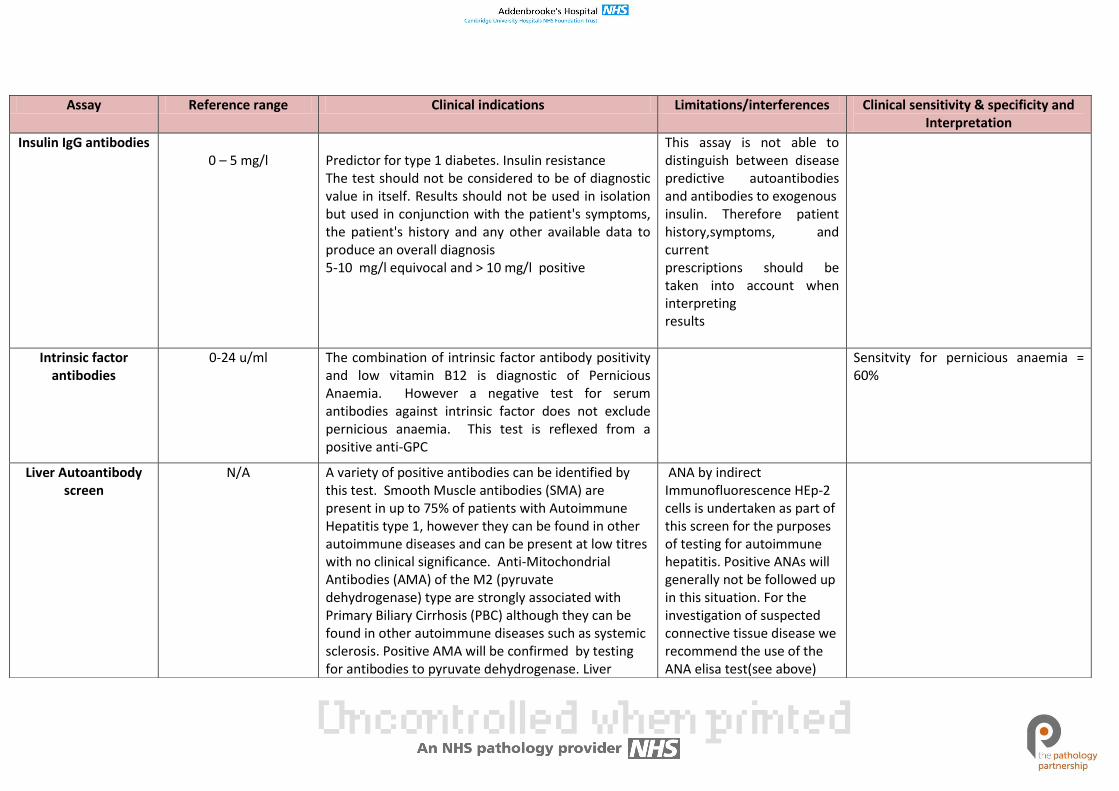
Insulin IgG antibodies 0 – 5 mg/l
Predictor for type 1 diabetes. Insulin resistance The test should not be considered to be of diagnostic value in itself. Results should not be used in isolation but used in conjunction with the patient's symptoms, the patient's history and any other available data to produce an overall diagnosis 5-10 mg/l equivocal and > 10 mg/l positive
This assay is not able to distinguish between disease predictive autoantibodies and antibodies to exogenous insulin. Therefore patient history,symptoms, and current prescriptions should be taken into account when interpreting results
Intrinsic factor antibodies
0-24 u/ml The combination of intrinsic factor antibody positivity and low vitamin B12 is diagnostic of Pernicious Anaemia. However a negative test for serum antibodies against intrinsic factor does not exclude pernicious anaemia. This test is reflexed from a positive anti-GPC
Sensitvity for pernicious anaemia = 60%
Liver Autoantibody screen
N/A A variety of positive antibodies can be identified by this test. Smooth Muscle antibodies (SMA) are present in up to 75% of patients with Autoimmune Hepatitis type 1, however they can be found in other autoimmune diseases and can be present at low titres with no clinical significance. Anti-Mitochondrial Antibodies (AMA) of the M2 (pyruvate dehydrogenase) type are strongly associated with Primary Biliary Cirrhosis (PBC) although they can be found in other autoimmune diseases such as systemic sclerosis. Positive AMA will be confirmed by testing for antibodies to pyruvate dehydrogenase. Liver
ANA by indirect Immunofluorescence HEp-2 cells is undertaken as part of this screen for the purposes of testing for autoimmune hepatitis. Positive ANAs will generally not be followed up in this situation. For the investigation of suspected connective tissue disease we recommend the use of the ANA elisa test(see above)
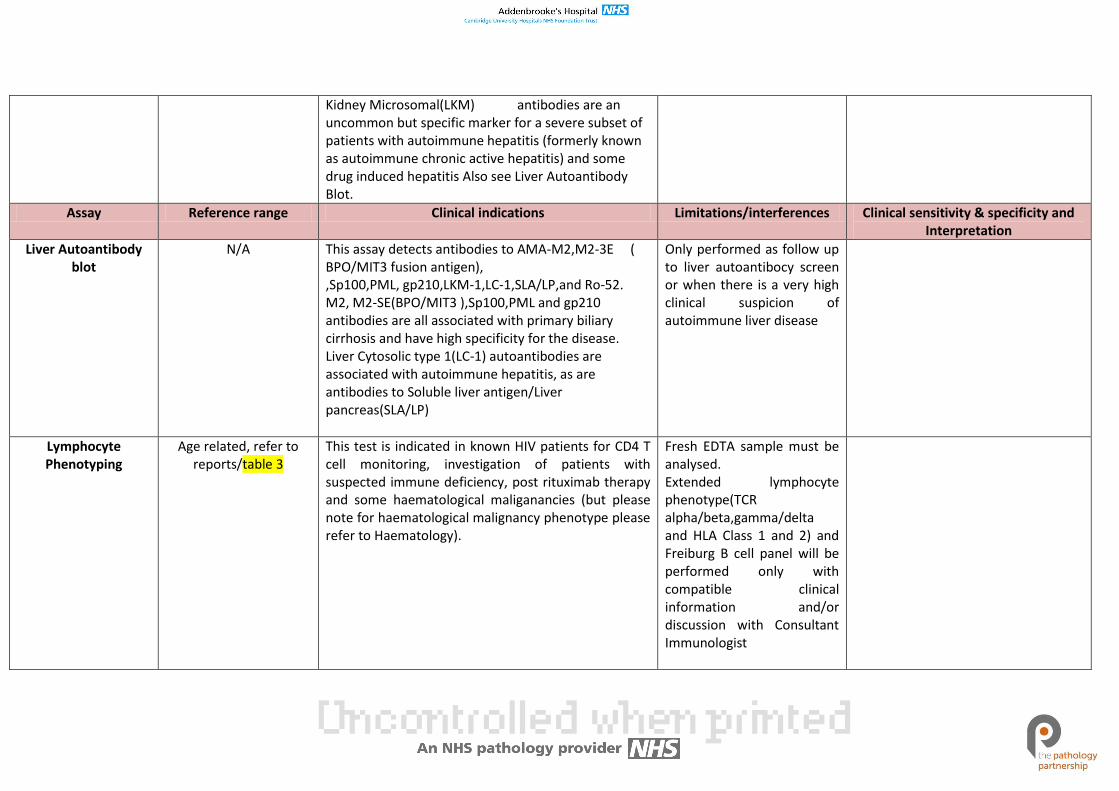
Kidney Microsomal(LKM) antibodies are an uncommon but specific marker for a severe subset of patients with autoimmune hepatitis (formerly known as autoimmune chronic active hepatitis) and some drug induced hepatitis Also see Liver Autoantibody Blot.
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
Liver Autoantibody blot
N/A This assay detects antibodies to AMA-M2,M2-3E ( BPO/MIT3 fusion antigen), ,Sp100,PML, gp210,LKM-1,LC-1,SLA/LP,and Ro-52. M2, M2-SE(BPO/MIT3 ),Sp100,PML and gp210 antibodies are all associated with primary biliary cirrhosis and have high specificity for the disease. Liver Cytosolic type 1(LC-1) autoantibodies are associated with autoimmune hepatitis, as are antibodies to Soluble liver antigen/Liver pancreas(SLA/LP)
Only performed as follow up to liver autoantibocy screen or when there is a very high clinical suspicion of autoimmune liver disease
Lymphocyte Phenotyping
Age related, refer to reports/table 3
This test is indicated in known HIV patients for CD4 T cell monitoring, investigation of patients with suspected immune deficiency, post rituximab therapy and some haematological maliganancies (but please note for haematological malignancy phenotype please refer to Haematology).
Fresh EDTA sample must be analysed. Extended lymphocyte phenotype(TCR alpha/beta,gamma/delta and HLA Class 1 and 2) and Freiburg B cell panel will be performed only with compatible clinical information and/or discussion with Consultant Immunologist
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
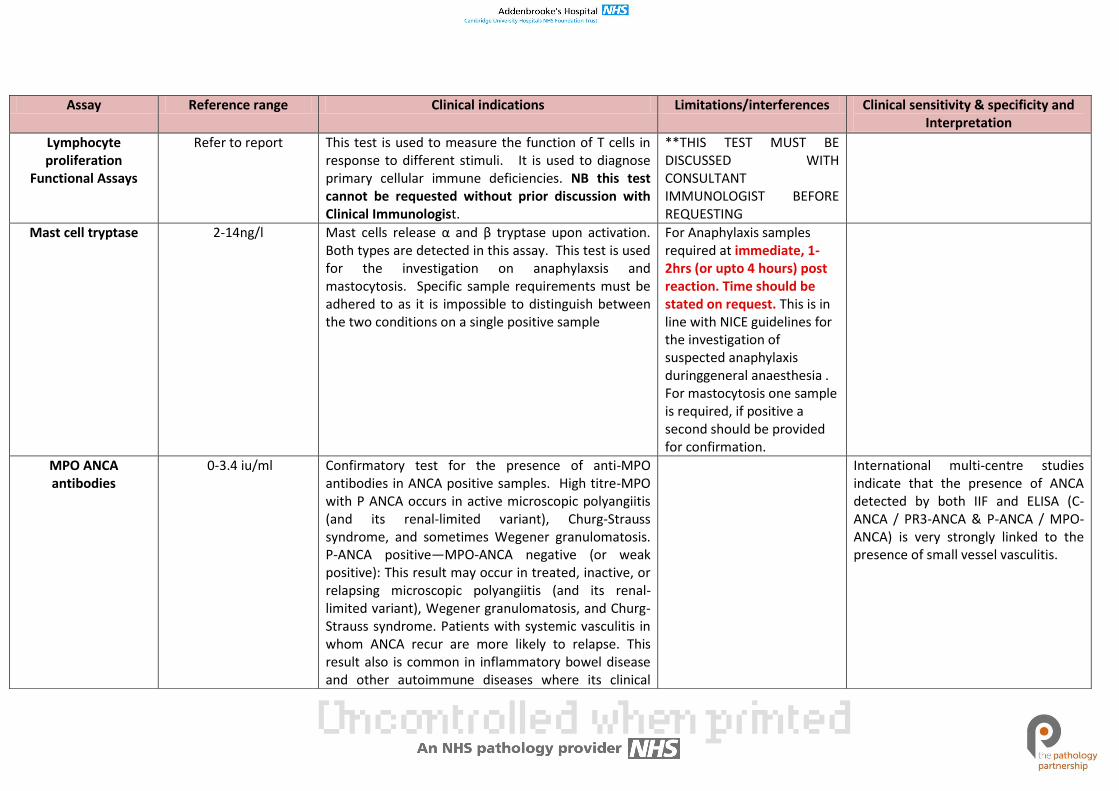
Lymphocyte proliferation
Functional Assays
Refer to report This test is used to measure the function of T cells in response to different stimuli. It is used to diagnose primary cellular immune deficiencies. NB this test cannot be requested without prior discussion with Clinical Immunologist.
**THIS TEST MUST BE DISCUSSED WITH CONSULTANT IMMUNOLOGIST BEFORE REQUESTING
Mast cell tryptase 2-14ng/l Mast cells release α and β tryptase upon activation. Both types are detected in this assay. This test is used for the investigation on anaphylaxsis and mastocytosis. Specific sample requirements must be adhered to as it is impossible to distinguish between the two conditions on a single positive sample
For Anaphylaxis samples required at immediate, 1-2hrs (or upto 4 hours) post reaction. Time should be stated on request. This is in line with NICE guidelines for the investigation of suspected anaphylaxis duringgeneral anaesthesia . For mastocytosis one sample is required, if positive a second should be provided for confirmation.
MPO ANCA antibodies
0-3.4 iu/ml Confirmatory test for the presence of anti-MPO antibodies in ANCA positive samples. High titre-MPO with P ANCA occurs in active microscopic polyangiitis (and its renal-limited variant), Churg-Strauss syndrome, and sometimes Wegener granulomatosis. P-ANCA positive—MPO-ANCA negative (or weak positive): This result may occur in treated, inactive, or relapsing microscopic polyangiitis (and its renal-limited variant), Wegener granulomatosis, and Churg-Strauss syndrome. Patients with systemic vasculitis in whom ANCA recur are more likely to relapse. This result also is common in inflammatory bowel disease and other autoimmune diseases where its clinical
International multi-centre studies indicate that the presence of ANCA detected by both IIF and ELISA (C-ANCA / PR3-ANCA & P-ANCA / MPO-ANCA) is very strongly linked to the presence of small vessel vasculitis.
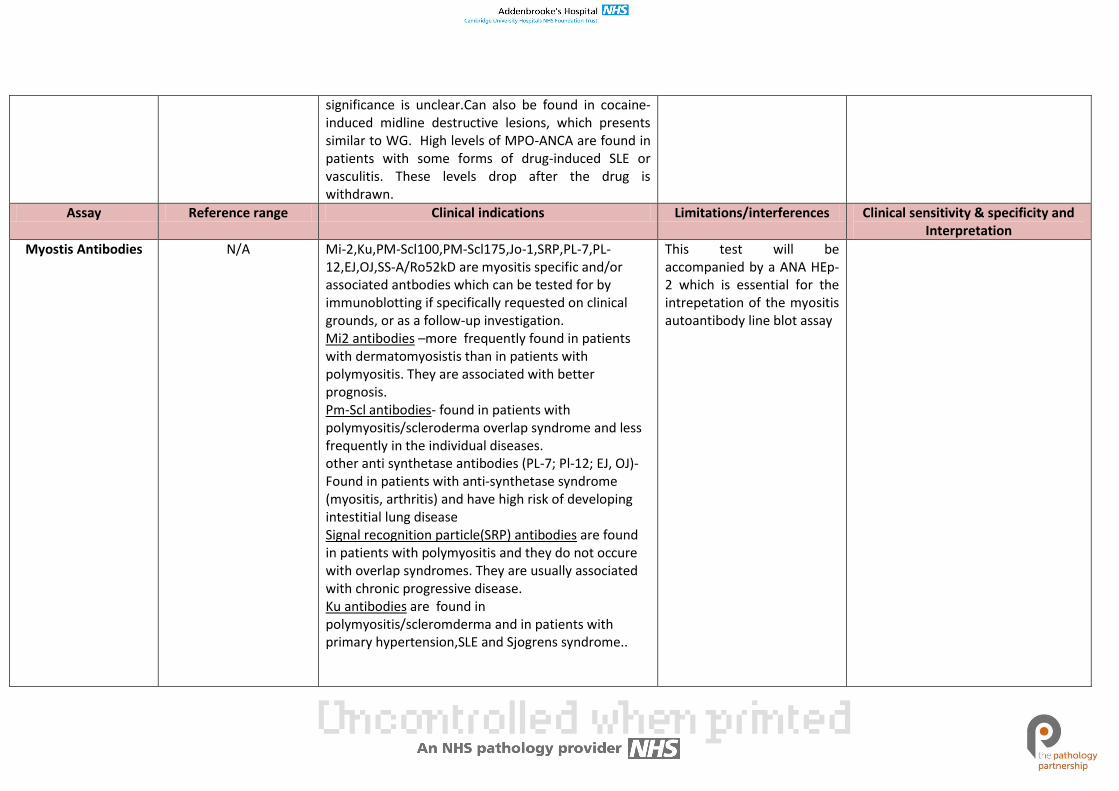
significance is unclear.Can also be found in cocaine-induced midline destructive lesions, which presents similar to WG. High levels of MPO-ANCA are found in patients with some forms of drug-induced SLE or vasculitis. These levels drop after the drug is withdrawn.
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
Myostis Antibodies N/A Mi-2,Ku,PM-Scl100,PM-Scl175,Jo-1,SRP,PL-7,PL-12,EJ,OJ,SS-A/Ro52kD are myositis specific and/or associated antbodies which can be tested for by immunoblotting if specifically requested on clinical grounds, or as a follow-up investigation. Mi2 antibodies –more frequently found in patients with dermatomyosistis than in patients with polymyositis. They are associated with better prognosis. Pm-Scl antibodies- found in patients with polymyositis/scleroderma overlap syndrome and less frequently in the individual diseases. other anti synthetase antibodies (PL-7; Pl-12; EJ, OJ)- Found in patients with anti-synthetase syndrome (myositis, arthritis) and have high risk of developing intestitial lung disease Signal recognition particle(SRP) antibodies are found in patients with polymyositis and they do not occure with overlap syndromes. They are usually associated with chronic progressive disease. Ku antibodies are found in polymyositis/scleromderma and in patients with primary hypertension,SLE and Sjogrens syndrome..
This test will be accompanied by a ANA HEp-2 which is essential for the intrepetation of the myositis autoantibody line blot assay
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
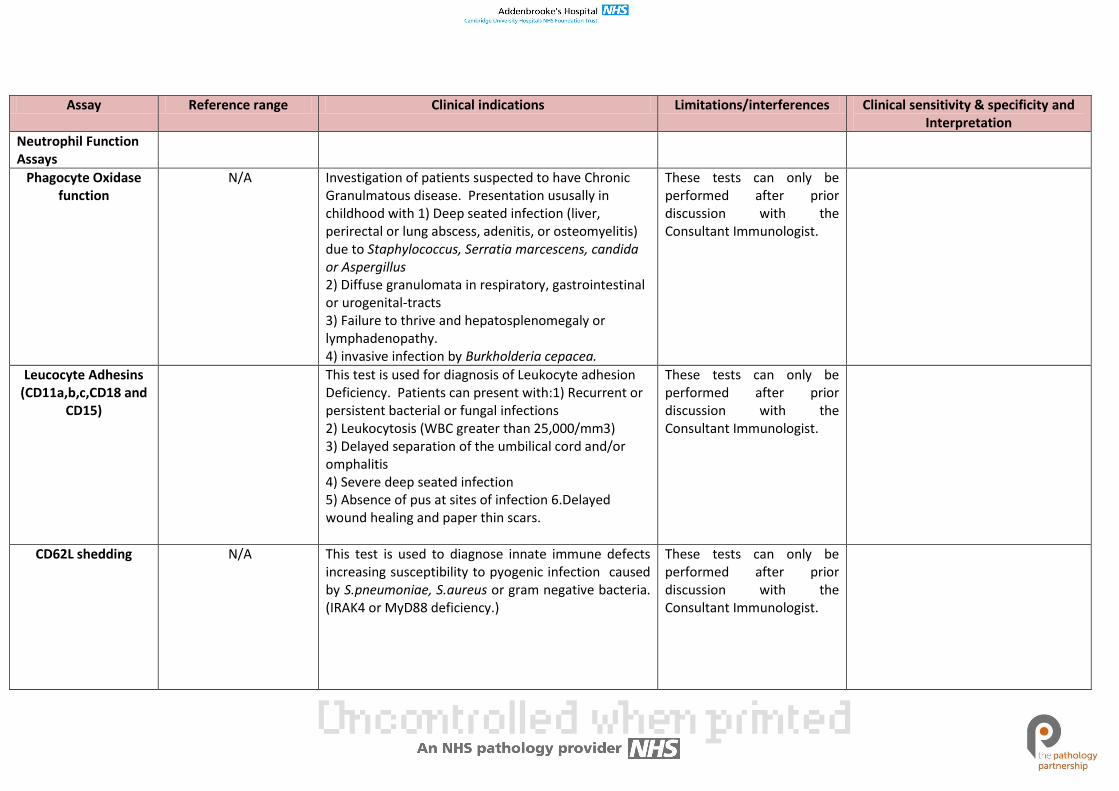
Neutrophil Function Assays
Phagocyte Oxidase function
N/A Investigation of patients suspected to have Chronic Granulmatous disease. Presentation ususally in childhood with 1) Deep seated infection (liver, perirectal or lung abscess, adenitis, or osteomyelitis) due to Staphylococcus, Serratia marcescens, candida or Aspergillus 2) Diffuse granulomata in respiratory, gastrointestinal or urogenital-tracts 3) Failure to thrive and hepatosplenomegaly or lymphadenopathy. 4) invasive infection by Burkholderia cepacea.
These tests can only be performed after prior discussion with the Consultant Immunologist.
Leucocyte Adhesins (CD11a,b,c,CD18 and
CD15)
This test is used for diagnosis of Leukocyte adhesion Deficiency. Patients can present with:1) Recurrent or persistent bacterial or fungal infections 2) Leukocytosis (WBC greater than 25,000/mm3) 3) Delayed separation of the umbilical cord and/or omphalitis 4) Severe deep seated infection 5) Absence of pus at sites of infection 6.Delayed wound healing and paper thin scars.
These tests can only be performed after prior discussion with the Consultant Immunologist.
CD62L shedding N/A This test is used to diagnose innate immune defects increasing susceptibility to pyogenic infection caused by S.pneumoniae, S.aureus or gram negative bacteria. (IRAK4 or MyD88 deficiency.)
These tests can only be performed after prior discussion with the Consultant Immunologist.
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
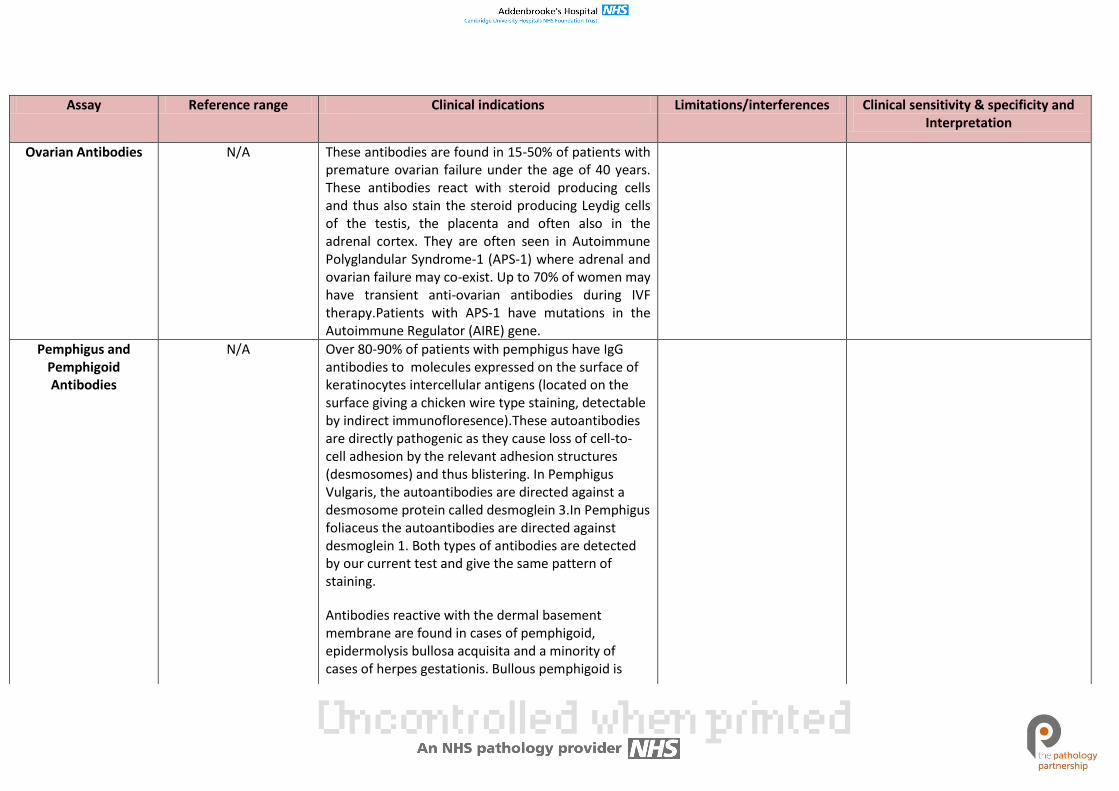
Ovarian Antibodies N/A These antibodies are found in 15-50% of patients with premature ovarian failure under the age of 40 years. These antibodies react with steroid producing cells and thus also stain the steroid producing Leydig cells of the testis, the placenta and often also in the adrenal cortex. They are often seen in Autoimmune Polyglandular Syndrome-1 (APS-1) where adrenal and ovarian failure may co-exist. Up to 70% of women may have transient anti-ovarian antibodies during IVF therapy.Patients with APS-1 have mutations in the Autoimmune Regulator (AIRE) gene.
Pemphigus and Pemphigoid Antibodies
N/A Over 80-90% of patients with pemphigus have IgG antibodies to molecules expressed on the surface of keratinocytes intercellular antigens (located on the surface giving a chicken wire type staining, detectable by indirect immunofloresence).These autoantibodies are directly pathogenic as they cause loss of cell-to-cell adhesion by the relevant adhesion structures (desmosomes) and thus blistering. In Pemphigus Vulgaris, the autoantibodies are directed against a desmosome protein called desmoglein 3.In Pemphigus foliaceus the autoantibodies are directed against desmoglein 1. Both types of antibodies are detected by our current test and give the same pattern of staining.
Antibodies reactive with the dermal basement membrane are found in cases of pemphigoid, epidermolysis bullosa acquisita and a minority of cases of herpes gestationis. Bullous pemphigoid is
blistering disease affecting skin and mucous membranes, while cicatrial pemphigoid primarily affects the mucous membranes. Blood of patients with bullous pemphigoid contain (IgG, Sometimes IgA) antibodies directed against molecules expressed on the surface of antigens expressed on the epidermal basement membrane (hemi-desmosomes). These antibodies cause activation of complement. Complement breakdown products attract phagocytic cells to the basement membrane zone. The combined action of the membrane attack complex of complement and enzymes liberated by the activated phagocytes results in damage to the basement membrane zone causing subepidermal blister formation.
80% of patients with bullous pemphigoid have IgG antibodies to the epidermal basement membrane zone. Only about 20% of patients with cicatrial pemphigoid have similar autoantibodies detectable with indirect immunofluoresence
For patients with blistering skin diseases, an unfixed skin biopsy for the more sensitive test of direct immunofluorescence should also be sent to the histology department.
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
PR3 ANCA Antibodies 0-1.9 iu/ml Confirmatory test for the presence of anti-PR3 antibodies in ANCA positive samples, identified by indirect immunofluoresence. C-ANCA positive—PR3-ANCA: This result occurs in active Polyangitis with granulomatosis (Wegener's granulomatosis), microscopic polyangiitis (and its renal-limited variant), and Churg-Strauss syndrome. Patients with systemic vasculitis in whom ANCA recur are more likely to relapse C-ANCA positive—PR3-ANCA negative and MPO-ANCA negative: This result may occur in treated, inactive, or relapsing Polyangitis with granulomatosis (Wegener's granulomatosis),microscopic polyangiitis (and its renal-limited variant), and Churg-Strauss syndrome. This combination can also be seen in patients with chronic infections or in Inflammatory bowel disease.
International multi-centre studies indicate that the presence of ANCA detected by both IIF and ELISA (C-ANCA / PR3-ANCA & P-ANCA / MPO-ANCA) is very strongly linked to the presence of small vessel vasculitis.
Pancreatic islet cell Antibodies
N/A Presence of islet cell antibodies can aid in the diagnosis of type 1 diabetes Melitus (IDDM). Antibodies are present in up to 70% of new- onset diabetes but their presence is transient , often disappearing once the islets have been destroyed. Various antiboidy targets (glutamic acid decarboxylase 65 antibodies (GAD65) and protein tyrosine phosphatase-like protein (IA2) antibodies) will result in the same staining pattern. This test can also be useful in testing first degree relatives of patients with IDDM as the presence of high titre islet cell antibodies (ICA) confers a risk for development of IDDM. This is most useful if GAD65 and IA2 antibodies are measured Islet cell antibodies along with GAD65,
The presence of ICA does not always correspond to GAD65 and/or IA2 antibodies due to different sensitivities of the assays.
IDDM = 70% sensitive
insulin antibodies and IA2 antibodies may be of use when investigating latent autoimmune diabetes of adulthood (LADA). Approximately 10% of patients diagnosed with type 2 diabetes have LADA which requires insulin therapy. LADA may be distingushed from type 2 diabetes by the presence of the autoantibodies
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
Phospholipid antibodies (Anti-
Cardiolipin and Anti-B2GP1 Abs)
<10 GPL Anti-cardiolipin antibodies (ACA) are associated with anti-phospholipid syndrome, idiopathic spontaneous abortion and systemic lupus erythematosus (SLE). The international consensus statement clarifies that anti-phospholipid syndrome can be diagnosed with: Vascular thrombosis in any organ or tissue or pregnancy event (one or more miscarriages after 10th week of gestation, three or more miscarriages before 10th week of gestation, or one or more premature births before 34th week of gestation due to eclampsia and persistently positive IgG or IgM anti-phospholipid antibodies ( at moderate-high titer : >40 GPL or MPL U/mL), or moderate-to-high titer beta-2 glycoprotein antibodies. Anti-cardiolipin antibodies should be positive on at two occasions at least 12 weeks apart to fulfill the criterion of positive ACA antibodies. IgG anti-cardiolipin antibodies are the most prevalent and demonstrate the greatest clinical correlation. The significance of IgM anti-cardiolipin antibodies is uncertain (these are not measured routinely here). All samples positive for anti-cardiolipin automatically receive anti-B2GP1 tests.
ACA are frequently detected in syphilis, HIV infected patients and other viral, bacterial and parasitic infections but are not correlated with the thrombosis risk or haematological manifestations of anti-phospholipid syndrome
Anti-Cardiolipin (ACA) are not diagnostic in themselves and can be found without a clinical antiphospholipid syndrome. Lupus anticoagulant (DRVVT) must also be checked and APS can be present with an isolated positive LA and undetectable ACA. Cardiolipin antibodies should be repeated at least 12 weeks apart to provide evidence of a persistent autoantibody
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
Pyruvate dehydrogenase
antibodies(PDH-M2)
N/A Antibodies to pyruvate dehydrogenase subunits are the antigen recognised by M2 antibodies and are present in most patients with PBC
Quantiferon TB
This is a new NICE / US-FDA approved blood test for the detection of Mycobacterium tuberculosis infection, whether tuberculosis disease or latent tuberculosis infection (LTBI). It cannot distinguish between tuberculosis disease and LTBI and is intended for use in conjunction with clinical risk assessment, radiography, microbiology and other medical and diagnostic evaluations for the diagnosis of clinically significant mycobacterial infections. QFT-G is highly specific and a positive test is strongly predictive of true infection with M. tuberculosis complex (MTB). The test is approved as an aid for diagnosing both active TB disease and LTBI, but does not differentiate between the two. Who is eligible for testing? QFTG can be used in patients who have been evaluated for possible M. tuberculosis – complex infection, whether tuberculosis disease or LTBI. In other words it can be used in all circumstances where the tuberculosis skin test is considered.
Specific Sample requirements: Adults and children: 1ml of blood must be drawn directly into each of the three QuantiFERON-GOLD tubes in order, which must be all labelled with appropriate patient identifying information. (1) Nil control (GREY TOP), (2) TB Antigen (RED TOP), (3) Mitogen Control (PURPLE CAP)(Collection tubes available from outpatients Phlebotomy and Clinical Immunology) Samples must be delivered directly to the laboratory and must arrive between 08.00 and 17.00 Monday-Friday. No weekend or out of hours sample collection.Samples must be incubated at 37º c within 16 hrs of collection, and must be kept at room temperature prior to this. Please contact the laboratory for further
How are the results reported and interpreted?The diagnosis or exclusion of tuberculosis disease, and assessing the probability of LTBI, requires a combination of epidemiological, historical, medical, radiological and microbiological findings that should be taken into account when interpreting test results. See general guidance on the diagnosis and treatment of tuberculosis disease and LTBI (http://www.cdc.gov/nchstp/tb/) or the NICE guidance on tuberculosis: http://www.nice.org.uk/guidance/index.jsp?action=byID&o=13422.. QUANTIFERON-TB Gold results are reported as positive, negative or indeterminate. 1. Positive(ESAT-6 and/or CFP-10 and/or TB7.7 responsiveness detected): M. tuberculosis infection likely.See text above 2.Negative(No ESAT-6 or CFP-10 and/or TB7.7responsiveness detected): M. tuberculosis infection unlikely, but cannot be excluded especially when:1. any illness is consistent with tuberculosis disease 2.
information if requesting test from non-Addenbrookes locations.What are the current limitations of QFTG test?• Specimens for testing must be transferred to the laboratory for processing within 12 hours of venesection. • The test has not been extensively studied in many groups, such as those with immunodeficiency, those on immunosuppressive drugs and clinical conditions which may reduce immunocompetence including diabetes, silicosis, chronic renal failure, and haematological disorders, or malignancy. • The test has not been extensively evaluated in children or in pregnant women. • It has not been extensively tested in those who have been treated for latent TB infection or tuberculosis disease. • The ability of QFTG test to predict the risk of LTBI progression to tuberculosis disease has not been determined. The risk
likelihood of progression to disease (e.g. because of immunosuppression) is increased. See text above 3.Indeterminate Test not interpretable. Unable to determine a result due to lack of stimulatory response to the positive control. This may be due to technical error in sample acquisition or an unspecified reason related to the clinical picture of the patient. Immune suppression or underlying immunodeficiency
may be different in those positive for the QFTG test than in those with a positive tuberculous skin test. QFT-G is highly specific and a positive test is strongly predictive of true infection with M. tuberculosis complex (MTB). However it cannot distinguish between latent and active disease.
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
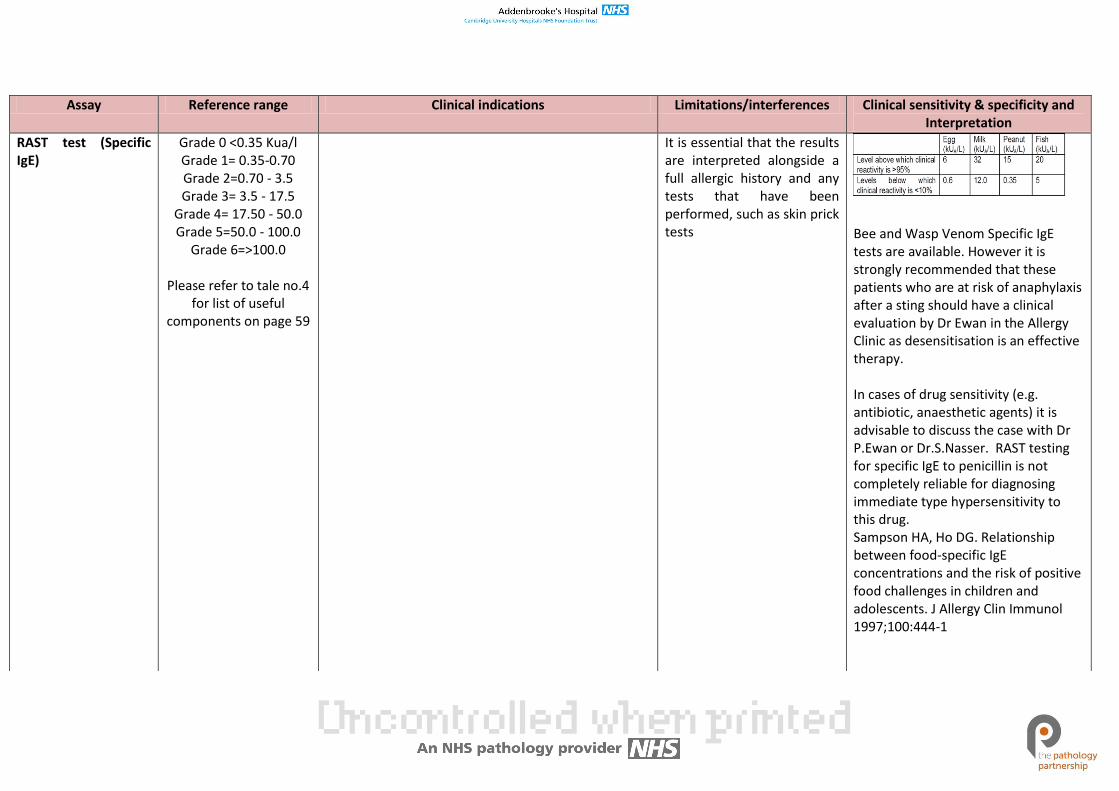
RAST test (Specific IgE)
Grade 0 <0.35 Kua/l Grade 1= 0.35-0.70 Grade 2=0.70 - 3.5 Grade 3= 3.5 - 17.5
Grade 4= 17.50 - 50.0 Grade 5=50.0 - 100.0
Grade 6=>100.0
Please refer to tale no.4 for list of useful
components on page 59
It is essential that the results are interpreted alongside a full allergic history and any tests that have been performed, such as skin prick tests
Bee and Wasp Venom Specific IgE tests are available. However it is strongly recommended that these patients who are at risk of anaphylaxis after a sting should have a clinical evaluation by Dr Ewan in the Allergy Clinic as desensitisation is an effective therapy. In cases of drug sensitivity (e.g. antibiotic, anaesthetic agents) it is advisable to discuss the case with Dr P.Ewan or Dr.S.Nasser. RAST testing for specific IgE to penicillin is not completely reliable for diagnosing immediate type hypersensitivity to this drug. Sampson HA, Ho DG. Relationship between food-specific IgE concentrations and the risk of positive food challenges in children and adolescents. J Allergy Clin Immunol 1997;100:444-1

Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
Rheumatoid factor (performed in biochemistry)
0- 14 iu/ml
In Rheumatoid Arthritis, the presence of a high titre RF at onset is of some predictive value as these patients have a worse prognosis than seronegative patients and are more likely to suffer from systemic manifestations of the disease than those who are RF negative. This test is of no value in monitoring RA; use CRP instead. A negative test for RF can be helpful in the differential diagnosis of rheumatic diseases as they are not usually detected in rheumatic fever, gout, Reiter's syndrome, ankylosing spondylitis, osteoarthritis, psoriatic arthritis and Juvenile Chronic Arthritis. Rheumatoid Factors are immunoglobulins which react with IgG and are found in a variety of conditions (viral infections, chronic bacterial infections, connective tissue diseases, lymphoproliferative disorders and low titres may be found in normal elderly people) and by themselves are of low diagnostic value.
Positive rheumatoid factor is not specific for rheumatoid arthritis, and can be found in other connective tissue diseases (e.g. Sjogren's, lupus), infections, and in up to 15% of the normal population. Interpretation of Rheumatoid factor in patients suspected with Rheumatoid Arthritis: Result Relative risk of Rheumatoid arthritis 25-50 Iu/ml 3.6 (95% Confidence interval: 1.7-7.3) 50-100 IU/ml 6 (95% Confidence interval: 3.4-10) >100 IU/ml 26 (95% Confidence interval: 15-46) (Reference: BMJ 2012 , vol 345, e5244)
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
Scleroderma antibodies
N/A Scl-70,CENP A,CENP B ,RP11,RP155,Fibrillarin,NOR90,Th/To,PM-Scl100,PM-Scl75,Ku,PDGFR.Ro-52, are scleroderma specific and/or associated antbodies which can be tested for by immunoblotting if specifically requested on clinical grounds, or as a follow-up investigation RNA Polmerase 3. Antibodies( RP11 and RP155 subunits) and fibrillarin have a high specificity for Systemic Sclerosis. Th/To-antibodies are found in patients with Systemic sclerosis,predominantly the limited cutaneous form but also with Primary Raynauds phenomenon,SLE,Polymyositis and RA NOR-Nucleolar Organising Region 90 antibodies are rare and are associated with patients with Scleroderma and Raynauds phenomenon.
This test will be accompanied by a ANA HEp-2 which is essential for the intrepetation of the myositis autoantibody line blot assay
Serum Free light chains
3.30 – 19.4 mg/l (Serum kappa free light chain)
5.71 – 26.3 mg/l (serum lambda free light chain)
0.26 – 1.65 kappa:lambda ratio
Guidelines for the management and monitoring of myeloma suggest that serum FLCs may be useful in monitoring free light chain only myeloma. Abnormal FLC levels and ratio can be found in multiple myeloma, Bence Jones proteinuria, non-secretory myelomas, free light chain disease and primary amyloidosis. Serum concentrations of FLCs are dependent on the balance between production and renal clearance. Elevated levels of both free kappa and free lambda light chain can be found in renal failure (due to decreased loss in urine) or in inflammation (increased synthesis). In these conditions kappa and lambda are affected equally.
Haemolysis, grossly lipaemic or icteric samples.
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
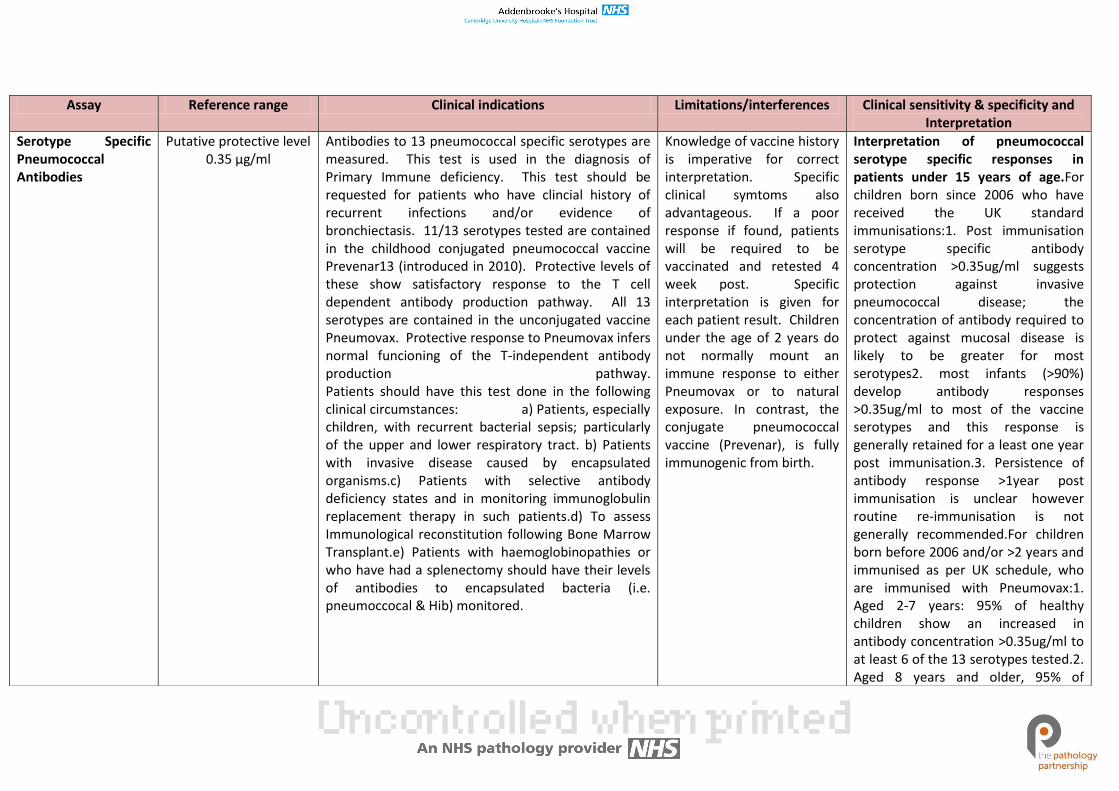
Serotype Specific Pneumococcal Antibodies
Putative protective level 0.35 µg/ml
Antibodies to 13 pneumococcal specific serotypes are measured. This test is used in the diagnosis of Primary Immune deficiency. This test should be requested for patients who have clincial history of recurrent infections and/or evidence of bronchiectasis. 11/13 serotypes tested are contained in the childhood conjugated pneumococcal vaccine Prevenar13 (introduced in 2010). Protective levels of these show satisfactory response to the T cell dependent antibody production pathway. All 13 serotypes are contained in the unconjugated vaccine Pneumovax. Protective response to Pneumovax infers normal funcioning of the T-independent antibody production pathway. Patients should have this test done in the following clinical circumstances: a) Patients, especially children, with recurrent bacterial sepsis; particularly of the upper and lower respiratory tract. b) Patients with invasive disease caused by encapsulated organisms.c) Patients with selective antibody deficiency states and in monitoring immunoglobulin replacement therapy in such patients.d) To assess Immunological reconstitution following Bone Marrow Transplant.e) Patients with haemoglobinopathies or who have had a splenectomy should have their levels of antibodies to encapsulated bacteria (i.e. pneumoccocal & Hib) monitored.
Knowledge of vaccine history is imperative for correct interpretation. Specific clinical symtoms also advantageous. If a poor response if found, patients will be required to be vaccinated and retested 4 week post. Specific interpretation is given for each patient result. Children under the age of 2 years do not normally mount an immune response to either Pneumovax or to natural exposure. In contrast, the conjugate pneumococcal vaccine (Prevenar), is fully immunogenic from birth.
Interpretation of pneumococcal serotype specific responses in patients under 15 years of age.For children born since 2006 who have received the UK standard immunisations:1. Post immunisation serotype specific antibody concentration >0.35ug/ml suggests protection against invasive pneumococcal disease; the concentration of antibody required to protect against mucosal disease is likely to be greater for most serotypes2. most infants (>90%) develop antibody responses >0.35ug/ml to most of the vaccine serotypes and this response is generally retained for a least one year post immunisation.3. Persistence of antibody response >1year post immunisation is unclear however routine re-immunisation is not generally recommended.For children born before 2006 and/or >2 years and immunised as per UK schedule, who are immunised with Pneumovax:1. Aged 2-7 years: 95% of healthy children show an increased in antibody concentration >0.35ug/ml to at least 6 of the 13 serotypes tested.2. Aged 8 years and older, 95% of
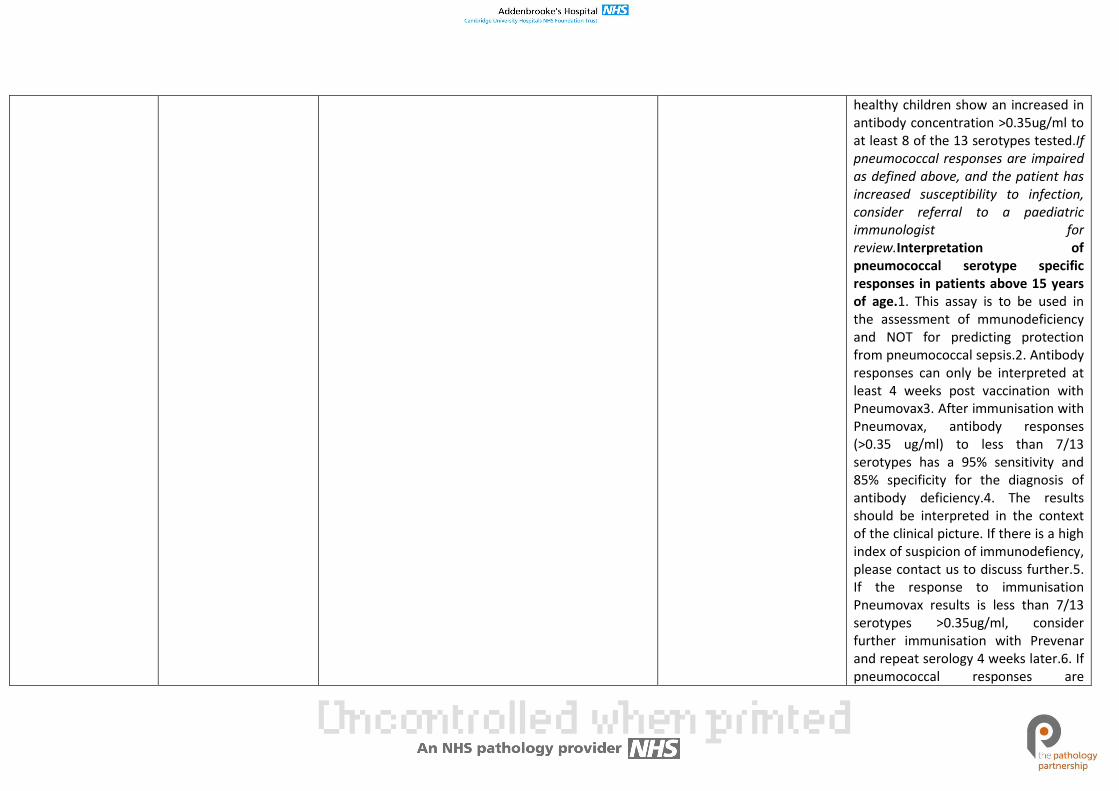
healthy children show an increased in antibody concentration >0.35ug/ml to at least 8 of the 13 serotypes tested.If pneumococcal responses are impaired as defined above, and the patient has increased susceptibility to infection, consider referral to a paediatric immunologist for review.Interpretation of pneumococcal serotype specific responses in patients above 15 years of age.1. This assay is to be used in the assessment of mmunodeficiency and NOT for predicting protection from pneumococcal sepsis.2. Antibody responses can only be interpreted at least 4 weeks post vaccination with Pneumovax3. After immunisation with Pneumovax, antibody responses (>0.35 ug/ml) to less than 7/13 serotypes has a 95% sensitivity and 85% specificity for the diagnosis of antibody deficiency.4. The results should be interpreted in the context of the clinical picture. If there is a high index of suspicion of immunodefiency, please contact us to discuss further.5. If the response to immunisation Pneumovax results is less than 7/13 serotypes >0.35ug/ml, consider further immunisation with Prevenar and repeat serology 4 weeks later.6. If pneumococcal responses are
abnormal as defined above, consider referral to an immunologist.Note: Prevenar is a more powerful immunogen than Pneumovax and activates T cell dependent antibody responses. Therefore antibody responses to Prevenar cannot be used to evaluate thymus independent responses to polysaccharides.
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
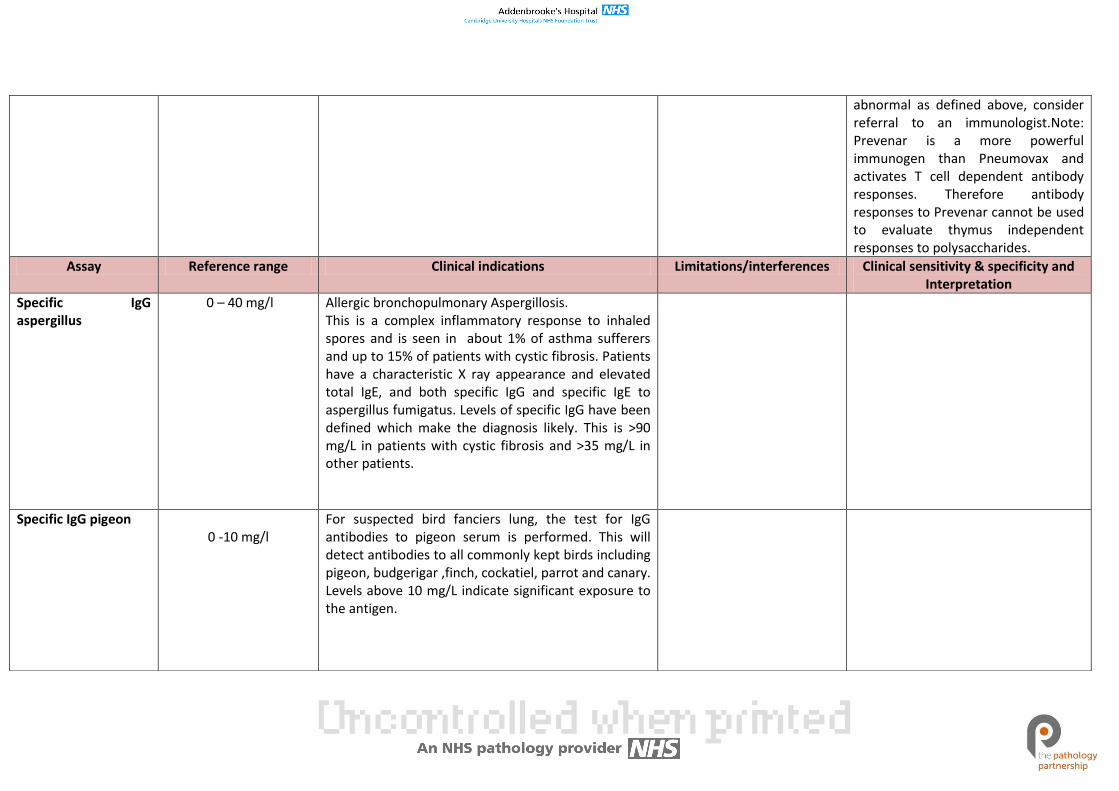
Specific IgG aspergillus
0 – 40 mg/l Allergic bronchopulmonary Aspergillosis. This is a complex inflammatory response to inhaled spores and is seen in about 1% of asthma sufferers and up to 15% of patients with cystic fibrosis. Patients have a characteristic X ray appearance and elevated total IgE, and both specific IgG and specific IgE to aspergillus fumigatus. Levels of specific IgG have been defined which make the diagnosis likely. This is >90 mg/L in patients with cystic fibrosis and >35 mg/L in other patients.
Specific IgG pigeon 0 -10 mg/l
For suspected bird fanciers lung, the test for IgG antibodies to pigeon serum is performed. This will detect antibodies to all commonly kept birds including pigeon, budgerigar ,finch, cockatiel, parrot and canary. Levels above 10 mg/L indicate significant exposure to the antigen.
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
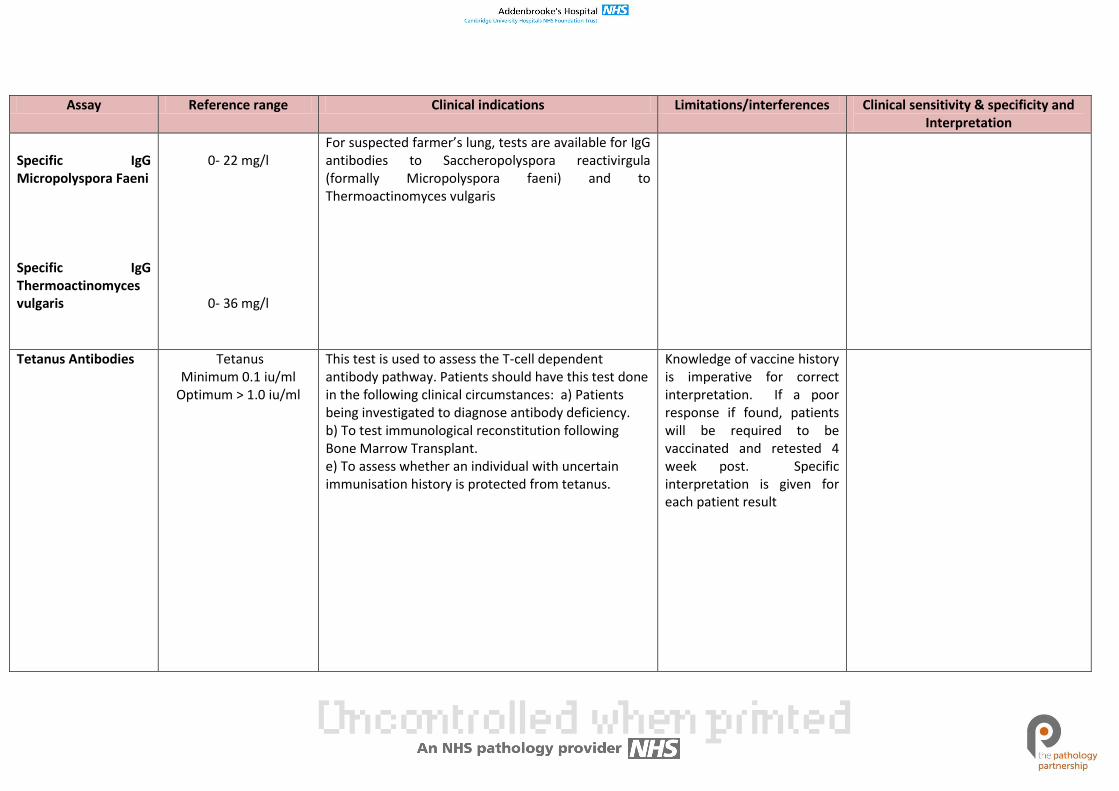
Specific IgG Micropolyspora Faeni Specific IgG Thermoactinomyces vulgaris
0- 22 mg/l
0- 36 mg/l
For suspected farmer’s lung, tests are available for IgG antibodies to Saccheropolyspora reactivirgula (formally Micropolyspora faeni) and to Thermoactinomyces vulgaris
Tetanus Antibodies Tetanus Minimum 0.1 iu/ml
Optimum > 1.0 iu/ml
This test is used to assess the T-cell dependent antibody pathway. Patients should have this test done in the following clinical circumstances: a) Patients being investigated to diagnose antibody deficiency. b) To test immunological reconstitution following Bone Marrow Transplant. e) To assess whether an individual with uncertain immunisation history is protected from tetanus.
Knowledge of vaccine history is imperative for correct interpretation. If a poor response if found, patients will be required to be vaccinated and retested 4 week post. Specific interpretation is given for each patient result
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
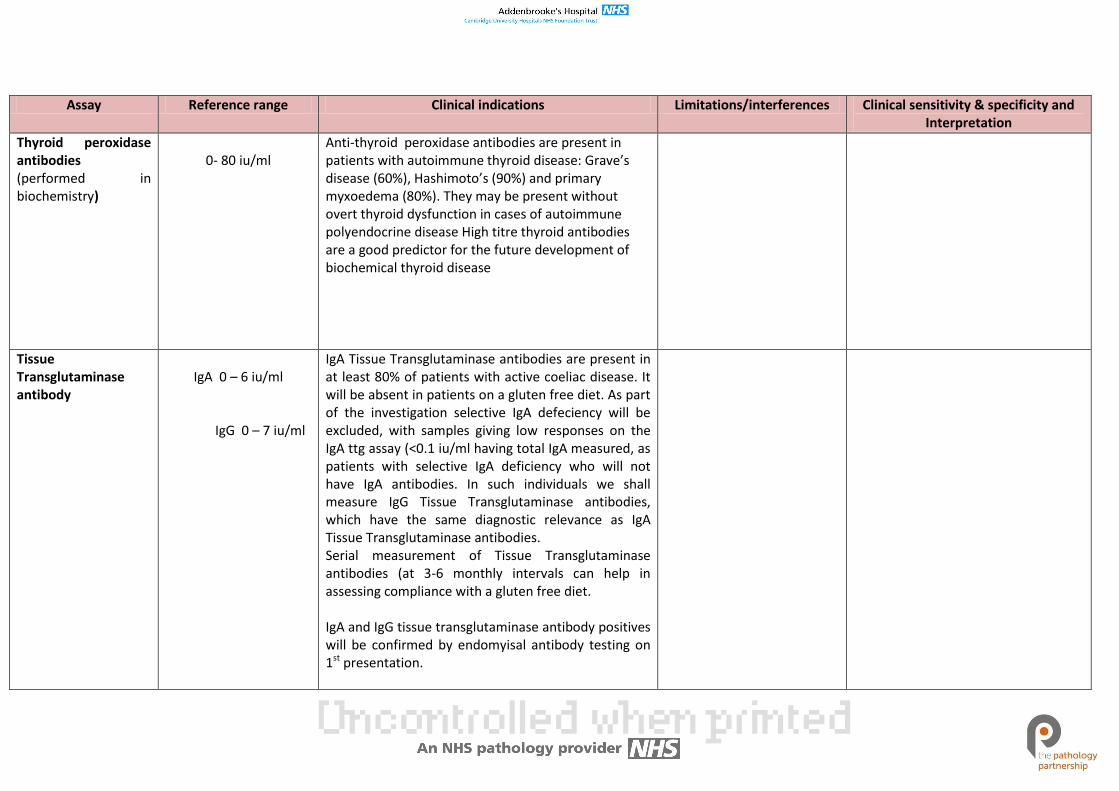
Thyroid peroxidase antibodies (performed in biochemistry)
0- 80 iu/ml
Anti-thyroid peroxidase antibodies are present in patients with autoimmune thyroid disease: Grave’s disease (60%), Hashimoto’s (90%) and primary myxoedema (80%). They may be present without overt thyroid dysfunction in cases of autoimmune polyendocrine disease High titre thyroid antibodies are a good predictor for the future development of biochemical thyroid disease
Tissue Transglutaminase antibody
IgA 0 – 6 iu/ml
IgG 0 – 7 iu/ml
IgA Tissue Transglutaminase antibodies are present in at least 80% of patients with active coeliac disease. It will be absent in patients on a gluten free diet. As part of the investigation selective IgA defeciency will be excluded, with samples giving low responses on the IgA ttg assay (<0.1 iu/ml having total IgA measured, as patients with selective IgA deficiency who will not have IgA antibodies. In such individuals we shall measure IgG Tissue Transglutaminase antibodies, which have the same diagnostic relevance as IgA Tissue Transglutaminase antibodies. Serial measurement of Tissue Transglutaminase antibodies (at 3-6 monthly intervals can help in assessing compliance with a gluten free diet. IgA and IgG tissue transglutaminase antibody positives will be confirmed by endomyisal antibody testing on 1st presentation.
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
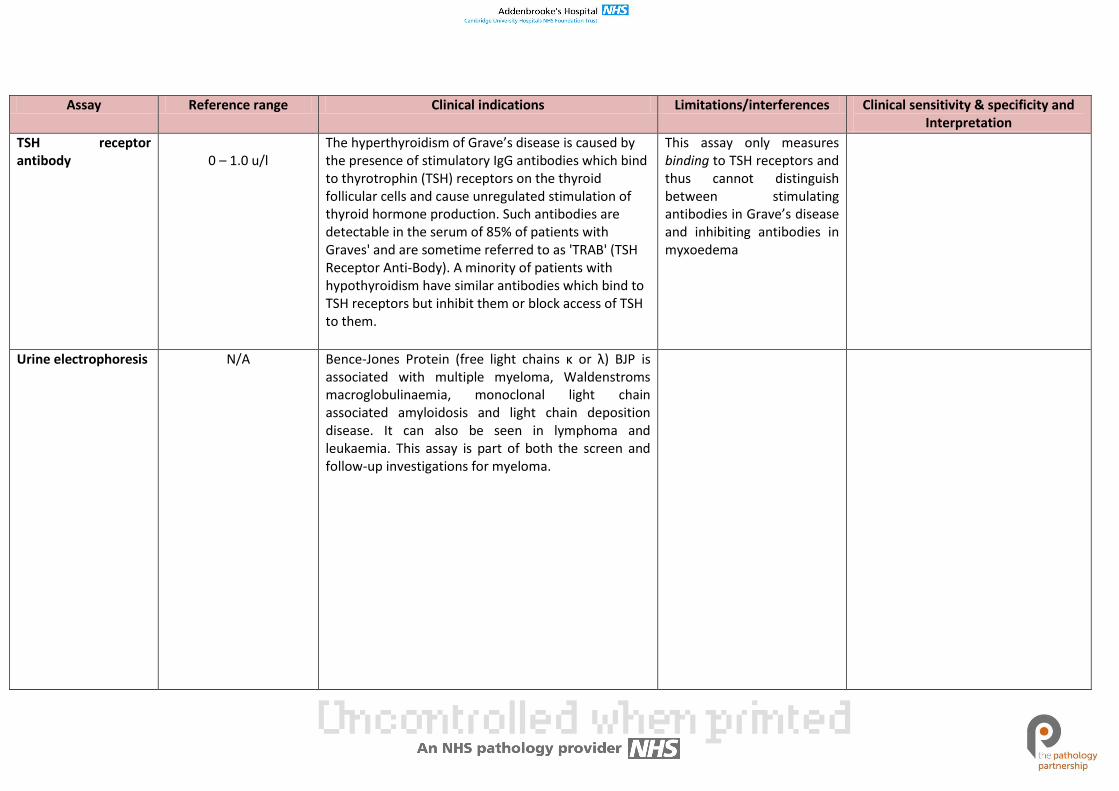
TSH receptor antibody
0 – 1.0 u/l
The hyperthyroidism of Grave’s disease is caused by the presence of stimulatory IgG antibodies which bind to thyrotrophin (TSH) receptors on the thyroid follicular cells and cause unregulated stimulation of thyroid hormone production. Such antibodies are detectable in the serum of 85% of patients with Graves' and are sometime referred to as 'TRAB' (TSH Receptor Anti-Body). A minority of patients with hypothyroidism have similar antibodies which bind to TSH receptors but inhibit them or block access of TSH to them.
This assay only measures binding to TSH receptors and thus cannot distinguish between stimulating antibodies in Grave’s disease and inhibiting antibodies in myxoedema
Urine electrophoresis N/A Bence-Jones Protein (free light chains κ or λ) BJP is associated with multiple myeloma, Waldenstroms macroglobulinaemia, monoclonal light chain associated amyloidosis and light chain deposition disease. It can also be seen in lymphoma and leukaemia. This assay is part of both the screen and follow-up investigations for myeloma.
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
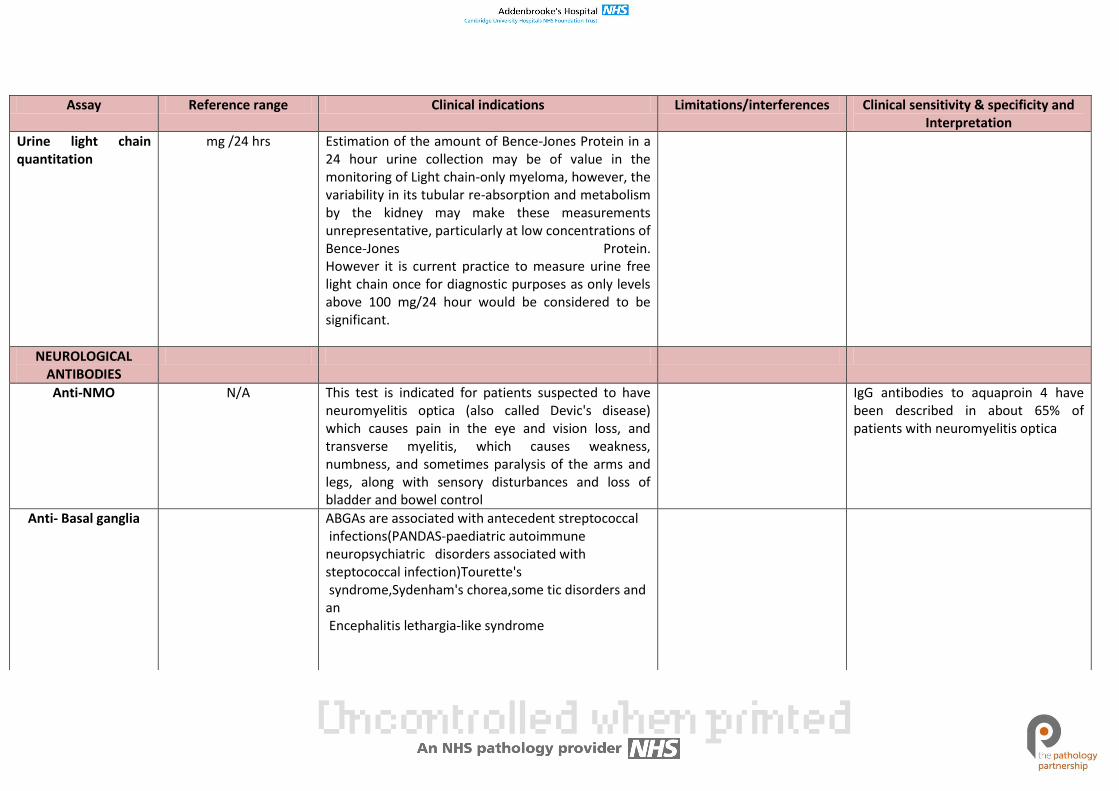
Urine light chain quantitation
mg /24 hrs Estimation of the amount of Bence-Jones Protein in a 24 hour urine collection may be of value in the monitoring of Light chain-only myeloma, however, the variability in its tubular re-absorption and metabolism by the kidney may make these measurements unrepresentative, particularly at low concentrations of Bence-Jones Protein. However it is current practice to measure urine free light chain once for diagnostic purposes as only levels above 100 mg/24 hour would be considered to be significant.
NEUROLOGICAL ANTIBODIES
Anti-NMO N/A This test is indicated for patients suspected to have neuromyelitis optica (also called Devic's disease) which causes pain in the eye and vision loss, and transverse myelitis, which causes weakness, numbness, and sometimes paralysis of the arms and legs, along with sensory disturbances and loss of bladder and bowel control
IgG antibodies to aquaproin 4 have been described in about 65% of patients with neuromyelitis optica
Anti- Basal ganglia ABGAs are associated with antecedent streptococcal infections(PANDAS-paediatric autoimmune neuropsychiatric disorders associated with steptococcal infection)Tourette's syndrome,Sydenham's chorea,some tic disorders and an Encephalitis lethargia-like syndrome
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
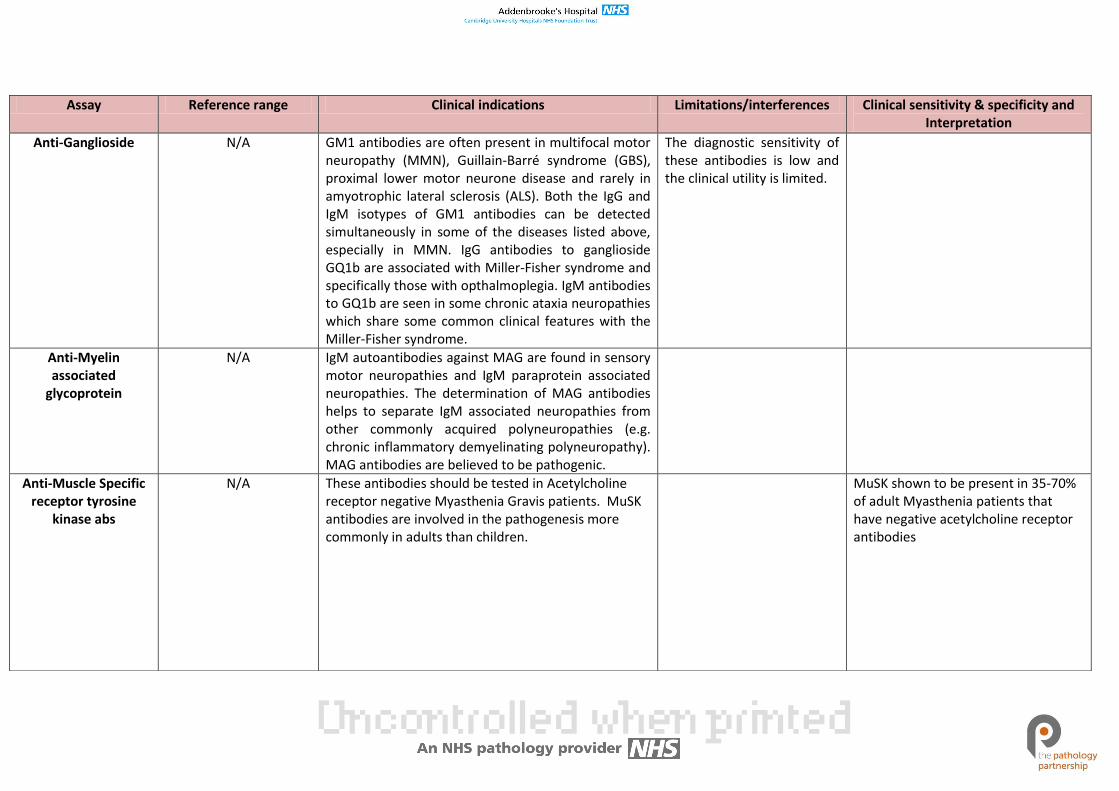
Anti-Ganglioside N/A GM1 antibodies are often present in multifocal motor neuropathy (MMN), Guillain-Barré syndrome (GBS), proximal lower motor neurone disease and rarely in amyotrophic lateral sclerosis (ALS). Both the IgG and IgM isotypes of GM1 antibodies can be detected simultaneously in some of the diseases listed above, especially in MMN. IgG antibodies to ganglioside GQ1b are associated with Miller-Fisher syndrome and specifically those with opthalmoplegia. IgM antibodies to GQ1b are seen in some chronic ataxia neuropathies which share some common clinical features with the Miller-Fisher syndrome.
The diagnostic sensitivity of these antibodies is low and the clinical utility is limited.
Anti-Myelin associated
glycoprotein
N/A IgM autoantibodies against MAG are found in sensory motor neuropathies and IgM paraprotein associated neuropathies. The determination of MAG antibodies helps to separate IgM associated neuropathies from other commonly acquired polyneuropathies (e.g. chronic inflammatory demyelinating polyneuropathy). MAG antibodies are believed to be pathogenic.
Anti-Muscle Specific receptor tyrosine
kinase abs
N/A These antibodies should be tested in Acetylcholine receptor negative Myasthenia Gravis patients. MuSK antibodies are involved in the pathogenesis more commonly in adults than children.
MuSK shown to be present in 35-70% of adult Myasthenia patients that have negative acetylcholine receptor antibodies
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
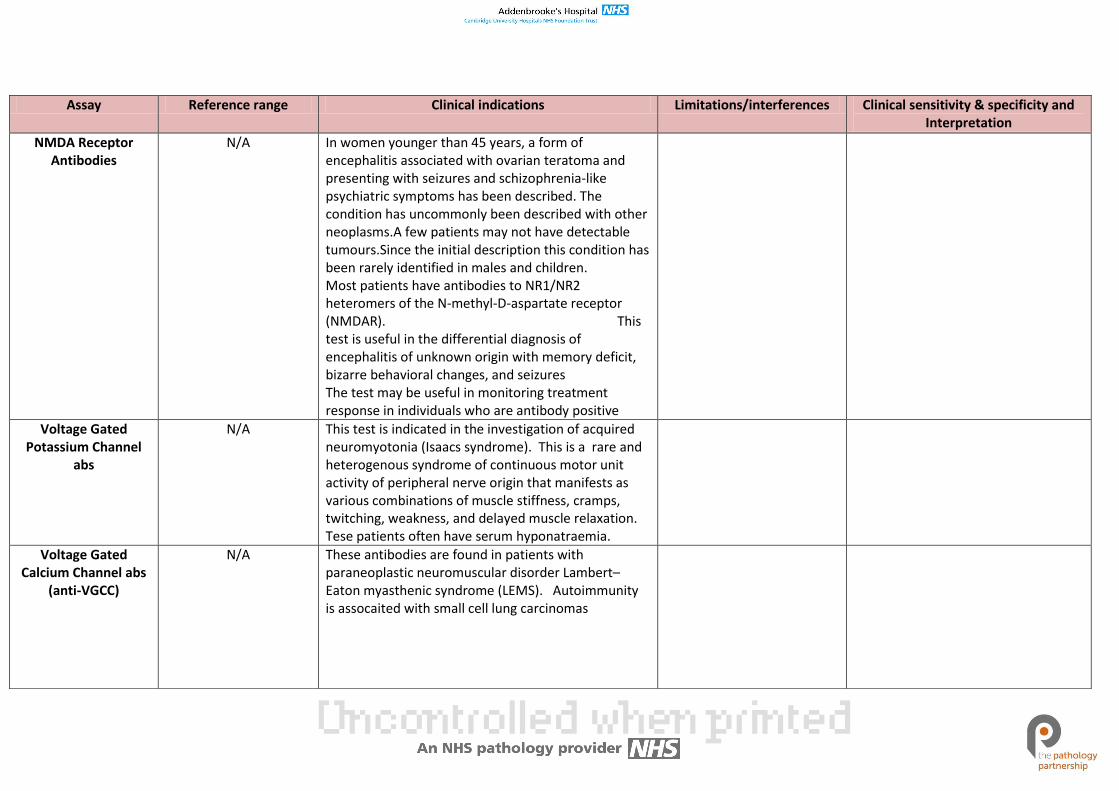
NMDA Receptor Antibodies
N/A In women younger than 45 years, a form of encephalitis associated with ovarian teratoma and presenting with seizures and schizophrenia-like psychiatric symptoms has been described. The condition has uncommonly been described with other neoplasms.A few patients may not have detectable tumours.Since the initial description this condition has been rarely identified in males and children. Most patients have antibodies to NR1/NR2 heteromers of the N-methyl-D-aspartate receptor (NMDAR). This test is useful in the differential diagnosis of encephalitis of unknown origin with memory deficit, bizarre behavioral changes, and seizures The test may be useful in monitoring treatment response in individuals who are antibody positive
Voltage Gated Potassium Channel
abs
N/A This test is indicated in the investigation of acquired neuromyotonia (Isaacs syndrome). This is a rare and heterogenous syndrome of continuous motor unit activity of peripheral nerve origin that manifests as various combinations of muscle stiffness, cramps, twitching, weakness, and delayed muscle relaxation. Tese patients often have serum hyponatraemia.
Voltage Gated Calcium Channel abs
(anti-VGCC)
N/A These antibodies are found in patients with paraneoplastic neuromuscular disorder Lambert–Eaton myasthenic syndrome (LEMS). Autoimmunity is assocaited with small cell lung carcinomas
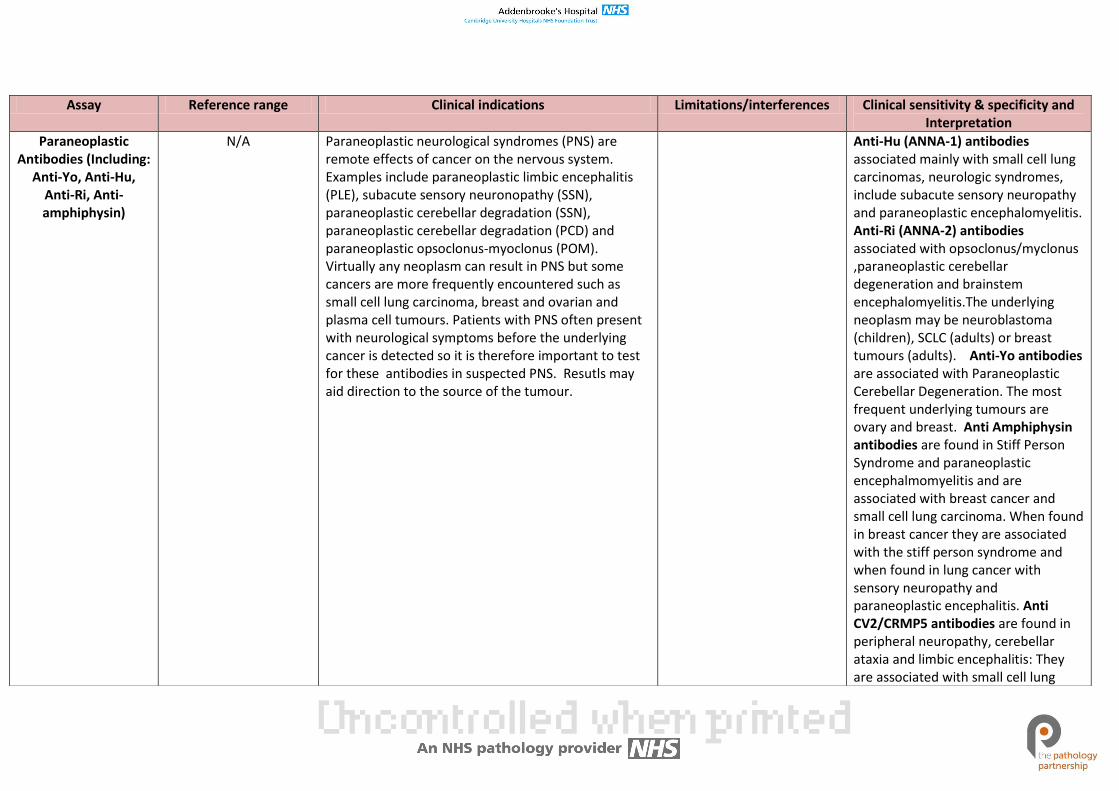
Assay Reference range Clinical indications Limitations/interferences Clinical sensitivity & specificity and Interpretation
Paraneoplastic Antibodies (Including:
Anti-Yo, Anti-Hu, Anti-Ri, Anti-amphiphysin)
N/A Paraneoplastic neurological syndromes (PNS) are remote effects of cancer on the nervous system. Examples include paraneoplastic limbic encephalitis (PLE), subacute sensory neuronopathy (SSN), paraneoplastic cerebellar degradation (SSN), paraneoplastic cerebellar degradation (PCD) and paraneoplastic opsoclonus-myoclonus (POM). Virtually any neoplasm can result in PNS but some cancers are more frequently encountered such as small cell lung carcinoma, breast and ovarian and plasma cell tumours. Patients with PNS often present with neurological symptoms before the underlying cancer is detected so it is therefore important to test for these antibodies in suspected PNS. Resutls may aid direction to the source of the tumour.
Anti-Hu (ANNA-1) antibodies associated mainly with small cell lung carcinomas, neurologic syndromes, include subacute sensory neuropathy and paraneoplastic encephalomyelitis. Anti-Ri (ANNA-2) antibodies associated with opsoclonus/myclonus ,paraneoplastic cerebellar degeneration and brainstem encephalomyelitis.The underlying neoplasm may be neuroblastoma (children), SCLC (adults) or breast tumours (adults). Anti-Yo antibodies are associated with Paraneoplastic Cerebellar Degeneration. The most frequent underlying tumours are ovary and breast. Anti Amphiphysin antibodies are found in Stiff Person Syndrome and paraneoplastic encephalmomyelitis and are associated with breast cancer and small cell lung carcinoma. When found in breast cancer they are associated with the stiff person syndrome and when found in lung cancer with sensory neuropathy and paraneoplastic encephalitis. Anti CV2/CRMP5 antibodies are found in peripheral neuropathy, cerebellar ataxia and limbic encephalitis: They are associated with small cell lung
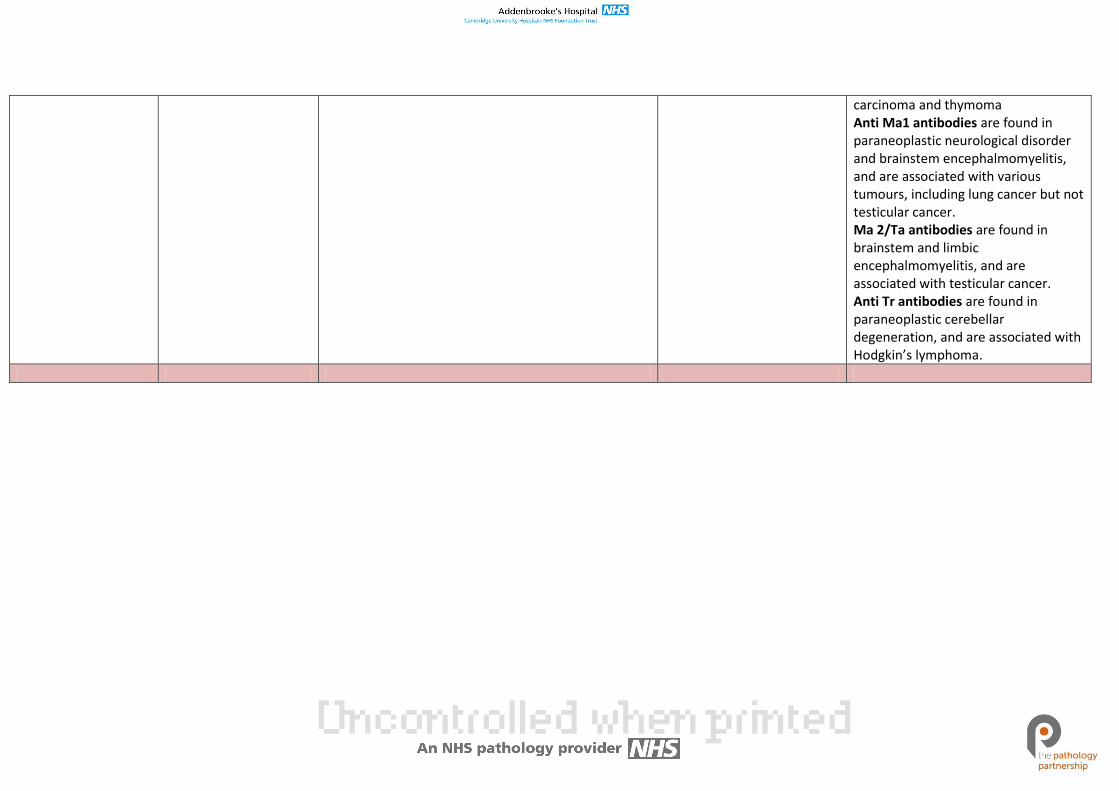
carcinoma and thymoma Anti Ma1 antibodies are found in paraneoplastic neurological disorder and brainstem encephalmomyelitis, and are associated with various tumours, including lung cancer but not testicular cancer. Ma 2/Ta antibodies are found in brainstem and limbic encephalmomyelitis, and are associated with testicular cancer. Anti Tr antibodies are found in paraneoplastic cerebellar degeneration, and are associated with Hodgkin’s lymphoma.
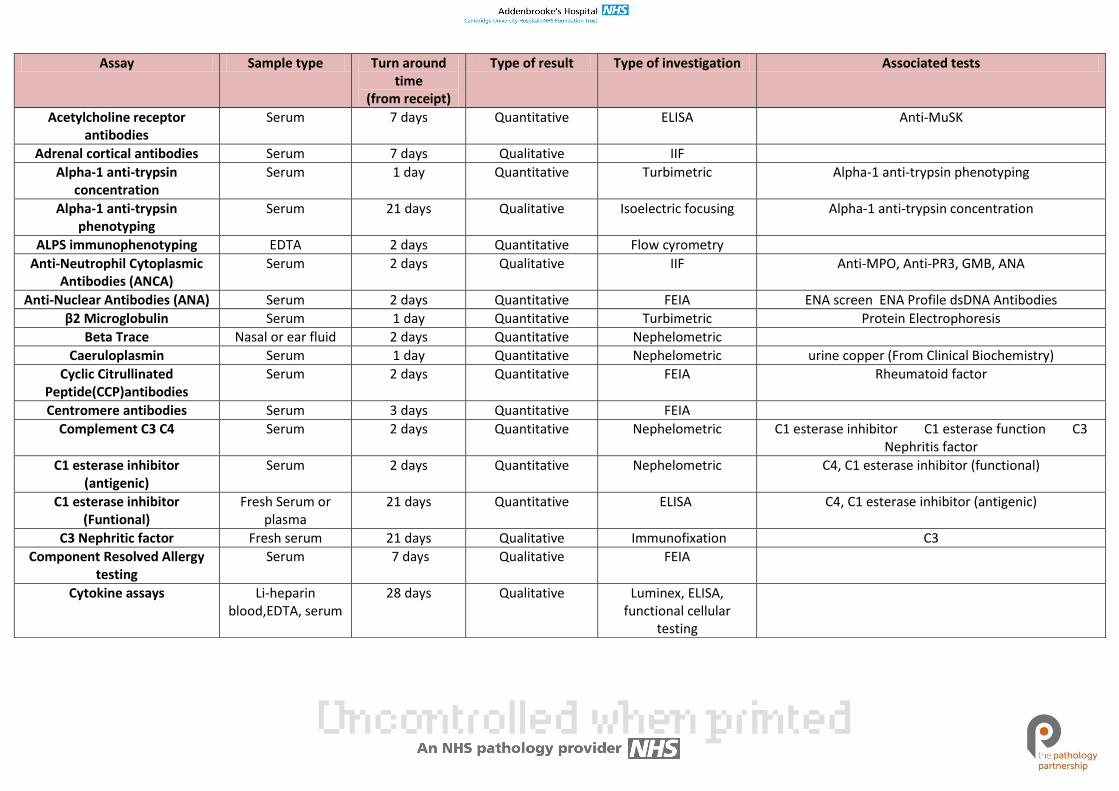
Assay Sample type Turn around time
(from receipt)
Type of result Type of investigation Associated tests
Acetylcholine receptor antibodies
Serum 7 days Quantitative ELISA Anti-MuSK
Adrenal cortical antibodies Serum 7 days Qualitative IIF
Alpha-1 anti-trypsin concentration
Serum 1 day Quantitative Turbimetric Alpha-1 anti-trypsin phenotyping
Alpha-1 anti-trypsin phenotyping
Serum 21 days Qualitative Isoelectric focusing Alpha-1 anti-trypsin concentration
ALPS immunophenotyping EDTA 2 days Quantitative Flow cyrometry
Anti-Neutrophil Cytoplasmic Antibodies (ANCA)
Serum 2 days Qualitative IIF Anti-MPO, Anti-PR3, GMB, ANA
Anti-Nuclear Antibodies (ANA) Serum 2 days Quantitative FEIA ENA screen ENA Profile dsDNA Antibodies
β2 Microglobulin Serum 1 day Quantitative Turbimetric Protein Electrophoresis
Beta Trace Nasal or ear fluid 2 days Quantitative Nephelometric
Caeruloplasmin Serum 1 day Quantitative Nephelometric urine copper (From Clinical Biochemistry)
Cyclic Citrullinated Peptide(CCP)antibodies
Serum 2 days Quantitative FEIA Rheumatoid factor
Centromere antibodies Serum 3 days Quantitative FEIA
Complement C3 C4 Serum 2 days Quantitative Nephelometric C1 esterase inhibitor C1 esterase function C3 Nephritis factor
C1 esterase inhibitor (antigenic)
Serum 2 days Quantitative Nephelometric C4, C1 esterase inhibitor (functional)
C1 esterase inhibitor (Funtional)
Fresh Serum or plasma
21 days Quantitative ELISA C4, C1 esterase inhibitor (antigenic)
C3 Nephritic factor Fresh serum 21 days Qualitative Immunofixation C3
Component Resolved Allergy testing
Serum 7 days Qualitative FEIA
Cytokine assays Li-heparin blood,EDTA, serum
28 days Qualitative Luminex, ELISA, functional cellular
testing
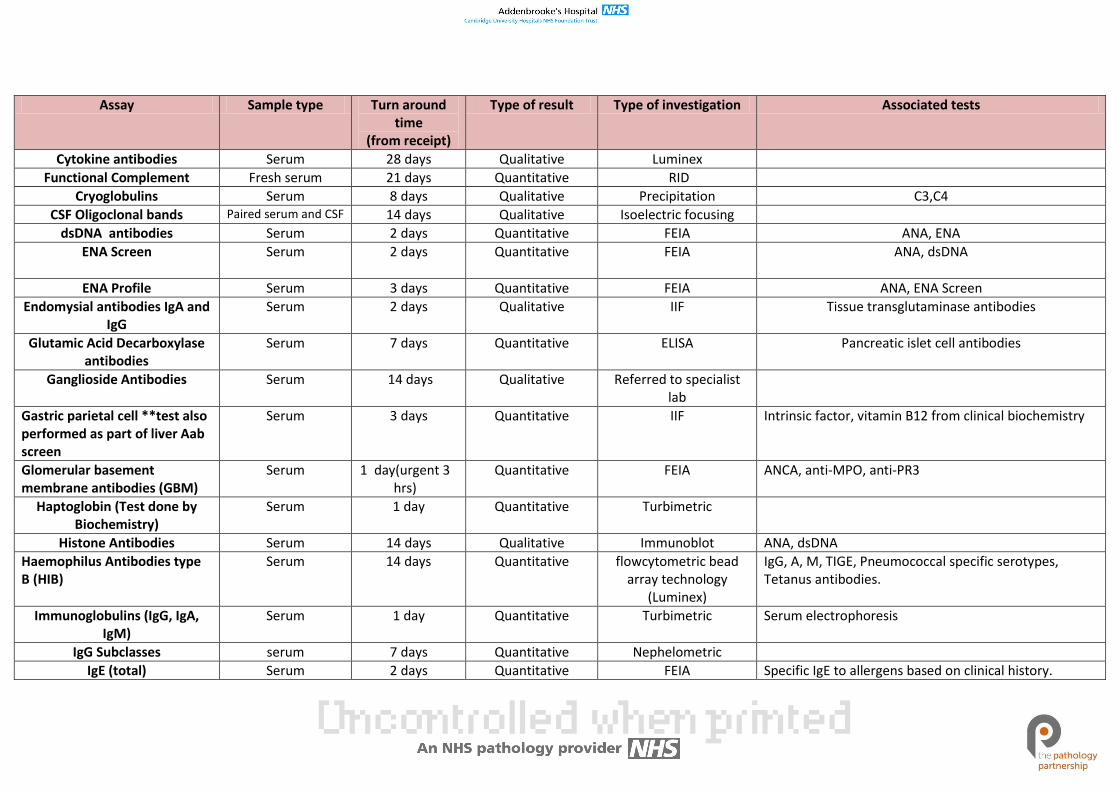
Assay Sample type Turn around time
(from receipt)
Type of result Type of investigation Associated tests
Cytokine antibodies Serum 28 days Qualitative Luminex
Functional Complement Fresh serum 21 days Quantitative RID
Cryoglobulins Serum 8 days Qualitative Precipitation C3,C4
CSF Oligoclonal bands Paired serum and CSF 14 days Qualitative Isoelectric focusing
dsDNA antibodies Serum 2 days Quantitative FEIA ANA, ENA
ENA Screen Serum 2 days Quantitative FEIA ANA, dsDNA
ENA Profile Serum 3 days Quantitative FEIA ANA, ENA Screen
Endomysial antibodies IgA and IgG
Serum 2 days Qualitative IIF Tissue transglutaminase antibodies
Glutamic Acid Decarboxylase antibodies
Serum 7 days Quantitative ELISA Pancreatic islet cell antibodies
Ganglioside Antibodies Serum 14 days Qualitative Referred to specialist lab
Gastric parietal cell **test also performed as part of liver Aab screen
Serum 3 days Quantitative IIF Intrinsic factor, vitamin B12 from clinical biochemistry
Glomerular basement membrane antibodies (GBM)
Serum 1 day(urgent 3 hrs)
Quantitative FEIA ANCA, anti-MPO, anti-PR3
Haptoglobin (Test done by Biochemistry)
Serum 1 day Quantitative Turbimetric
Histone Antibodies Serum 14 days Qualitative Immunoblot ANA, dsDNA
Haemophilus Antibodies type B (HIB)
Serum 14 days Quantitative flowcytometric bead array technology
(Luminex)
IgG, A, M, TIGE, Pneumococcal specific serotypes, Tetanus antibodies.
Immunoglobulins (IgG, IgA, IgM)
Serum 1 day Quantitative Turbimetric Serum electrophoresis
IgG Subclasses serum 7 days Quantitative Nephelometric
IgE (total) Serum 2 days Quantitative FEIA Specific IgE to allergens based on clinical history.
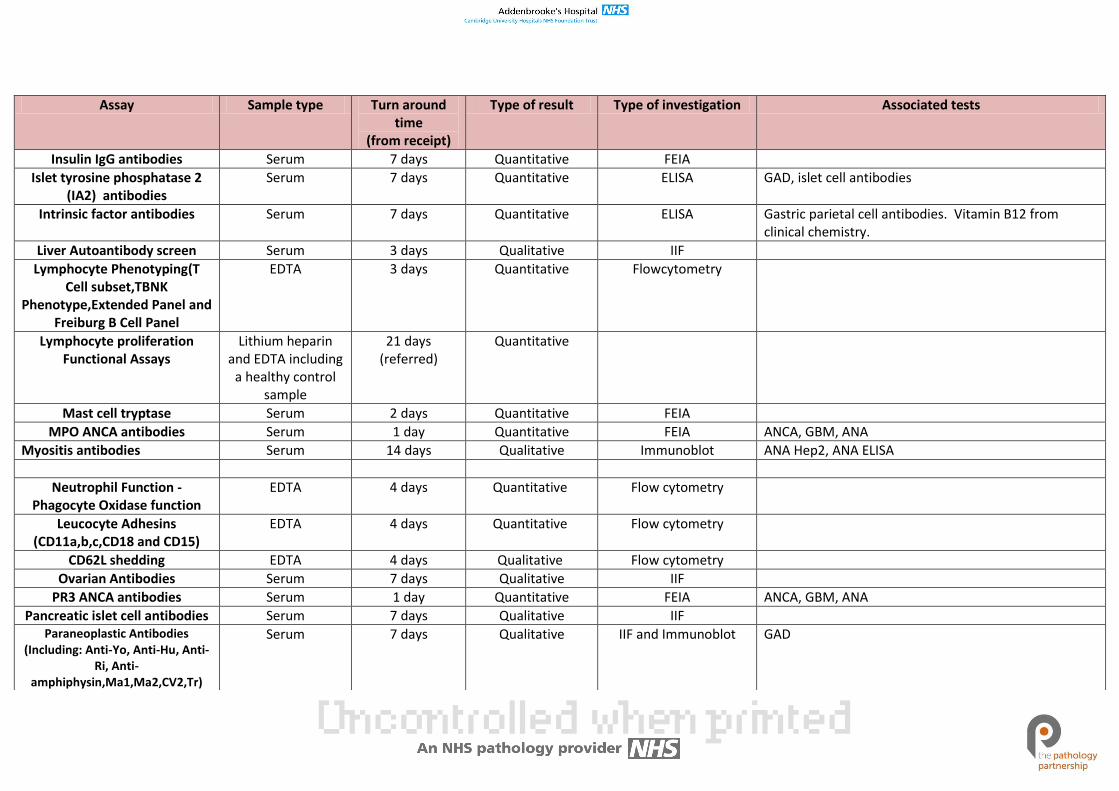
Assay Sample type Turn around time
(from receipt)
Type of result Type of investigation Associated tests
Insulin IgG antibodies Serum 7 days Quantitative FEIA
Islet tyrosine phosphatase 2 (IA2) antibodies
Serum 7 days Quantitative ELISA GAD, islet cell antibodies
Intrinsic factor antibodies Serum 7 days Quantitative ELISA Gastric parietal cell antibodies. Vitamin B12 from clinical chemistry.
Liver Autoantibody screen Serum 3 days Qualitative IIF
Lymphocyte Phenotyping(T Cell subset,TBNK
Phenotype,Extended Panel and Freiburg B Cell Panel
EDTA 3 days Quantitative Flowcytometry
Lymphocyte proliferation Functional Assays
Lithium heparin and EDTA including
a healthy control sample
21 days (referred)
Quantitative
Mast cell tryptase Serum 2 days Quantitative FEIA
MPO ANCA antibodies Serum 1 day Quantitative FEIA ANCA, GBM, ANA
Myositis antibodies Serum 14 days Qualitative Immunoblot ANA Hep2, ANA ELISA
Neutrophil Function - Phagocyte Oxidase function
EDTA 4 days Quantitative Flow cytometry
Leucocyte Adhesins (CD11a,b,c,CD18 and CD15)
EDTA 4 days Quantitative Flow cytometry
CD62L shedding EDTA 4 days Qualitative Flow cytometry
Ovarian Antibodies Serum 7 days Qualitative IIF
PR3 ANCA antibodies Serum 1 day Quantitative FEIA ANCA, GBM, ANA
Pancreatic islet cell antibodies Serum 7 days Qualitative IIF Paraneoplastic Antibodies
(Including: Anti-Yo, Anti-Hu, Anti-Ri, Anti-
amphiphysin,Ma1,Ma2,CV2,Tr)
Serum 7 days Qualitative IIF and Immunoblot GAD
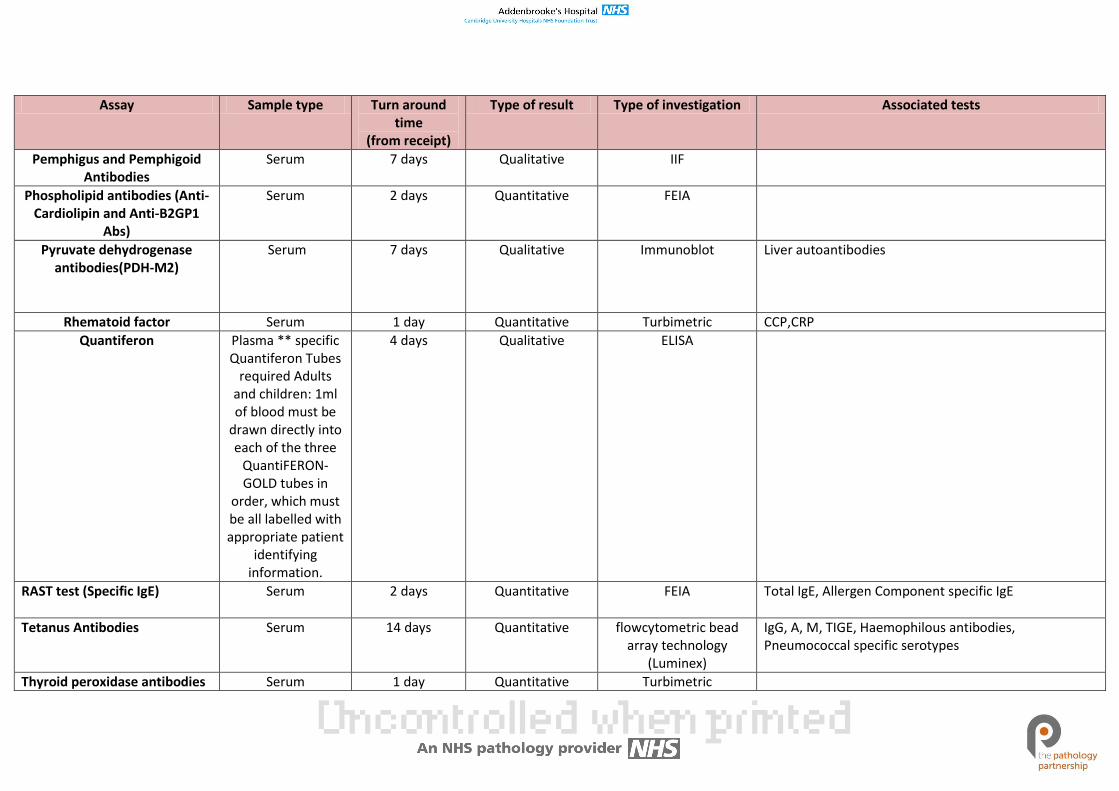
Assay Sample type Turn around time
(from receipt)
Type of result Type of investigation Associated tests
Pemphigus and Pemphigoid Antibodies
Serum 7 days Qualitative IIF
Phospholipid antibodies (Anti-Cardiolipin and Anti-B2GP1
Abs)
Serum 2 days Quantitative FEIA
Pyruvate dehydrogenase antibodies(PDH-M2)
Serum 7 days Qualitative Immunoblot Liver autoantibodies
Rhematoid factor Serum 1 day Quantitative Turbimetric CCP,CRP
Quantiferon Plasma ** specific Quantiferon Tubes
required Adults and children: 1ml of blood must be
drawn directly into each of the three
QuantiFERON-GOLD tubes in
order, which must be all labelled with appropriate patient
identifying information.
4 days Qualitative ELISA
RAST test (Specific IgE) Serum 2 days Quantitative FEIA Total IgE, Allergen Component specific IgE
Tetanus Antibodies Serum 14 days Quantitative flowcytometric bead array technology
(Luminex)
IgG, A, M, TIGE, Haemophilous antibodies, Pneumococcal specific serotypes
Thyroid peroxidase antibodies Serum 1 day Quantitative Turbimetric
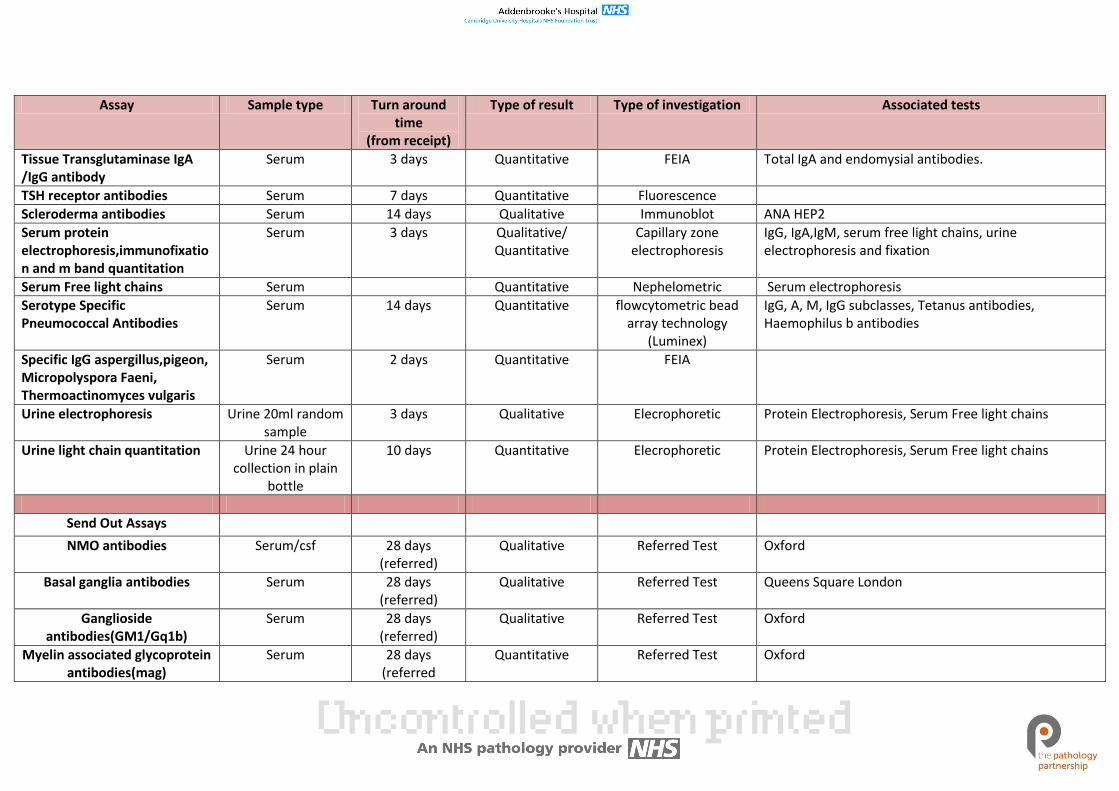
Assay Sample type Turn around time
(from receipt)
Type of result Type of investigation Associated tests
Tissue Transglutaminase IgA /IgG antibody
Serum 3 days Quantitative FEIA Total IgA and endomysial antibodies.
TSH receptor antibodies Serum 7 days Quantitative Fluorescence
Scleroderma antibodies Serum 14 days Qualitative Immunoblot ANA HEP2
Serum protein electrophoresis,immunofixation and m band quantitation
Serum 3 days Qualitative/ Quantitative
Capillary zone electrophoresis
IgG, IgA,IgM, serum free light chains, urine electrophoresis and fixation
Serum Free light chains Serum Quantitative Nephelometric Serum electrophoresis
Serotype Specific Pneumococcal Antibodies
Serum 14 days Quantitative flowcytometric bead array technology
(Luminex)
IgG, A, M, IgG subclasses, Tetanus antibodies, Haemophilus b antibodies
Specific IgG aspergillus,pigeon, Micropolyspora Faeni, Thermoactinomyces vulgaris
Serum 2 days Quantitative FEIA
Urine electrophoresis Urine 20ml random sample
3 days Qualitative Elecrophoretic Protein Electrophoresis, Serum Free light chains
Urine light chain quantitation Urine 24 hour collection in plain
bottle
10 days Quantitative Elecrophoretic Protein Electrophoresis, Serum Free light chains
Send Out Assays
NMO antibodies Serum/csf 28 days (referred)
Qualitative Referred Test Oxford
Basal ganglia antibodies Serum 28 days (referred)
Qualitative Referred Test Queens Square London
Ganglioside antibodies(GM1/Gq1b)
Serum 28 days (referred)
Qualitative Referred Test Oxford
Myelin associated glycoprotein antibodies(mag)
Serum 28 days (referred
Quantitative Referred Test Oxford
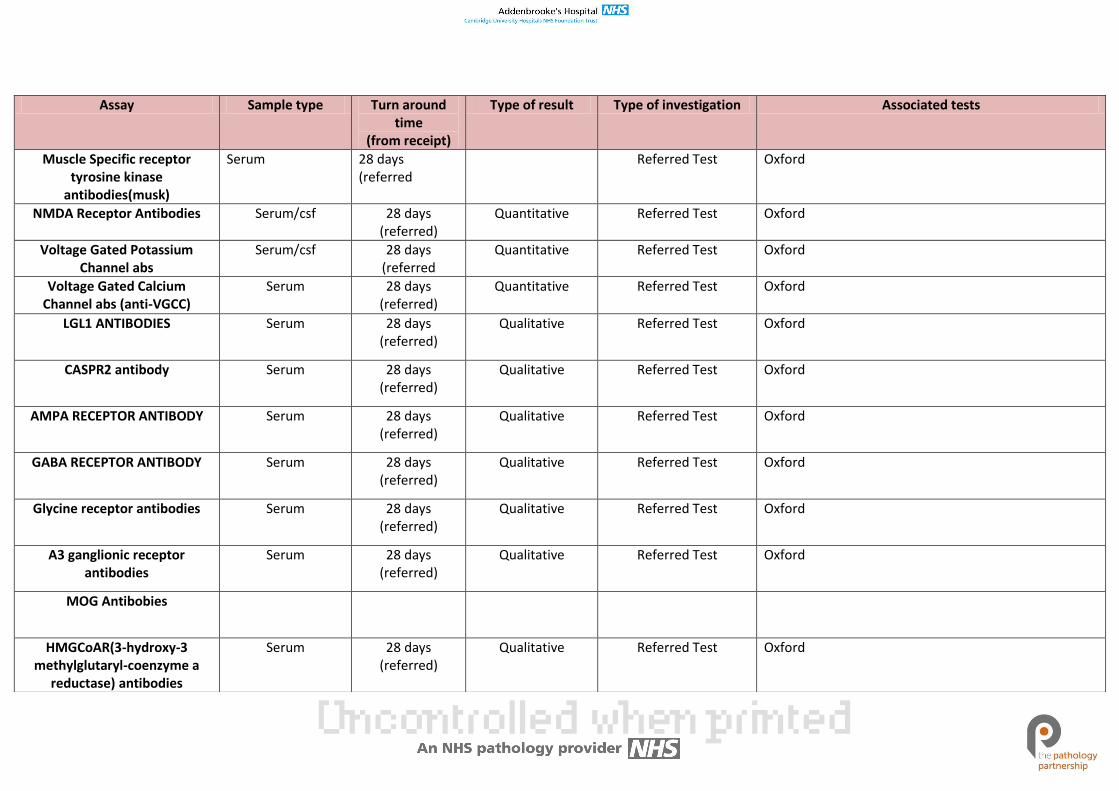
Assay Sample type Turn around time
(from receipt)
Type of result Type of investigation Associated tests
Muscle Specific receptor tyrosine kinase
antibodies(musk)
Serum 28 days (referred
Referred Test Oxford
NMDA Receptor Antibodies Serum/csf 28 days (referred)
Quantitative Referred Test Oxford
Voltage Gated Potassium Channel abs
Serum/csf 28 days (referred
Quantitative Referred Test Oxford
Voltage Gated Calcium Channel abs (anti-VGCC)
Serum 28 days (referred)
Quantitative Referred Test Oxford
LGL1 ANTIBODIES
Serum 28 days (referred)
Qualitative Referred Test Oxford
CASPR2 antibody Serum 28 days (referred)
Qualitative Referred Test Oxford
AMPA RECEPTOR ANTIBODY
Serum 28 days (referred)
Qualitative Referred Test Oxford
GABA RECEPTOR ANTIBODY Serum 28 days (referred)
Qualitative Referred Test Oxford
Glycine receptor antibodies Serum 28 days (referred)
Qualitative Referred Test Oxford
A3 ganglionic receptor antibodies
Serum 28 days (referred)
Qualitative Referred Test Oxford
MOG Antibobies
HMGCoAR(3-hydroxy-3 methylglutaryl-coenzyme a
reductase) antibodies
Serum 28 days (referred)
Qualitative Referred Test Oxford
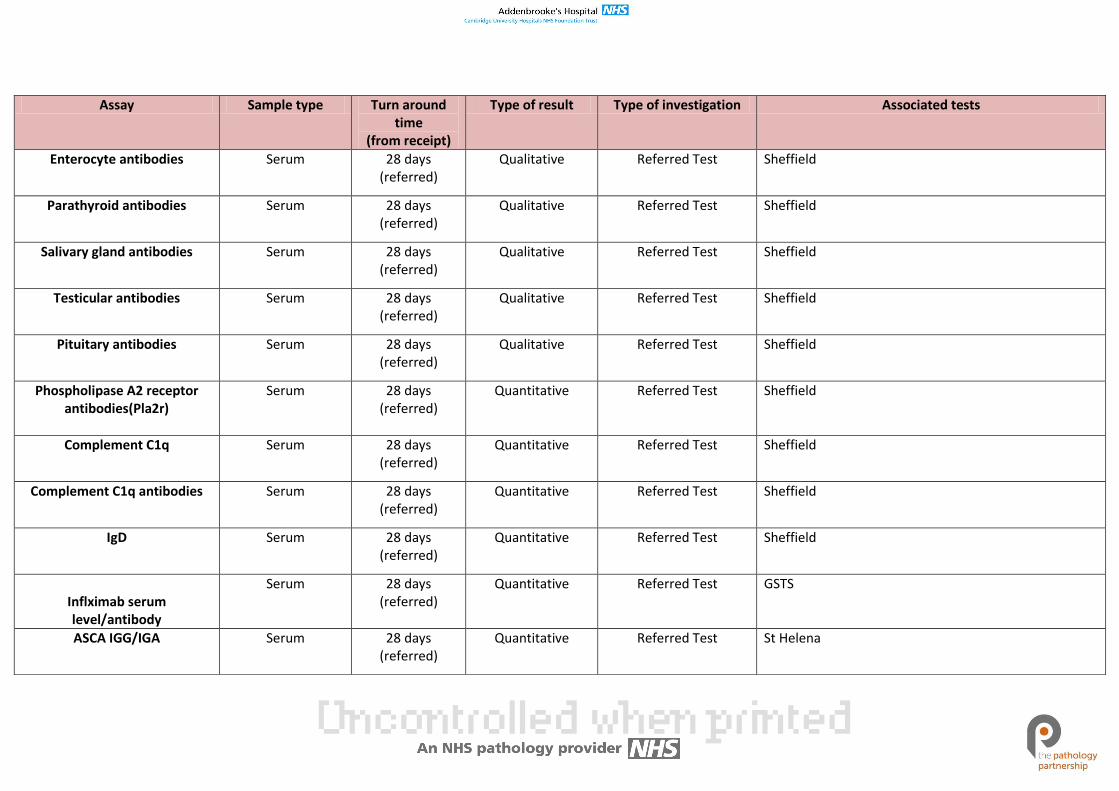
Assay Sample type Turn around time
(from receipt)
Type of result Type of investigation Associated tests
Enterocyte antibodies
Serum 28 days (referred)
Qualitative Referred Test Sheffield
Parathyroid antibodies
Serum 28 days (referred)
Qualitative Referred Test Sheffield
Salivary gland antibodies Serum 28 days (referred)
Qualitative Referred Test Sheffield
Testicular antibodies Serum 28 days (referred)
Qualitative Referred Test Sheffield
Pituitary antibodies Serum 28 days (referred)
Qualitative Referred Test Sheffield
Phospholipase A2 receptor antibodies(Pla2r)
Serum 28 days (referred)
Quantitative Referred Test Sheffield
Complement C1q
Serum 28 days (referred)
Quantitative Referred Test Sheffield
Complement C1q antibodies Serum 28 days (referred)
Quantitative Referred Test Sheffield
IgD
Serum 28 days (referred)
Quantitative Referred Test Sheffield
Inflximab serum level/antibody
Serum 28 days (referred)
Quantitative Referred Test GSTS
ASCA IGG/IGA
Serum 28 days (referred)
Quantitative Referred Test St Helena
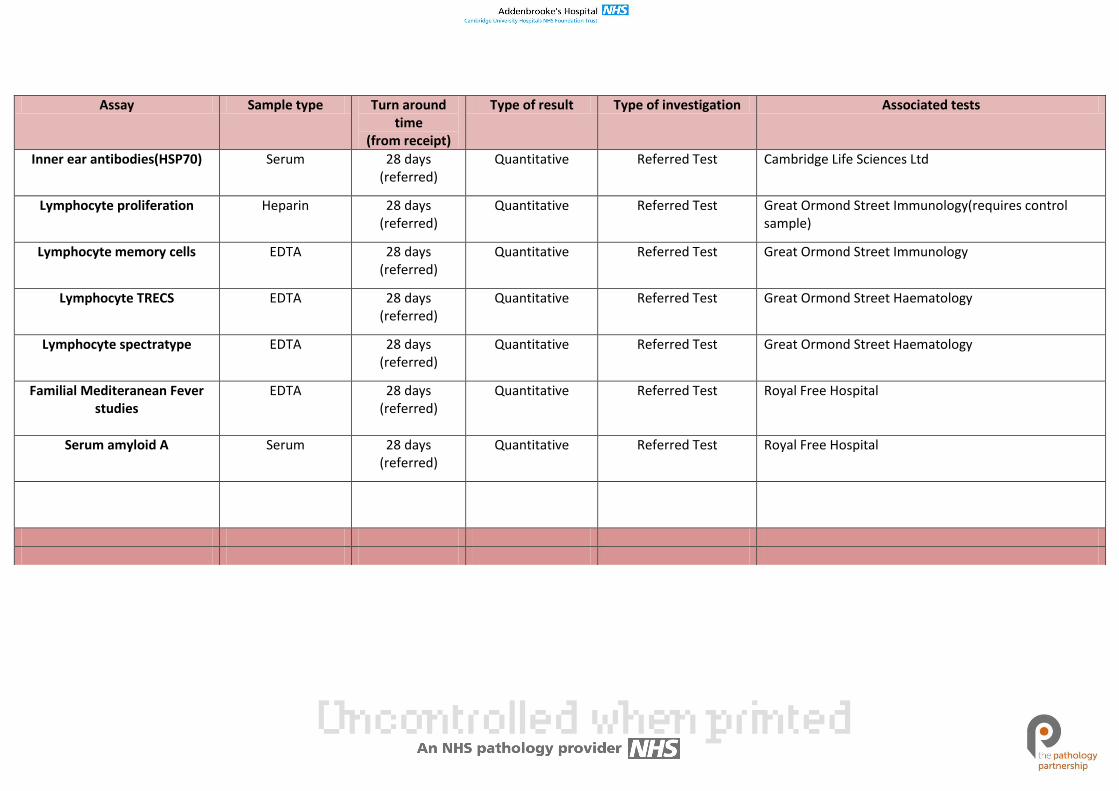
Assay Sample type Turn around time
(from receipt)
Type of result Type of investigation Associated tests
Inner ear antibodies(HSP70) Serum 28 days (referred)
Quantitative Referred Test Cambridge Life Sciences Ltd
Lymphocyte proliferation Heparin 28 days (referred)
Quantitative Referred Test Great Ormond Street Immunology(requires control sample)
Lymphocyte memory cells EDTA 28 days (referred)
Quantitative Referred Test Great Ormond Street Immunology
Lymphocyte TRECS EDTA 28 days (referred)
Quantitative Referred Test Great Ormond Street Haematology
Lymphocyte spectratype EDTA 28 days (referred)
Quantitative Referred Test Great Ormond Street Haematology
Familial Mediteranean Fever studies
EDTA 28 days (referred)
Quantitative Referred Test Royal Free Hospital
Serum amyloid A Serum 28 days (referred)
Quantitative Referred Test Royal Free Hospital
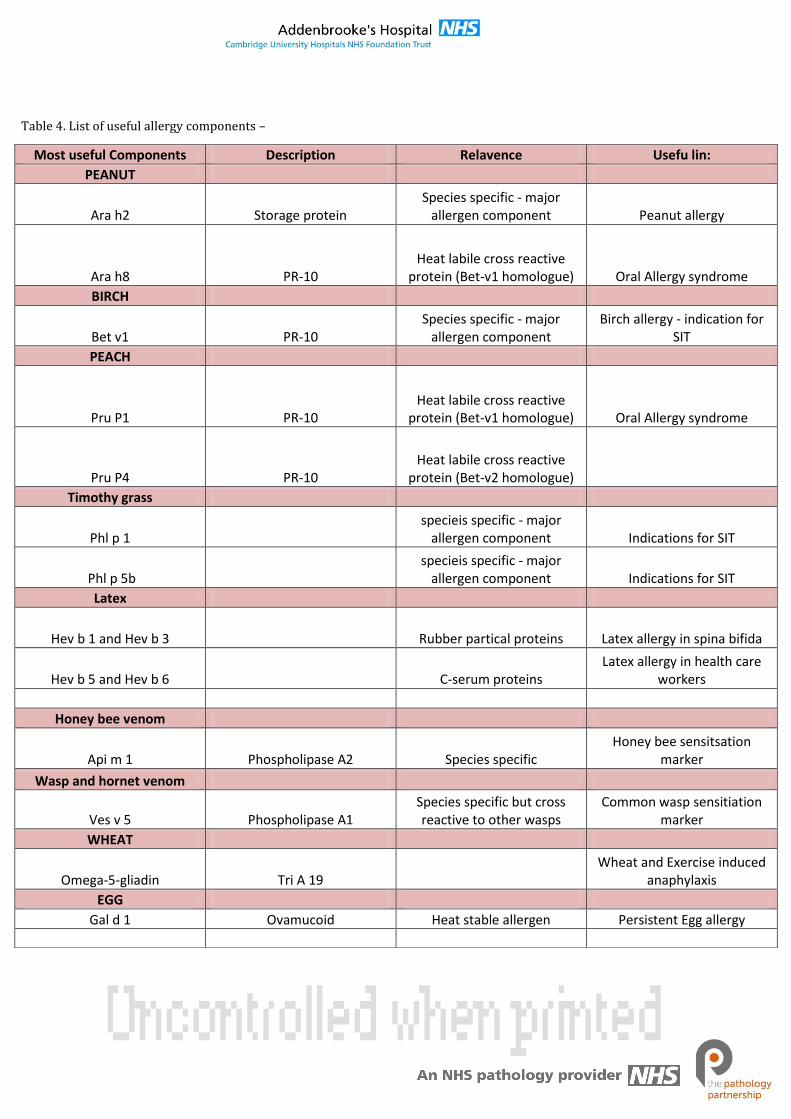
Most useful Components Description Relavence Usefu lin:
PEANUT
Ara h2 Storage protein Species specific - major
allergen component Peanut allergy
Ara h8 PR-10 Heat labile cross reactive
protein (Bet-v1 homologue) Oral Allergy syndrome
BIRCH
Bet v1 PR-10 Species specific - major
allergen component Birch allergy - indication for
SIT
PEACH
Pru P1 PR-10 Heat labile cross reactive
protein (Bet-v1 homologue) Oral Allergy syndrome
Pru P4 PR-10 Heat labile cross reactive
protein (Bet-v2 homologue)
Timothy grass
Phl p 1 specieis specific - major
allergen component Indications for SIT
Phl p 5b specieis specific - major
allergen component Indications for SIT
Latex
Hev b 1 and Hev b 3 Rubber partical proteins Latex allergy in spina bifida
Hev b 5 and Hev b 6 C-serum proteins Latex allergy in health care
workers
Honey bee venom
Api m 1 Phospholipase A2 Species specific Honey bee sensitsation
marker
Wasp and hornet venom
Ves v 5 Phospholipase A1 Species specific but cross reactive to other wasps
Common wasp sensitiation marker
WHEAT
Omega-5-gliadin Tri A 19 Wheat and Exercise induced
anaphylaxis
EGG
Gal d 1 Ovamucoid Heat stable allergen Persistent Egg allergy
Table 4. List of useful allergy components –
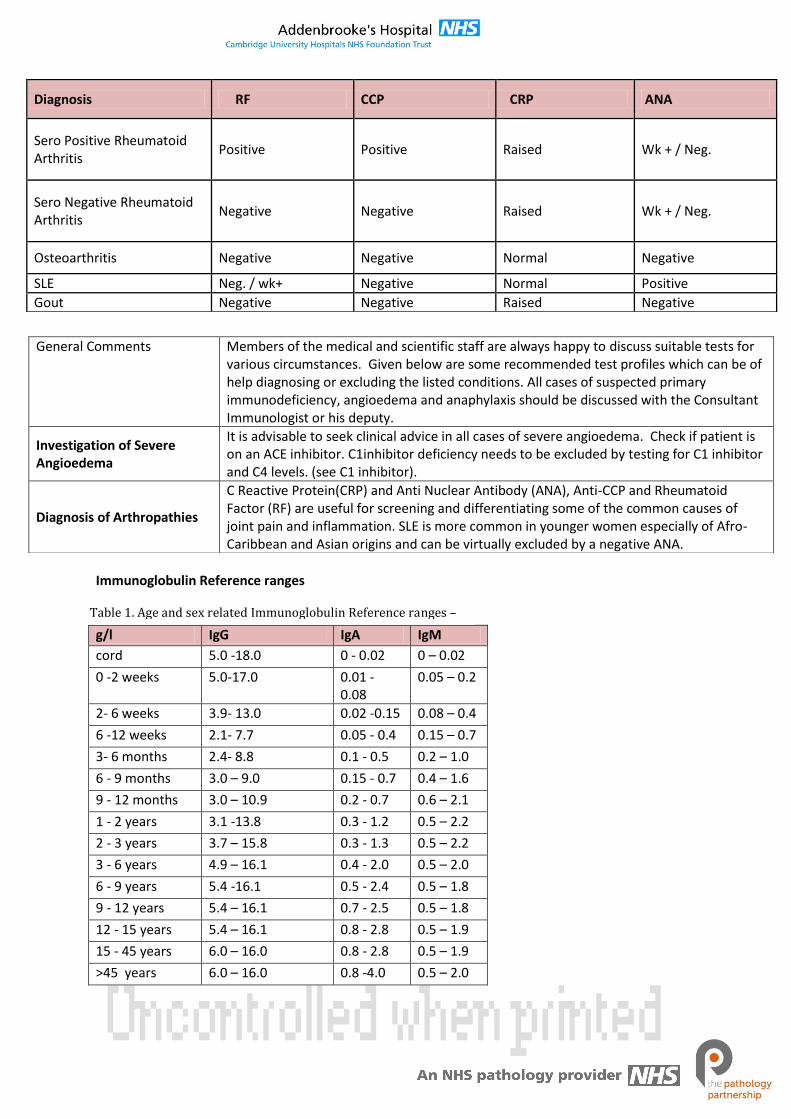
Immunoglobulin Reference ranges
g/l IgG IgA IgM
cord 5.0 -18.0 0 - 0.02 0 – 0.02
0 -2 weeks 5.0-17.0 0.01 - 0.08
0.05 – 0.2
2- 6 weeks 3.9- 13.0 0.02 -0.15 0.08 – 0.4
6 -12 weeks 2.1- 7.7 0.05 - 0.4 0.15 – 0.7
3- 6 months 2.4- 8.8 0.1 - 0.5 0.2 – 1.0
6 - 9 months 3.0 – 9.0 0.15 - 0.7 0.4 – 1.6
9 - 12 months 3.0 – 10.9 0.2 - 0.7 0.6 – 2.1
1 - 2 years 3.1 -13.8 0.3 - 1.2 0.5 – 2.2
2 - 3 years 3.7 – 15.8 0.3 - 1.3 0.5 – 2.2
3 - 6 years 4.9 – 16.1 0.4 - 2.0 0.5 – 2.0
6 - 9 years 5.4 -16.1 0.5 - 2.4 0.5 – 1.8
9 - 12 years 5.4 – 16.1 0.7 - 2.5 0.5 – 1.8
12 - 15 years 5.4 – 16.1 0.8 - 2.8 0.5 – 1.9
15 - 45 years 6.0 – 16.0 0.8 - 2.8 0.5 – 1.9
>45 years 6.0 – 16.0 0.8 -4.0 0.5 – 2.0
Diagnosis RF CCP CRP ANA
Sero Positive Rheumatoid Arthritis
Positive Positive Raised Wk + / Neg.
Sero Negative Rheumatoid Arthritis
Negative Negative Raised Wk + / Neg.
Osteoarthritis Negative Negative Normal Negative
SLE Neg. / wk+ Negative Normal Positive
Gout Negative Negative Raised Negative
General Comments Members of the medical and scientific staff are always happy to discuss suitable tests for various circumstances. Given below are some recommended test profiles which can be of help diagnosing or excluding the listed conditions. All cases of suspected primary immunodeficiency, angioedema and anaphylaxis should be discussed with the Consultant Immunologist or his deputy.
Investigation of Severe Angioedema
It is advisable to seek clinical advice in all cases of severe angioedema. Check if patient is on an ACE inhibitor. C1inhibitor deficiency needs to be excluded by testing for C1 inhibitor and C4 levels. (see C1 inhibitor).
Diagnosis of Arthropathies
C Reactive Protein(CRP) and Anti Nuclear Antibody (ANA), Anti-CCP and Rheumatoid Factor (RF) are useful for screening and differentiating some of the common causes of joint pain and inflammation. SLE is more common in younger women especially of Afro-Caribbean and Asian origins and can be virtually excluded by a negative ANA.
Table 1. Age and sex related Immunoglobulin Reference ranges –
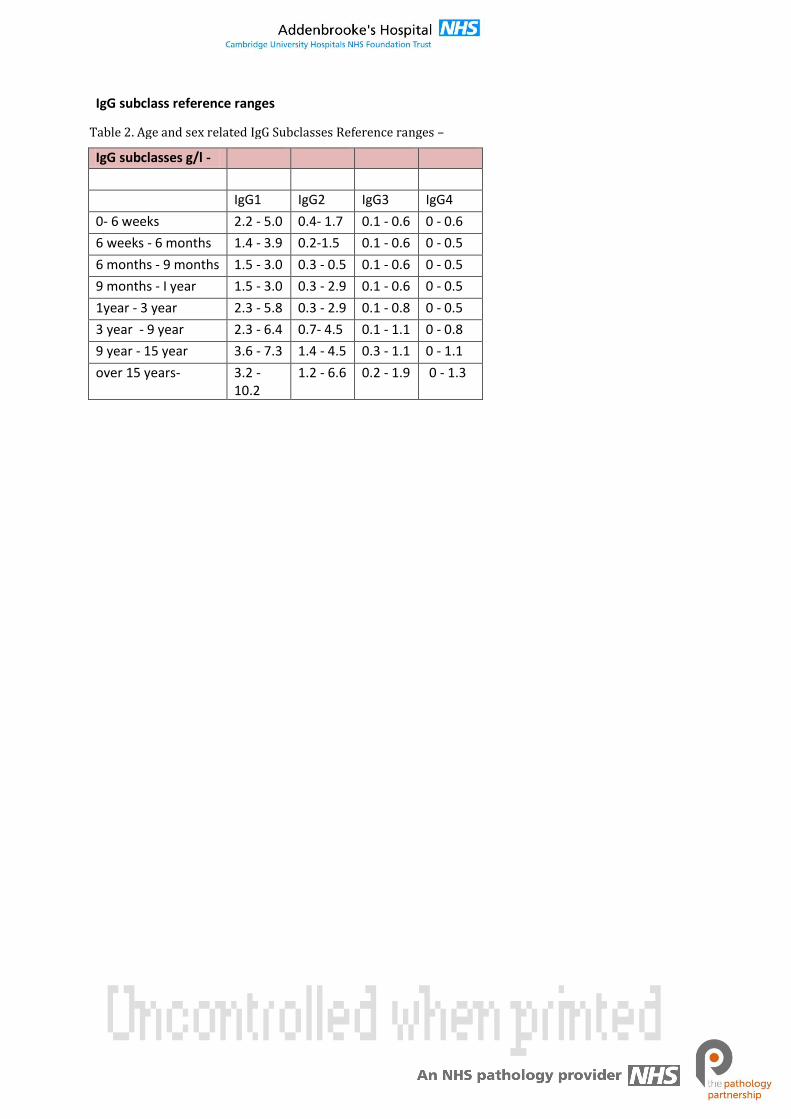
IgG subclass reference ranges
IgG subclasses g/l -
IgG1 IgG2 IgG3 IgG4
0- 6 weeks 2.2 - 5.0 0.4- 1.7 0.1 - 0.6 0 - 0.6
6 weeks - 6 months 1.4 - 3.9 0.2-1.5 0.1 - 0.6 0 - 0.5
6 months - 9 months 1.5 - 3.0 0.3 - 0.5 0.1 - 0.6 0 - 0.5
9 months - I year 1.5 - 3.0 0.3 - 2.9 0.1 - 0.6 0 - 0.5
1year - 3 year 2.3 - 5.8 0.3 - 2.9 0.1 - 0.8 0 - 0.5
3 year - 9 year 2.3 - 6.4 0.7- 4.5 0.1 - 1.1 0 - 0.8
9 year - 15 year 3.6 - 7.3 1.4 - 4.5 0.3 - 1.1 0 - 1.1
over 15 years- 3.2 - 10.2
1.2 - 6.6 0.2 - 1.9 0 - 1.3
Table 2. Age and sex related IgG Subclasses Reference ranges –
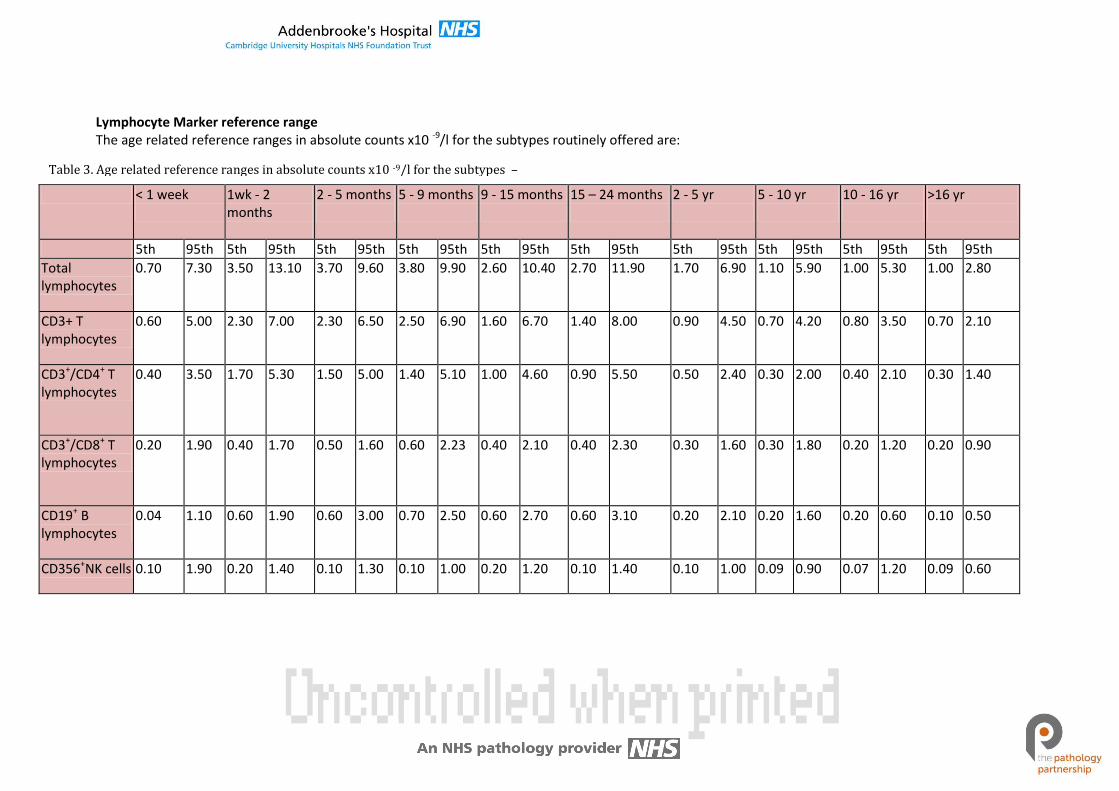
Lymphocyte Marker reference range The age related reference ranges in absolute counts x10 -9/l for the subtypes routinely offered are:
< 1 week
1wk - 2 months
2 - 5 months
5 - 9 months
9 - 15 months
15 – 24 months
2 - 5 yr
5 - 10 yr
10 - 16 yr
>16 yr
5th 95th 5th 95th 5th 95th 5th 95th 5th 95th 5th 95th 5th 95th 5th 95th 5th 95th 5th 95th
Total lymphocytes
0.70 7.30 3.50 13.10 3.70 9.60 3.80 9.90 2.60 10.40 2.70 11.90 1.70 6.90 1.10 5.90 1.00 5.30 1.00 2.80
CD3+ T lymphocytes
0.60 5.00 2.30 7.00 2.30 6.50 2.50 6.90 1.60 6.70 1.40 8.00 0.90 4.50 0.70 4.20 0.80 3.50 0.70 2.10
CD3+/CD4+ T lymphocytes
0.40 3.50 1.70 5.30 1.50 5.00 1.40 5.10 1.00 4.60 0.90 5.50 0.50 2.40 0.30 2.00 0.40 2.10 0.30 1.40
CD3+/CD8+ T lymphocytes
0.20 1.90 0.40 1.70 0.50 1.60 0.60 2.23 0.40 2.10 0.40 2.30 0.30 1.60 0.30 1.80 0.20 1.20 0.20 0.90
CD19+ B lymphocytes
0.04 1.10 0.60 1.90 0.60 3.00 0.70 2.50 0.60 2.70 0.60 3.10 0.20 2.10 0.20 1.60 0.20 0.60 0.10 0.50
CD356+NK cells 0.10 1.90 0.20 1.40 0.10 1.30 0.10 1.00 0.20 1.20 0.10 1.40 0.10 1.00 0.09 0.90 0.07 1.20 0.09 0.60
Table 3. Age related reference ranges in absolute counts x10 -9/l for the subtypes –
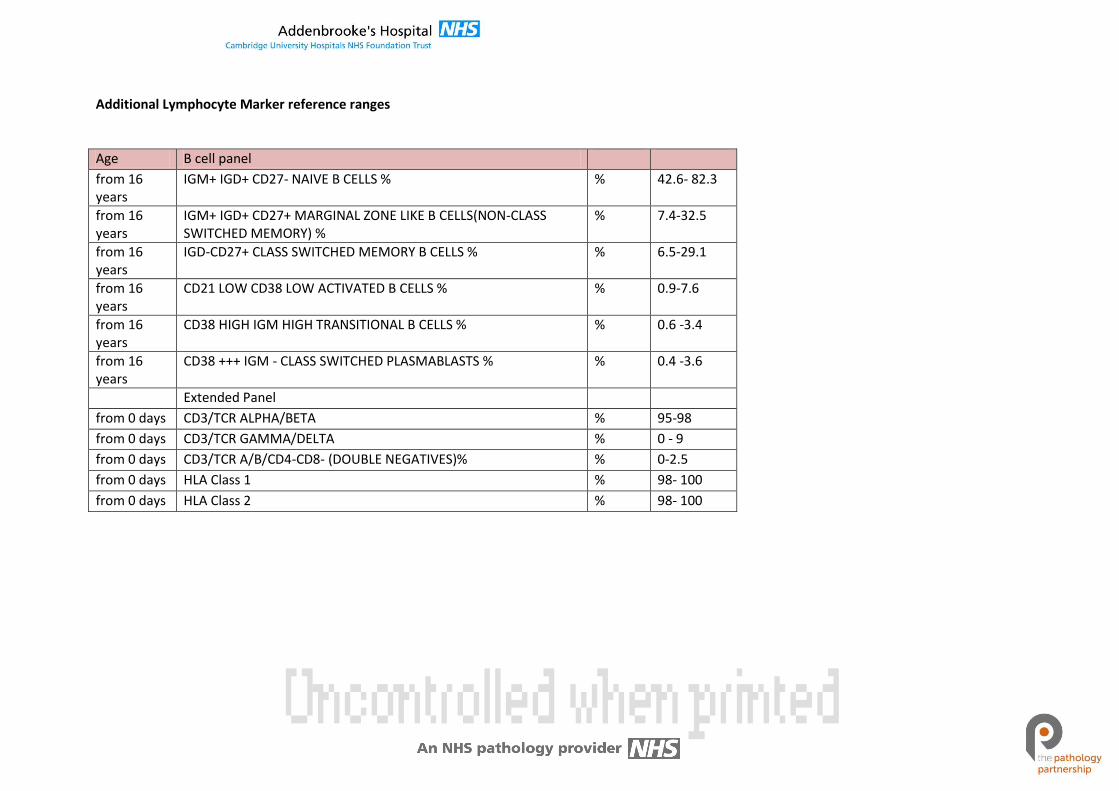
Additional Lymphocyte Marker reference ranges
Age B cell panel
from 16 years
IGM+ IGD+ CD27- NAIVE B CELLS % % 42.6- 82.3
from 16 years
IGM+ IGD+ CD27+ MARGINAL ZONE LIKE B CELLS(NON-CLASS SWITCHED MEMORY) %
% 7.4-32.5
from 16 years
IGD-CD27+ CLASS SWITCHED MEMORY B CELLS % % 6.5-29.1
from 16 years
CD21 LOW CD38 LOW ACTIVATED B CELLS % % 0.9-7.6
from 16 years
CD38 HIGH IGM HIGH TRANSITIONAL B CELLS % % 0.6 -3.4
from 16 years
CD38 +++ IGM - CLASS SWITCHED PLASMABLASTS % % 0.4 -3.6
Extended Panel
from 0 days CD3/TCR ALPHA/BETA % 95-98
from 0 days CD3/TCR GAMMA/DELTA % 0 - 9
from 0 days CD3/TCR A/B/CD4-CD8- (DOUBLE NEGATIVES)% % 0-2.5
from 0 days HLA Class 1 % 98- 100
from 0 days HLA Class 2 % 98- 100
Related Documents











