ABSTRACT Introduction: Oroantral fistulae are com- munications between the oral cavity and the maxillary sinus, primarily caused by tooth extractions. The majority of these communications close spontaneously due to their small size, but others form fistulae, perpetuating this pathological situation until proper treatment is pro- vided, causing both local and general pathology. Case report: We present the case of a 49- year-old male without previous medical history who was referred to the Oral Sur- gery Department at Hospital Virgen de La Paloma presenting with a three-week history of oroantral fistula with acute si- nusitis of the left maxillary sinus. After evaluation of the various therapeutic op- tions, Bichat’s buccal fat pad pedicle flap was performed along with a vestibular advancement flap, in a double-layer clo- sure technique. Conclusions: There are multiple tech- niques described in the literature for cor - recting this pathological entity, each with their own advantages and disadvantages. It is necessary to know the details of each of them in order to establish the ideal treatment for each situation. KEYWORDS Oroantral fistula; Oroantral communica- tion; Surgical treatment. Surgical treatment of oroantral post- extraction fistulas. Case presentation and review of the literature Clinical case García Moreno, Sergio Resident, Master in Oral Surgery and Implantology. Hospital Virgen de la Paloma. Private prac"ce. Leco Berrocal, Isabel Professor of Den"stry. Universi- dad Europea de Madrid (UEM). Professor of the Oral Surgery and Implantology Master’s Program. Hospital Virgen de la Paloma. Rubio-Alonso, Luis Associate Professor of Oral Sur- gery. School of Den"stry. Uni- versidad Complutense de Madrid (UCM). Professor of the Oral Surgery and Implantology Master’s Program. Hospital Vir- gen de la Paloma. Barona-Dorado, Cris"na Associate Professor of Oral Surgery. School of Dentistry. UCM. Deputy Director of the Oral Surgery and Implantology Master’s Program. Hospital Virgen de la Paloma. Mar #nez - González, José María Tenured Professor of Oral and Maxillofacial Surgery. School of Den"stry. UCM. Director of the Oral Surgery and Implantology Master’s Program. Hospital Vir- gen de la Paloma. 16 Correspondence address: Sergio García Moreno C/ Lagasca 13 3º dcha 28001 Madrid [email protected] Phone no: 649 985 148 Received: 1 June 2015. Accepted (or accepted for publication): 30 September 2015. Indexed in: - IME - IBECS - LATINDEX - GOOGLE SCHOLAR Published in Spanish Científica Dental Vol. 12. Nº 3. 2015 www.cientificadental.es Volver científica dental. vol 13 (special supplement) 2016. científica dental. vol 13 (special supplement) 2016.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ABSTRACTIntroduction: Oroantral fistulae are com-munications between the oral cavity andthe maxillary sinus, primarily caused bytooth extractions. The majority of thesecommunications close spontaneouslydue to their small size, but others formfistulae, perpetuating this pathologicalsituation until proper treatment is pro-vided, causing both local and generalpathology.
Case report: We present the case of a 49-year-old male without previous medicalhistory who was referred to the Oral Sur-gery Department at Hospital Virgen de LaPaloma presenting with a three-weekhistory of oroantral fistula with acute si-nusitis of the left maxillary sinus. Afterevaluation of the various therapeutic op-tions, Bichat’s buccal fat pad pedicle flapwas performed along with a vestibularadvancement flap, in a double-layer clo-sure technique.
Conclusions: There are multiple tech-niques described in the literature for cor-recting this pathological entity, each withtheir own advantages and disadvantages.It is necessary to know the details of eachof them in order to establish the idealtreatment for each situation.
KEYWORDSOroantral fistula; Oroantral communica-tion; Surgical treatment.
Surgical treatment of oroantral post-extraction fistulas.Case presentation and review of theliterature
Clinical case
García Moreno, SergioResident, Master in Oral Surgeryand Implantology. Hospital Virgende la Paloma. Private prac"ce.
Leco Berrocal, IsabelProfessor of Den"stry. Universi-dad Europea de Madrid (UEM).Professor of the Oral Surgery andImplantology Master’s Program.Hospital Virgen de la Paloma.
Rubio-Alonso, LuisAssociate Professor of Oral Sur-gery. School of Den"stry. Uni-versidad Complutense deMadrid (UCM). Professor of theOral Surgery and ImplantologyMaster’s Program. Hospital Vir-gen de la Paloma.
Barona-Dorado, Cris"naAssociate Professor of OralSurgery. School of Dentistry.UCM. Deputy Director of theOral Surgery and ImplantologyMaster’s Program. HospitalVirgen de la Paloma.
Mar#nez-González, José MaríaTenured Professor of Oral andMaxillofacial Surgery. School ofDen"stry. UCM. Director of theOral Surgery and ImplantologyMaster’s Program. Hospital Vir-gen de la Paloma.
16
Correspondence address:Sergio García Moreno
C/ Lagasca 13 3º dcha28001 [email protected] no: 649 985 148
Received: 1 June 2015.Accepted (or accepted for publication): 30 September 2015.
Indexed in:- IME- IBECS- LATINDEX- GOOGLE SCHOLAR
Published in Spanish Científica Dental Vol. 12. Nº 3. 2015www.cientificadental.es
Volver
científica dental. vol 13 (special supplement) 2016.científica dental. vol 13 (special supplement) 2016.
17
INTRODUCTION An oroantral communication (OAC) is a pathologicalcondition characterized by the presence of a continuitybetween the oral cavity and the maxillary sinus thataffects both the sinus, the oral mucosae and the max-illary bone between them. The most common causeof OAC is simple or surgical tooth extraction of antralteeth; Franco et al.1 state that this is the cause in92.63% of cases of OAC. It can also be found in the fieldof implantology, either immediately at the time of sur-gery, or following the placement of implants. Otherless frequent etiologies include the presence of cystsor tumors in the maxillary sinus (4.47%), trauma(1.3%), peridontal infections (0.93%), radiation to thehead and neck, syphilis, tuberculosis and bisphospho-nate-induced osteonecrosis2-6.
The clinical presentation of OAC is highly variable. Itcan be asymptomatic or present notable signs andsymptoms such as functional changes in swallowing,respiration or phonation, pain around the cheek, in-fraorbital area and tissues surrounding the OAC, supu-ration from the communication itself or the ipsilateralnasal fossa, swelling of the area, generalized malaiseor fever.
Treatment of this pathology is primarily surgical, withmultiple techniques described for this purpose. Themost commonly used techniques are trapezoidalvestibular advancement flap (TVAF), rotational palatalflap (RPF) and Bichat’s buccal fat pad (BBFP).
TVAF is usually performed in small OACs since there isa risk of recurrence in larger communications. RPF is afull-thickness mucoperiostic flap of the palatine fibro-mucosa that is rotated to cover the area of the OACdefect, leaving an exposed area of bone that heals sec-ondarily in a period of 3-4 weeks. Bichat’s buccal fatpad (BBFP) consists of traction of the flap through a0.5 to 3 cm horizontal incision in the periosteum at thelevel of the zygomatic arch, suturing it to the palatinemucosa and replacing the vestibular flap over it; theexposed fat tissue will epithelialize within approxi-mately 3 weeks; this flap provides a large amount of
vitalized tissue that is highly vascularized by the max-illary, superficial temporal and facial arteries, which al-lows to close large OACs with a low percentage ofcomplications and a high rate of success.
CASE REPORTWe present the case of a 49-year-old male withoutprevious medical history who was referred by his den-tist to the Oral Surgery Department at Hospital Virgende La Paloma in Madrid. The patient presented withswelling and intense pain in the cheek with suppura-tion in the oral cavity and left nasal fossa three weeksafter having undergone extractions in the left posteriormaxillary sector. In addition to local symptoms, the pa-tient referred malaise and high fever.
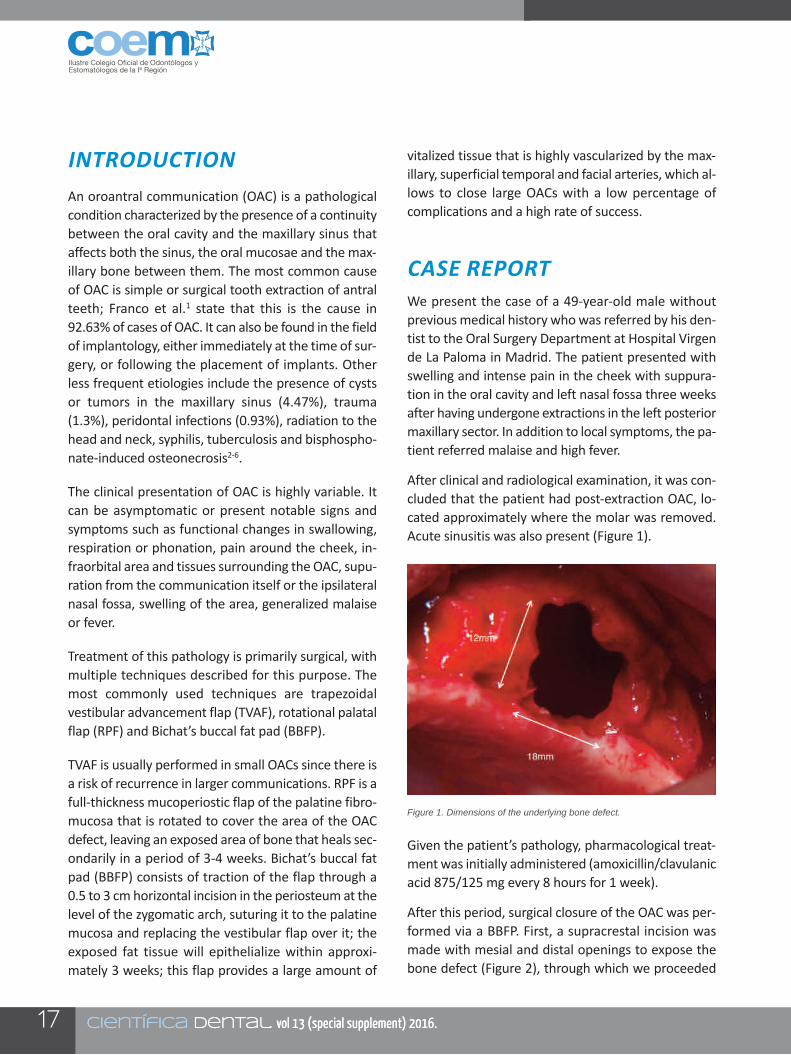
After clinical and radiological examination, it was con-cluded that the patient had post-extraction OAC, lo-cated approximately where the molar was removed.Acute sinusitis was also present (Figure 1).
Given the patient’s pathology, pharmacological treat-ment was initially administered (amoxicillin/clavulanicacid 875/125 mg every 8 hours for 1 week).
After this period, surgical closure of the OAC was per-formed via a BBFP. First, a supracrestal incision wasmade with mesial and distal openings to expose thebone defect (Figure 2), through which we proceeded
científica dental. vol 13 (special supplement) 2016.científica dental. vol 13 (special supplement) 2016.
Figure 1. Dimensions of the underlying bone defect.

18
to clean the sinus using 0.12% chlorhexidine lavagesand careful curettage. Once clean, a horizontal inci-sion was made in the periosteum at the level of thevestibular fundus of the second and third molar inorder to access Bichat’s buccal fat pad. Once exposed,it is dissected and progressively pulled until the entirebone defect is covered with no tension on the flap(Figure 3) and the palatine mucosa is sutured. In thiscase, given the large bone defect, the adipose tissuewas covered with a TVAF in order to provide more sta-bility and to avoid possible complications derived fromscarring of the adipose tissue that was directly ex-posed in the oral cavity.
The patient was followed and evaluated at days 3rd,7th, at the 3rd and 6th weeks (Figure 4) and at one year(Figure 5) postoperatively. No complications occurredand complete resolution of the sinus pathology andthe oroantral fistula was achieved.
DISCUSSIONThere are multiple surgical techniques and protocolsfor the treatment of OAC with no clearly establishedand unanimously accepted action criteria.
The majority of authors state that small OACs closespontaneously without the need for surgical treatmentwithin a period of 2 days to 2 weeks in the absence of
científica dental. vol 13 (special supplement) 2016.científica dental. vol 13 (special supplement) 2016.
Figure 2. Traction of the Bichat’s pad of fat. Figure 5. Appearance at one year.
Figure 3. Suturing of the surgical wound.
Figure 4. Appearance at 6 weeks.

19
sinus pathology7. Some authors claim that the maxi-mum width for spontaneous closure be 2 mm7,8 or upto 5 mm as referred by others9,10.
Prior to surgical closure of the communication, evalu-ation of the state of the maxillary sinuses is required;if they are involved or there was sinus pathology priorto tooth extraction, intraoral treatment of the sinusesusing a Cadwell-Luc approach or endoscopic treatmentvia the nasal fossae would be required7,11.
There is a high level of variability on the usage criteria,limitations, complications, etc. among the most com-monly used techniques.
According to most authors, TVAF is the techniquepresenting the fewest postoperative complications,but it has the greatest risk of recurrence of theoroantral fistula. Some authors found recurrence onlyin patients treated with TVAF but not with other tech-niques7,9. However, Franco et al.1 reported a failurerate of 10.39%, which is even lower than RPF, with afailure rate of 11.68%, although this is due to the factthat their meta-analysis included authors who usedRPF to treat OACs caused by extraction of superiorthird molars, a technique not indicated for this typeof defect unless the anterior palatine orifice is ex-tended12. Batra et al.7 consider this technique to becontraindicated when there are large bone defects,sinus involvement, reinterventions or when the OACis very posterior or very palatinized, given that inthese cases, the tension on the flap is much greater,which increases the risk of failure. They also considerit contraindicated when the patient is going to receiverehabilitation with any type of removeable prosthesisdue to the decrease in the width of permanentvestibular fundus that is present in 40% of patients7,9.TVAF has also been used as a complement to theBBFP technique, as in the case presented, in order toprovide greater safety to the intervention and toavoid the risk of healing-related complications asso-ciated to this technique such as herniation of the flap,partial necrosis and in particular excessive granula-tion tissue formation during healing1; however, otherauthors state that it does not provide any significant
advantage over the conventional BBFP technique andonly recommend its use when the Bichat’s pad hasbeen perforated or excessively stretched under trac-tion, a situation that can be solved with the use oflyophilized porcine dermal membranes, without los-ing vestibular depth5,7.
Another possible combination described in the TVAFliterature is using small-sized RPF that, although itslightly decreases the possible tension on the suture,it adds some loss of the vestibular fundus that resultsfrom TVAF to the morbidity of RPF.
RPF has been used to close both small and very ex-tensive OAC. It has been reported to successfullyclose a 2 x 4 cm OAC8. The main disadvantage of thistechnique reported by the majority of authors is post-operative complications and the high number of com-plications that can occur (persistence of the passageof air and liquids between the nose and oral cavitybelow the flap until healing has concluded, flapnecrosis, postoperative bleeding, excessive granula-tion of the scar, etc.)1,7. Batra et al.7 state that the re-maining techniques available are less aggressive andequally successful. Therefore, they recommendavoiding its use except in very specific situations, al-though other authors claim these problems are min-imal and they indicate its use for closure of large orlong-duration OACs prior to TVAF and BBFP8,13,14.However, all authors concur in that OACs in a veryposterior or very vestibularized location are besttreated with a technique other than RPF.
The majority of authors consider BBFP to have thelowest risk of recurrence. Franco et al.1 report a1.30%, much lower other techniques. According tothe literature, the use of this technique is indicatedin defects up to 7 x 5 cm, but the majority of authorsrecommend limiting this technique to defects smallerthan 5 x 4 cm15. The reasons for the high success rateof this technique appear to be related to the largemass of vitalized tissue that is highly vascularized bythe maxillary, facial and superficial temporal arteries.This promotes rapid epithelialization once exposedto the oral cavity within 3-4 weeks15. In addition to
científica dental. vol 13 (special supplement) 2016.científica dental. vol 13 (special supplement) 2016.

20
the high level of success, BBFP is increasingly becom-ing the technique of choice for post-extraction OACsdue to its ease of extraction with minimal dissection,the low rate of complications, low morbidity in thedonor zone and because this technique can be per-formed under local anesthesia in the dental office.Although less frequent than RPF, BBFP is also not ex-empt from complications, some of which are moresignificant than those produced by other techniques.These include partial necrosis of the flap, fibrosis,trismus, marked inflammation, excessive formationof granulation tissue and complications derived fromdeficient surgical technique such as hemorrhage anddamage to the facial nerve8,9.
This technique was used in the case presented inorder to achieve maximum predictability in the clo-sure of such a large OAC. RPF was discarded despitea larger vestibular fundus being preferable in light offuture prosthetic rehabilitation because it was not asound reason because of the complications thatcould arise, such as a worse surgical field for cleaningthe sinus or greater postoperative damage, in a pa-tient who had just had all of the maxillary teeth ex-tracted. Although the patient initially lost length ofthe vestibular fundus, he recovered the original di-mensions over time, with complete symmetry at theone-year follow-up visit.
There are also other techniques based on mobiliza-tion of the soft tissues such as the lingual flap, thebuccal mucosal flap from the genial region or thetemporal muscle flap. These are currently used muchless frequently due to their high morbidity, and prac-tically abandoned for closure of post-extractionOAC7.
We can also find techniques that are not only basedon mobilization of soft tissues for closure of OACsuch as the use of alloplastic materials including goldor polymethacrylate sheets, but these can result incomplications such as extrusion, migration or infec-tion16; or autologous transplant and subsequent en-dodontics of the third superior molar to the bedwhere the defect is located17.
In patients needing prosthetic rehabilitation with theuse of osseointegrated implants, closure of the OACby surgical techniques that only involve mobilizationof different soft tissues, the sinus mucosa and theoral mucosa will be in contact without a barrier be-tween them, which significantly difficults future sur-gery to elevate the sinus for the placement ofimplants. In order to avoid this problem, en blockbone grafts from different donor areas can be used,whether they are intra-oral or extra-oral18-21, or au-tologous cartilage implants, be they auricular orfrom the nasal septum; these types of grafts havethe advantage of being more resistant to infectionthan osseous tissue and they do not require vascu-larization for integration, which considerably reducesthe risk of failure in addition to lower morbidity ofthe donor zone22. Within this field, there are also au-thors who propose the use of bone morphogenicprotein 2 (BMP2), claiming that there is a lower riskof infection compared to conventional bone grafts,when the previous chronic infection of the targetarea is eliminated23.
CONCLUSIONSThere is no single solution for the treatment of thispathology, nor are there unanimous criteria on whenone technique or another is indicated. For this reason,it is very important to understand the limitations anddisadvantages of each technique and to integrate as-pects such as location, time of disease progression,size of the OAC and type of prosthetic rehabilitationthat the patient will use in the future. The therapeuticapproach that best suits the individual patient’s situ-ation should be chosen.
científica dental. vol 13 (special supplement) 2016.científica dental. vol 13 (special supplement) 2016.

21 científica dental. vol 13 (special supplement) 2016.científica dental. vol 13 (special supplement) 2016.
1. Franco-Carro B, Barona-DoradoC, Martínez-González MJ, Rubio-Alonso LJ, Martínez-González JM.Meta-analytic study on the fre-quency and treatment of oral an-tral communications. Med Oral Pa-tol Oral Cir Bucal 2011; 16: 682-7.
2. Arias-Irimia O, Barona-Dorado C,Santos-Marino JA, Marti nez-Ro-dríguez N, Martinez-Gonzalez JM.Meta-analsis of the etiology ofodontogenic maxillary sinusitis.Med Oral Patol Oral Cir Bucal2010; 15: 70-3.
3. González-García A, González-García J, Diniz-Freitas M, García-García A, Bullón P. Accidental dis-placement and migration ofendosseous implants into adjacentcraniofacial structures: A reviewand update. Med Oral Pato Cir Bu-cal 2012; 17: e769-74.
4. Del Rey-Santamaría M, Valma-seda Castellón E, Berini Aytés L,Gay Escoda C. Incidence of oralsinus communications in 389 up-per third molar extraction. MedOral Patol Oral Cir Bucal 2006; 11:334-8.
5. Jain M, Ramesh C, Sankar K, Lo-kesh K. Pedicled buccal fat pad inthe management of oroantral fis-tula: a clinical study of 15 cases.Int J Oral Maxillofac Surg 2012;41: 1025-9.
6. Mast G, Otto S, Mücke T, SchreyerC, Bissinger O, Kolk A, et all. Inci-dence of maxillary sinusitis andoro-antral fistulae in bisphospho-nate-related osteonecrosis of thejaw. J Craneo-Maxillofac Surg2012; 40: 568-71.
7. Batra H, Jindal G, Kaur S. Eva-luation of different treatment mo-dalities for closure of oro-antralcommunications and formulationof a rational approach. J MaxillofacOral Surg 2010; 9: 13-8.
8. Anavi Y, Gal G, Silfen R, CalderonS. Palatal rotation-advancementflap for delayed repair of oroantralfistula: A retrospective evaluationof 63 cases. Oral Surg Oral MedOral Pathol Oral Radiol Endod2003; 96: 527-34.
9. Nezafati S, Vafaii A, GhojazadehM. Comparison of pedicled buccalfat pad flap with buccal flap for clo-sure of oro-antral communication.Int J Oral Maxillofac Surg 2012;4: 624-8.
10. Aparicio A. Colgajos locales y pe-diculados en el manejo de las co-municaciones y fístulas oroantra-les. Rev Med 2011; 19: 217-25.
11. Giovannetti F, Priore P, Raponi I,Valentini V. Endoscopic Sinus Sur-gery in Sinus-Oral Pathology. Cra-niofac Surg 2014; 25: 991-4.
12. Vericat Queralt A, Berini Aytés L,Gay Escoda C. Tratamiento qui-rúrgico de las comunicaciones bu-cosinusales. Rev Vasca Odonto-estomatol 2000; 2: 10-23.
13. Hori M, Tanaka H, Matsumoto M,Matsunaga S. Application of theinterseptal alveolotomy for closingthe oroantral fistula. J Oral Maxi-llofac Surg 1995; 53: 1392-6.
14. Herbert DC. Closure of a palatalfistula using mucoperiosteal islandflap. Br J Plast Surg 1974; 27:332-6.
15. Singh J, Prasad K, Lalitha RM,Ranganath K. Buccal pad of fatand its applications in oral and ma-xillofacial surgery: a review of pu-blished literature (February) 2004to (July) 2009. Oral Surg Oral MedOral Pathol Oral Radiol Endod2010; 110: 698-705.
16. Kansu L, Akman H, Uckan S. Clo-sure of oroantral fistula with theseptal cartilage graft. Eur Arch Otor-hinolaryngol 2010; 267: 1805-6.
17. Kitagawa Y, Sano K, Nakamura
M, Ogasawara T. Use of third mo-lar transplantation for closure ofthe oroantral communication aftertooth extraction: a report of 2 ca-ses. Oral Surg Oral Med Oral Pa-thol Oral Radiol Endod 2003; 95:409-15.
18. Peñarrocha-Diago M, García B,Gomez D, Balaguer J. Zygomaticbone graft for oral- antral commu-nication closure and implant pla-cement. J Oral Implantol 2007; 33:305-9.
19. Mohamadi M, Samieirad S, Bani-mostafaee H, Sadeghi HM. Clo-sure of large oroantral communi-cation using coronoid processpedicled on temporalis muscleflap: a new alternative approach.J Craniofac Surg 2013; 24: 1399-402.
20. Watzak G, Tepper G, Zechner W,Monov G, Busenlechner D, Wat-zek G. Bony press-fit closure oforo-antral fistulas: a technique forpre-sinus lift repair and secondaryclosure. J Oral Maxillofac Surg2005; 63: 1288-94.
21. Er N, Tuncer HY, Karaca C, Co-purog lu S. Treatment of oroantralfistulas using bony press-fit tech-nique. J Oral Maxillofac Surg2013; 71: 659-66.
22. Isler SC, Demircan S, Cansiz E.Closure of oroantral fistula usingauricular cartilage: a new methodto repair an oroantral fistula. Br JOral Maxillofac Surg 2011; 49:86-7.
23. Cottam JR, Jensen OT, Beatty L,Ringeman J. Closure of 1.5-cm al-veolar oral antral fistula with intra-alveolar sinus membrane eleva-tion and bone morphogeneticprotein-2/ collagen graft followedby dental implant restoration: casereport. Int J Oral Maxillofac Im-plants 2013; 28: 277-82.
BIBLIOGRAPHY
Related Documents