
Chapter 6 Revenue Determination 5–3 Learning Objectives Define basic methods of payment for health care firms Understand the general factors that influence.
Dec 27, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Chapter 6
Revenue Determination
•5–3
Learning Objectives• Define basic methods of payment for health care
firms
• Understand the general factors that influence pricing
• Define the basic health care pricing formula
• Determine if prices are defensible
• List some of the important considerations when negotiating a managed-care contract
2
Alternative Payment Systems
• Payment systems can be categorized by 2 dimensions– Payment Basis– Unit of Payment
•5–4
3
Payment Basis
• The basis of payment defines how the actual payment will be made. There are 3 primary methods-
1. Cost
2. Fee Schedules
– e.g. DRG’s
3. Price Related
– e.g. 75% of billed charges
•5–5
4

Unit of Payment
• Unit of payment defines how the services provided are consolidated into an actual claim. There are 2 primary methods-
1. Specific Services
– Individual items that are listed in a claim are paid
2. Bundled Services
– Specific services listed in a claim are paid on some aggregated basis – such as a DRG or per diem
•5–6
5
•5–7
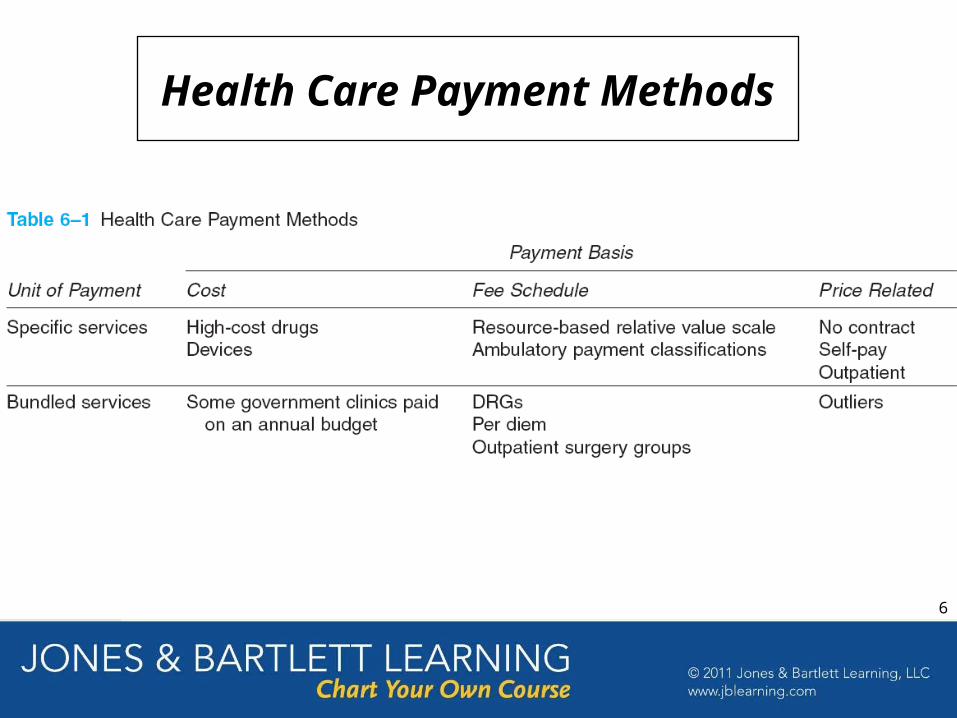
Health Care Payment Methods
6
Factors Influencing Pricing
• Pricing includes the establishment of CDM prices and the negotiation of managed care contracts
• Three factors drive pricing policies– Required net income– Competitive position– Market structure
•5–8
7
•5–9
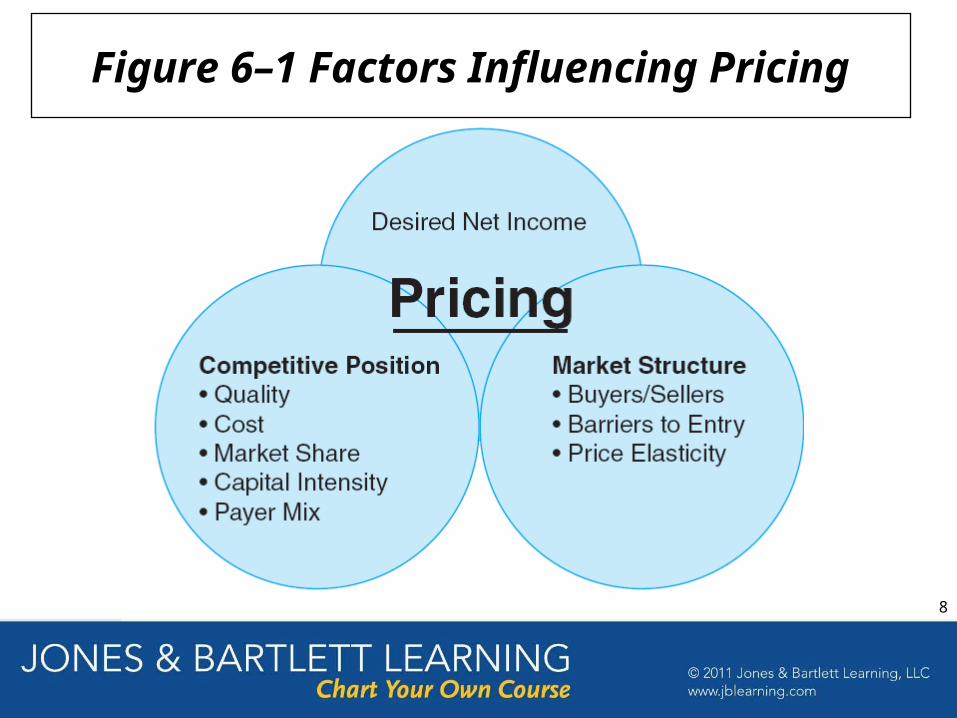
Figure 6–1 Factors Influencing Pricing
8
Setting Actual CDM Prices
• There are 4 factors that must be “mathematically” reflected in prices
• Failure to incorporate these 4 factors will impact financial survival.
•5–10
9
•5–11
Four Elements of Pricing
10
•Average costsLosses on third-party fee-schedule payments
MedicaidMedicareOther
Write-offs on billed-charge patientsSelf payCommercial
Reasonable return on investmentSustainable growth
•5–12
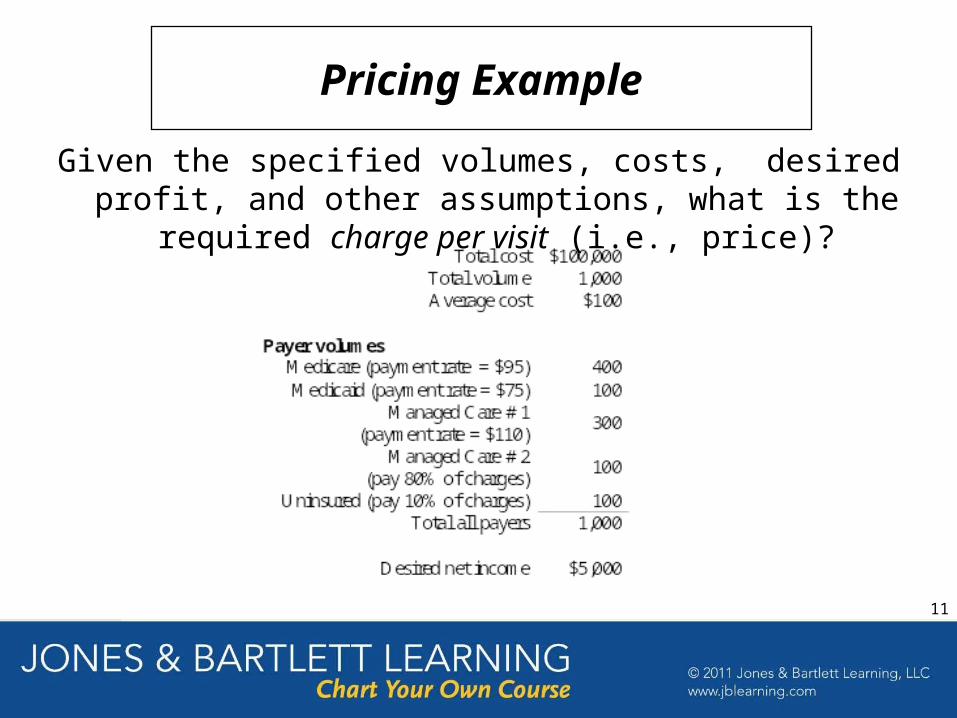
Pricing Example
Given the specified volumes, costs, desired profit, and other assumptions, what is the required charge per visit (i.e., price)?
11
•5–13
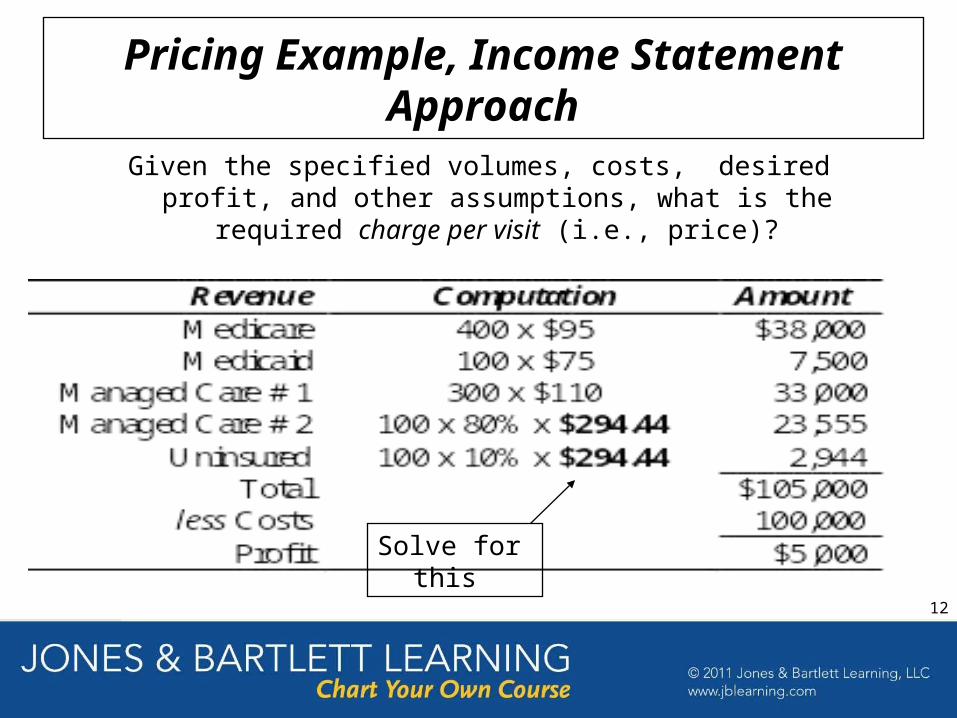
Pricing Example, Income Statement Approach
Given the specified volumes, costs, desired profit, and other assumptions, what is the required charge per visit (i.e., price)?
Solve for this
12

•5–14
Pricing Formula
General Pricing Formula
Pricing Formula Applied to Example
13
•5–15
1. Increase in costs
2. Governmental programs that pay less than cost
3. Managed-care plan fee schedules that do not pay at levels above cost
4. Increases in required profit, such as debt-service obligations or capital replacement
5. Reductions in charge-paying patients
6. Increases in uninsured patients
Factors That Tend to Increase Prices
14
Assessing Reasonableness of Prices
• Many healthcare providers, especially hospitals, have been criticized for unreasonable prices.
• One web site http://www.hospitalvictims.com compares prices based on markups for all hospitals in US. A Maryland hospital (Johns Hopkins) is selected because Medicare + Medicaid pay close to 100% of charges which keeps Maryland hospital prices very low.
•5–16
15
•5–17
1. Return-on-Investment (ROI) adequacy
2. Comparison with other health care firms
Reasonableness of Charges
Two Generic Ways of Assessing:
16

•5–18
Is ROI at Case Hospital reasonable?
Are costs at Case Hospital reasonable?
Is investment at Case Hospital reasonable?
ROI Method, Case Hospital Example
Three Issues:
Investment
CostRevenueInvestmentonReturn
17

•5–19
Figure 6–3 Return on Assets (Net Income/Assets) 5-Year Average – 2004 to 2008
18
•5–20
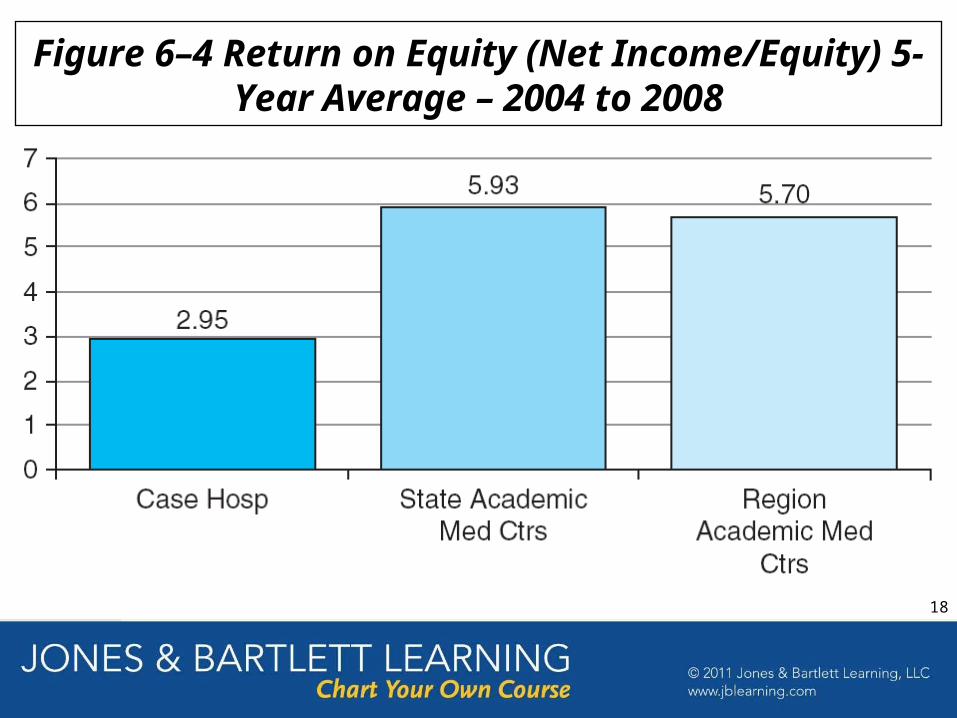
Figure 6–4 Return on Equity (Net Income/Equity) 5-Year Average – 2004 to 2008
18
•5–21
Reasonableness of Costs, Case Hospital Example
1. Medicare cost per discharge – Case-mix- and wage-index adjusted (MCPD)
2. Medicare cost per outpatient claim – relative-weight and wage-index adjusted (MCPC)
The hospital cost index (HCI) is then constructed as follows:
avgUS
MCPCxrevenueOutpatient%
avgUS
MCPDxrevenueInpatient%HCI
Cost Assessment Methodology:
20
•5–22
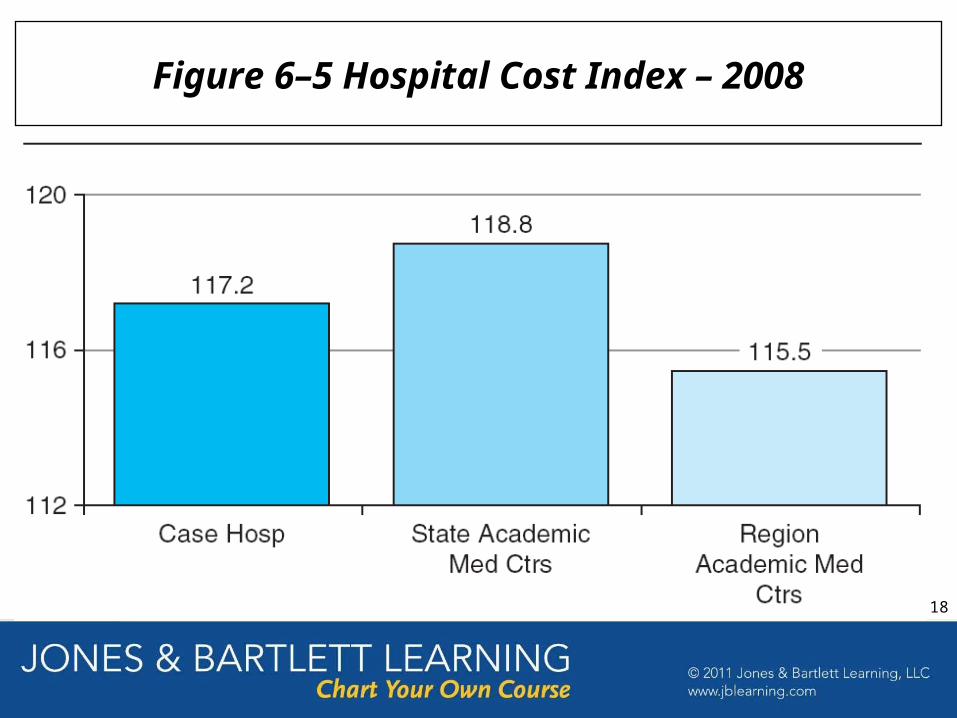
Figure 6–5 Hospital Cost Index – 2008
18
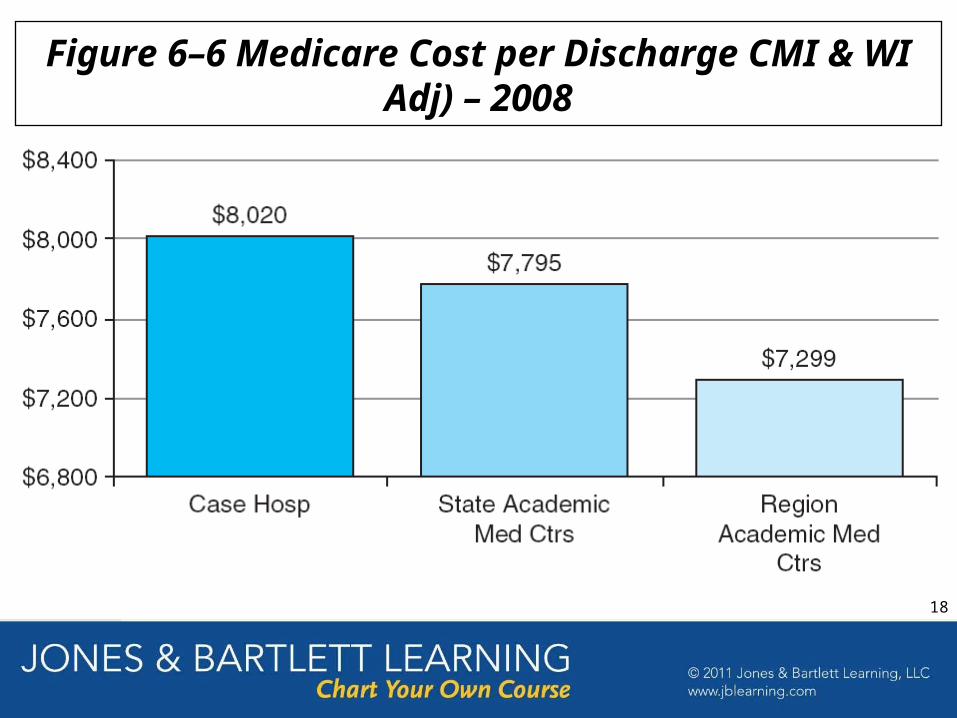
Figure 6–6 Medicare Cost per Discharge CMI & WI Adj) – 2008
18
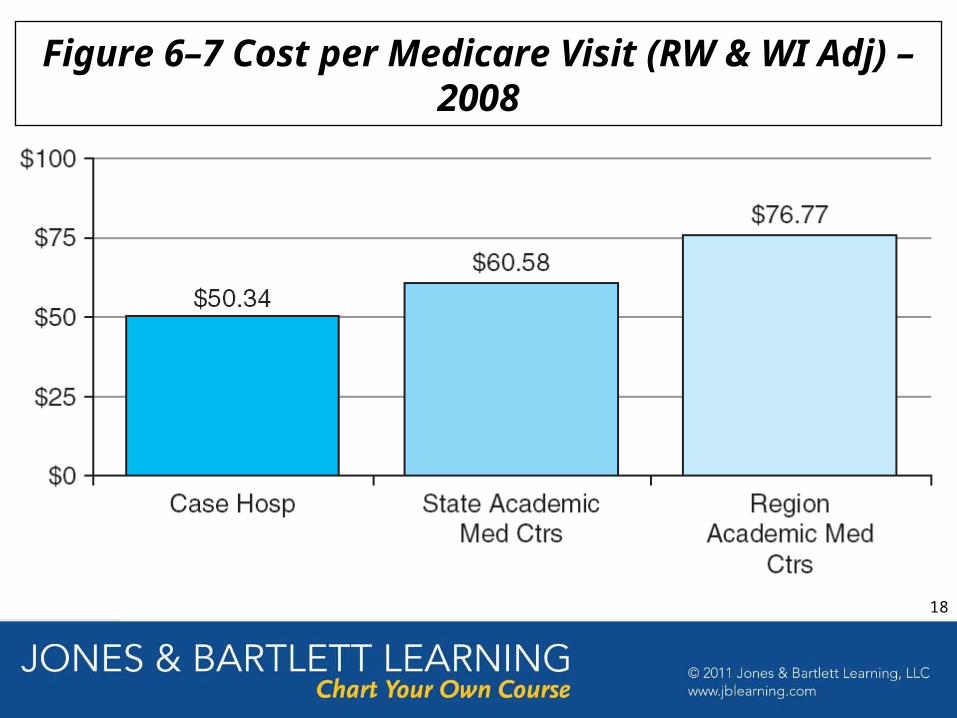
Figure 6–7 Cost per Medicare Visit (RW & WI Adj) –2008
18
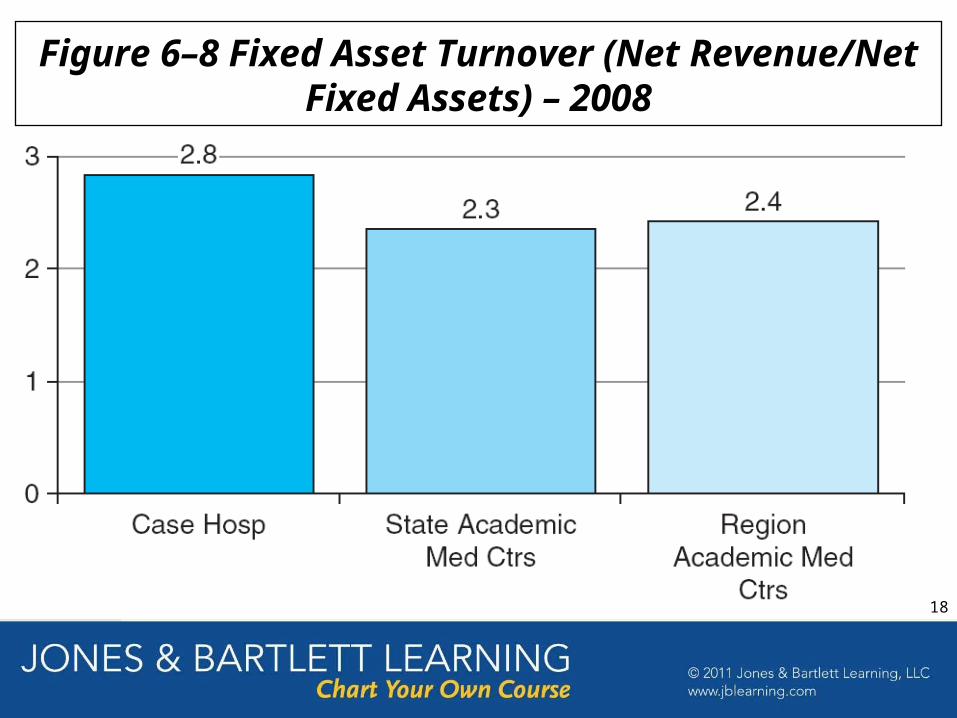
Figure 6–8 Fixed Asset Turnover (Net Revenue/Net Fixed Assets) – 2008
18
•5–26
Case Hospital is not realizing excessive profits
Costs at Case Hospital are consistent with expected values and are reasonable
Investment at Case Hospital is reasonable and not excessive
Therefore prices must be reasonable
ROI Method—Summary, Case Hospital Example
Conclusions:
25
•5–27
Compare with similar hospitals and/or
Compare with hospitals in the same region
Comparison-of-Charges Method, Case Hospital Example
General Methodology:
Compare with all academic centers in California
Compare with regional average for academic medical centers (cost-of-living adjusted)
Case Hospital:
26
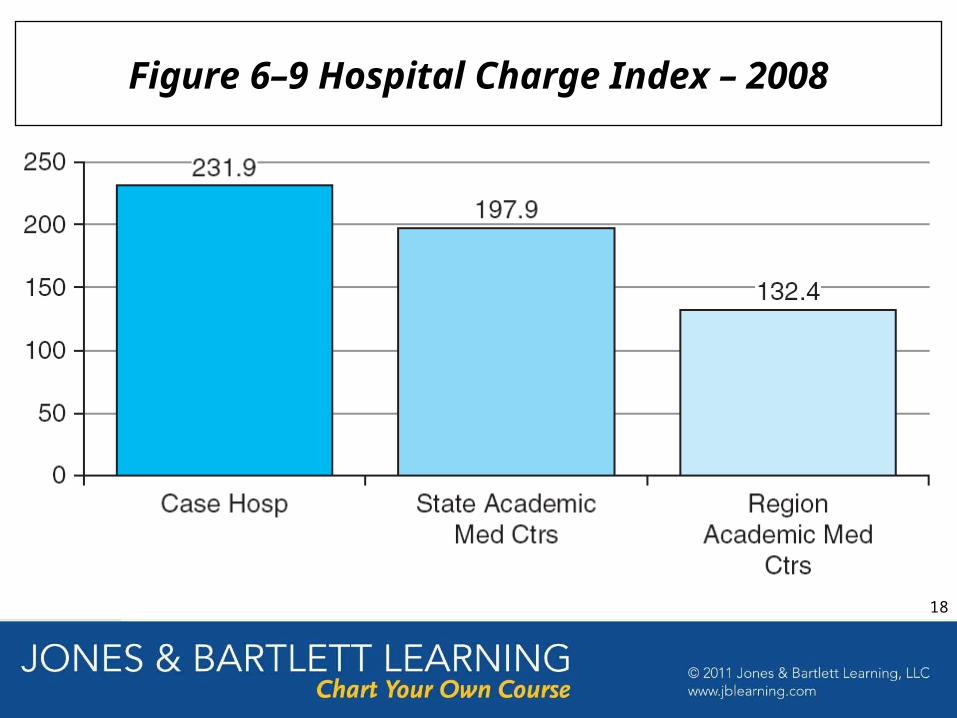
Figure 6–9 Hospital Charge Index – 2008
18

Figure 6–10 Medicare Charge per Discharge (CMI & WI Adj) – 2008
18
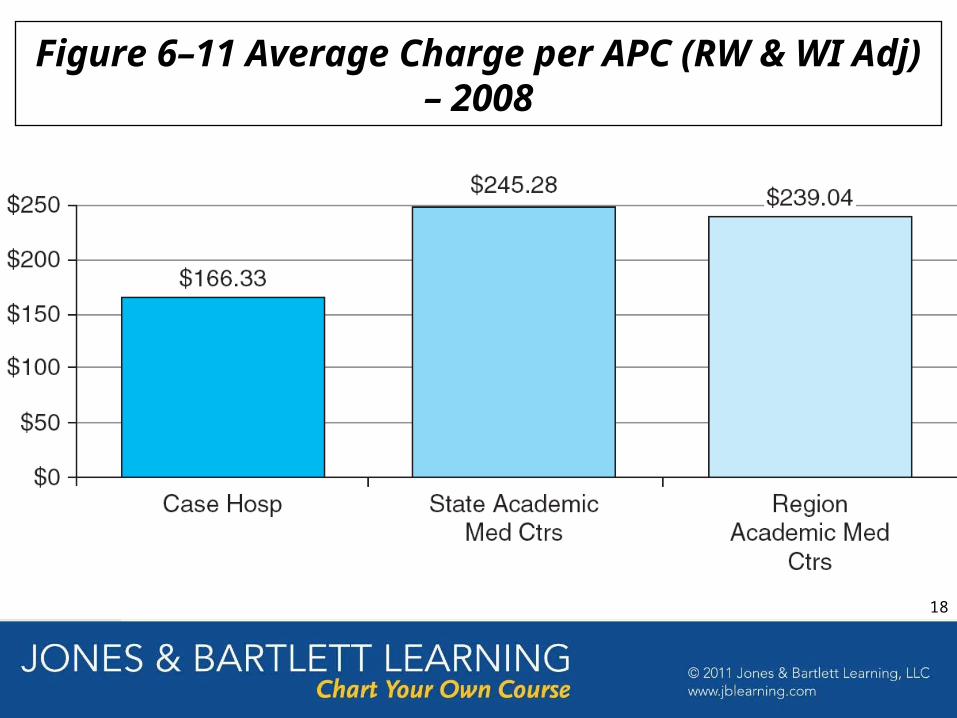
Figure 6–11 Average Charge per APC (RW & WI Adj) – 2008
18
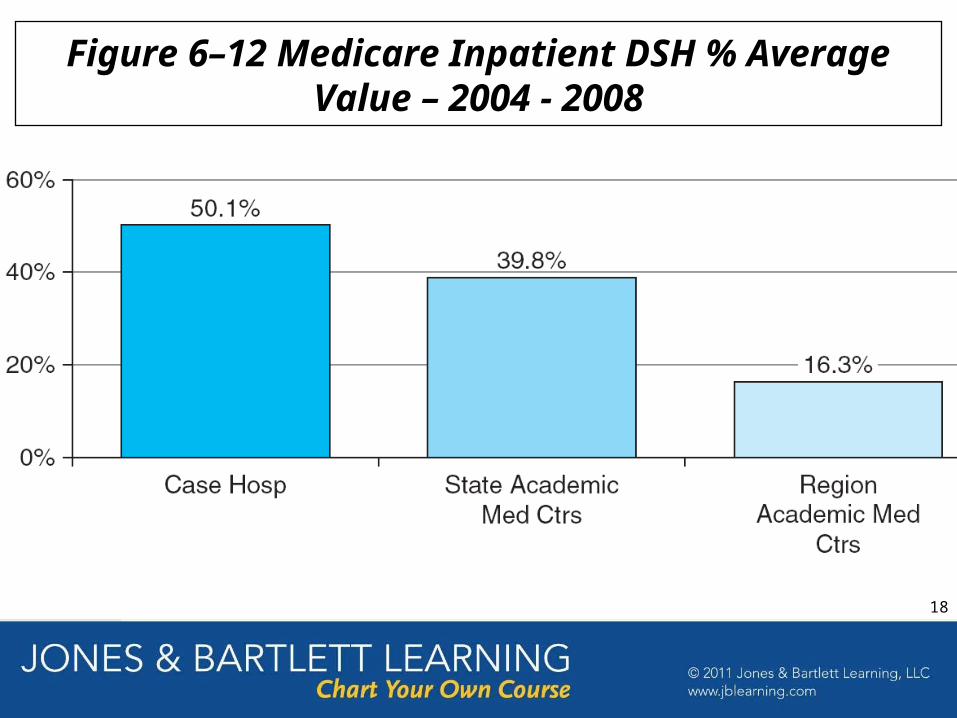
Figure 6–12 Medicare Inpatient DSH % Average Value – 2004 - 2008
18
Negotiating Managed Care Contracts
• Contract negotiation is critical to continued financial solvency
• Contract negotiation involved 2 key areas– Contract language– Payment rates
•5–32
31

•5–33
Managed-Care Contract Negotiation
1. Remove contract ambiguity
2. Eliminate retroactive denials
3. Establish a reasonable appeal process
4. Define clean claims
5. Remove most favored nation (MFN) clauses
6. Prohibit silent PPO arrangements
7. Include terms for outliers or technology-driven increases
8. Establish ability to recover payment after termination
9. Preserve the ability to be paid for services
10. Minimize health plan rate differentials
10 Important Areas of Managed-Care Contract Language:
32
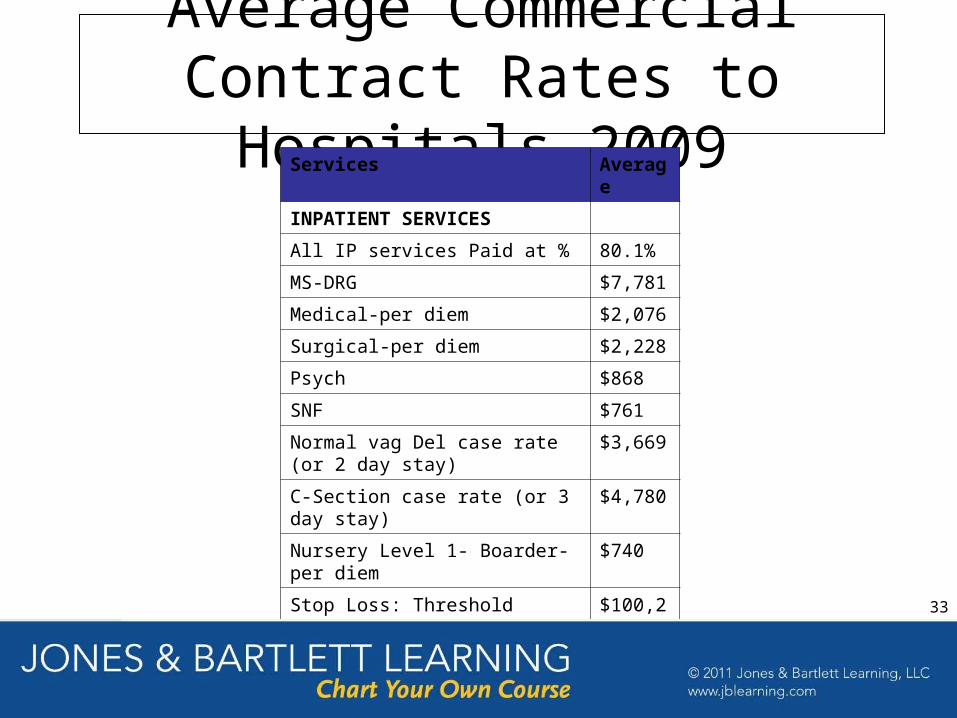
Average Commercial Contract Rates to Hospitals 2009
Services Average
INPATIENT SERVICES
All IP services Paid at % 80.1%
MS-DRG $7,781
Medical-per diem $2,076
Surgical-per diem $2,228
Psych $868
SNF $761
Normal vag Del case rate (or 2 day stay)
$3,669
C-Section case rate (or 3 day stay) $4,780
Nursery Level 1- Boarder-per diem $740
Stop Loss: Threshold $100,212
Stop Loss Charges paid at %: 63.5%
Rate Increase Limit % 5.8%
•5–34
33

Average Commercial
Contract Rates to Hospitals 2009
Outpatient Services
All OP services Paid at % 79.8%
Emergency Department Paid at % 74.5%
Emergency Department-Case Rate $667
Observation Paid at % 73.5%
Observation case rate-per hour $65
Physical Therapy Paid at % 74.6%
PT case rate-per visit $147
MRI OP Paid at % 76.4%
MRI OP-case rate $1,009
Outpatient Surgery Paid at % 74.7%
OP Surgery Group-case rate $2,569
OP Surg Group 1-case rate $1,280
OP Surg Group 2-case rate $1,632
OP Surg Group 3-case rate $2,011
OP Surg Group 4-case rate $2,448
OP Surg Group 5-case rate $2,894
OP Surg Group 6-case rate $3,116
OP Surg Group 7-case rate $3,964
OP Surg Group 8-case rate $4,718
OP Surg Group 9-case rate $5,875
•5–35
34
Summary
• Revenue generation is critical to financial solvency
• Revenue generation is impacted by 3 areas:– Pricing– Contract negotiation– Coding and billing
• Inadequate payments by many government payers force healthcare providers to “cost shift”
•5–36
35
Related Documents











