World Health Organization Regional Office for the Western Pacific reaching the POOR CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
World Health OrganizationRegional Office for the Western Pacific
r e a c h i n g t h e P O O RCHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION
Acknowledgements:
The main contributors to this document are: Sarah Coll-Black, Pieter Van Maaren, Dongil Ahn and Takeshi Kasai, Stop TB Unit, and Anjana Bhushan, Health Systems Unit of the World Health Organization Regional Office for the Western Pacific.
The team gratefully acknowledges the work on TB and poverty commissioned by the Stop TB Partnership in Geneva, of which WHO Headquarters serves as Secretariat. In particular, this document builds on Tuberculosis, poverty and inequity: a review of the literature and discussion of issues (2002), by Christy Hanson and A systematic analysis of TB and poverty (2003), by Bertha Nhlema, Julia Kemp, Ger Steenbergen, Sally Theobald, Shenglan Tang, and Bertel Squire, both commissioned by the Stop TB Partnership.
Photograph credits: pp. 11, FAO/19649/G. Bizzarri; pp. 2, FAO/19665/G. Bizzari; cover, FAO/19669/G. Bizzarri; pp. 22, FAO/19717/G. Bizzarri; pp. 3, FAO/15685/P. Gigli; pp. 19, FAO/19197/P. Johnson; pp. 15, International Labour Organization/Deloche P.; pp. 25, 34, International Labour Organization/Rain N.; pp. 1, 6, 13, 14, WHO/WPRO; pp. i, www.photos.com.
WHO Library Cataloguing in Publication Data
Reaching the poor: challenges for the TB programmes in the Western Pacific Region
1. Tuberculosis. 2. Poverty. 3. Directly observed therapy.
ISBN 92 9061 093 X (NLM Classification: WF 200)
© World Health Organization 2004All rights reserved.
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers' products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
The World Health Organization does not warrant that the information contained in this publication is complete and correct and shall not be liable for any damages incurred as a result of its use.
Publications of the World Health Organization can be obtained from Marketing and Dissemination, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel: +41 22 791 2476; fax: +41 22 791 4857; email: [email protected]). Requests for permission to reproduce WHO publications, in part or in whole, or to translate them - whether for sale or for noncommercial distribution - should be addressed to Publications, at the above address (fax: +41 22 791 4806; email: [email protected]). For WHO Western Pacific Regional Publications, request for permission to reproduce should be addressed to Publications Office, World Health Organization, Regional Office for the Western Pacific, P.O. Box 2932, 1000, Manila, Philippines, Fax. No. (632) 521-1036, email: [email protected]

Poverty can influence the way the poor perceive their illness,
their health seeking behaviour, when and where they access
diagnosis and proper treatment, the quality of care they receive
and whether they achieve a successful outcome.

TABLE OF CONTENTS iii
Table of Contents
List of Abbreviations Foreword Executive Summary
1 What is poverty?
2 How are poverty and health related?
3 What is the relationship between poverty and TB?
4 Does effective TB control reduce poverty?
5 Why may DOTS be failing to reach the poor?
6 How should TB programmes improve access for the poor to DOTS?
List of Figures
List of Boxes
References Endnotes
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• •
• • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
ivvvi
1
32.1 Poverty shapes the global burden of disease 42.2 The poor have less access to quality health services 5
63.1 Why the poor are at greater risk of TB 73.2 How TB causes and perpetuates poverty: the socio-economic costs of TB to patients and families 83.3 How TB causes and perpetuates poverty: TB hinders economic growth and social development 93.4 The reinforcing cycle of poverty and TB 10
114.1 DOTS effectively reduces the risk of TB 124.2 How DOTS contributes to poverty reduction 134.3 Is DOTS sufficiently pro-poor? 134.4 DOTS may not be reaching the poor 13
155.1 Poverty restricts health seeking along the pathway to cure 165.2 Pathway to cure: barriers delay and impede access by the poor to DOTS 165.3 Factors that prevent or delay the poor from accessing DOTS 17
226.1 Improving access to meet the TB control targets 236.2 Strategies by the TB programme to improve access by the poor to DOTS 236.3 Strategies beyond the TB programme 256.4 Integrating poverty into TB control: next steps 25
Figure 1 Proportion of population living below US$ 1 a day in six countries in the Western Pacific Region 2Figure 2 Health status and poverty, Viet Nam 4Figure 3 The benefit incidence of public spending by income quintile, Cambodia 2002 5Figure 4 TB burden in poor and rich countries 7Figure 5 TB prevalence rates among the poor and non-poor, Philippines 7Figure 6 Trends in smear-positive TB, Viet Nam: 1990 - 1999 9Figure 7 Prevalence of smear-positive TB by ethnic group, China 10Figure 8 Treatment success rates in the seven high burden countries, Western Pacific Region 12Figure 9 The model: Barriers along the pathway to cure 16Figure 10 How barriers prevent the poor from accessing DOTS 17Figure 11 Reasons for treatment delay, China 18Figure 12 Where TB symptomatics go for help, Philippines 21Figure 13 Case detection rates in high burden countries in the Region, 2002 23
Box 1 Gender and TB: some evidence from Viet Nam 8Box 2 TB and social exclusion: ethnic minorities, prisoners, and people living with HIV/AIDS 10
2631
CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION
List of Abbreviations
ADB Asian Development BankAIDS Acquired immunodeficiency syndromeARI Annual risk of infectionCHW Community health workerDALYs Disability-adjusted life yearsDOTS Directly observed treatment, short-courseDOT Directly observed treatmentGDP Gross domestic productGNI Gross national incomeGFATM Global Fund to Fight AIDS, Tuberculosis and MalariaHDI Human Development IndexHIV Human immunodeficiency virusIEC Information, education and communicationIMR Infant mortality rateMDGs Millennium Development GoalsNGOs Nongovernmental organizationsNTP National TB ProgrammePHC Primary health carePRSP Poverty Reduction Strategy Paper TAG Technical Advisory GroupTB TuberculosisTB/HIV HIV-associated TBUNDP United Nations Development ProgrammeWB World BankWHO World Health OrganizationWPRO Western Pacific Regional Office
iv LIST OF ABBREVIATIONS
r e a c h i n g t h e P O O R
Foreword
In the Western Pacific Region, 1000 people die of tuberculosis (TB) every day; many of them are among the poorest and most vulnerable. TB is a disease of poverty that thrives on deprivation and inequality. Attacking those in the most economically and socially productive age group of 15–54, TB leaves disaster in its wake. The loss of productive labour and frequently unaffordable expense of seeking treatment can thrust TB patients and their families deeper into poverty. When aggregated to the national level, the cost of TB to economic development and poverty reduction is tremendous.
In 1999, WHO's Regional Committee for the Western Pacific declared TB a "regional crisis". Launched in response, the Stop TB Special Project aims to reduce the prevalence and mortality of tuberculosis in the Region by half by 2010. While important progress has been made in the battle against TB, we must strive to reach those most in need–poor and marginalized communities in countries with the highest burden of TB in the Region–to ensure the 2010 target is met.
The Western Pacific Region is seeking to integrate a pro-poor focus in TB control programmes. Reaching the poor: challenges for TB programmes in the Western Pacific Region is the first step in this direction. Targeting national TB programme managers and policy-makers from countries and areas in the Western Pacific Region, this publication aims to increase awareness of the relationship between poverty and TB. This will be followed by a Regional Framework on TB and poverty that will systematically integrate poverty into TB control.
This initiative builds on a series of recent events reflecting the growing commitment internationally to addressing poverty and TB as a joint challenge. Both poverty reduction and TB control are integral to the Millennium Development Goals, which WHO is committed to supporting. In 2002, the Stop TB Partnership in Geneva, of which WHO Headquarters serves as Secretariat, created a TB-Poverty Advisory Committee and commissioned further work on TB and poverty. In September 2003, the Regional Committee for the Western Pacific called for a focus on poverty in TB control to improve access by the poor to DOTS. This resolution followed a recommendation made in an external thematic evaluation of the Stop TB Special Project of the Western Pacific Regional Office conducted in early 2003.
Building on work done at the global level, Reaching the poor: challenges for TB programmes in the Western Pacific Region presents evidence from the Region on the relationship between poverty and TB. We hope to assist national TB programme managers and policy-makers improve access for the poor to DOTS. Notably, the Stop TB Unit and the Health Systems Unit in the Western Pacific Regional Office developed this publication jointly. We hope that such collaboration will be strengthened and expanded to other technical programmes in the days ahead.
Now it is time to move beyond "business as usual", to promote greater equity in access to TB control services, thus ensuring that the poor and marginalized can particularly benefit from DOTS.
Shigeru Omi, MD, Ph.DRegional Director
FOREWORD v
CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION
Executive Summary
Globally, over 98% of the deaths caused by tuberculosis (TB) annually are in developing countries. Within the Western Pacific Region, the seven countries that account for 94% of the TB prevalence are low or lower middle-income economies. Within countries, as well, poor and marginalized communities suffer disproportionately from TB. Importantly, TB affects the most economically and socially productive age group, as 77% of TB deaths occur within the ages of 15 – 54.
This evidence points to the important relationship between poverty and TB. The deprivation associated with poverty, such as overcrowding, poor ventilation and malnutrition, increases the rate of transmission and progression from infection to disease. In turn, the costs of TB can further impoverish poor households. This is because poor households must dedicate a larger proportion of their income to meet the direct and indirect costs of seeking TB care than the non-poor. The opportunity costs are likewise higher for the poor than non-poor. For the poor, a decrease in productivity or an increase in time away from work because of illness leads to a reduction in income. Moreover, coping mechanisms employed by poor households during periods of illness may reduce household productivity in the long-term. TB has important social costs as well, which are more likely to affect women with TB than men. For example, stigma and isolation resulting from TB can reduce an individual's social position.
Since the economic and social costs of TB are high, effective TB control, such as directly observed treatment, short-course (DOTS), may indirectly reduce poverty, through longer lives and increased productivity. However, the extent to which national TB programmes (NTPs) respond to the needs of the poor cannot be accurately assessed because routine monitoring and recording systems do not provide information on patients by socio-economic status. Health-related research from beyond TB offers many reasons to suspect that, even with free diagnosis and treatment, DOTS may not be reaching the poor. Evidence from within TB is beginning to reveal similar trends: the non-poor may be capturing most of the benefits of DOTS, and DOTS programmes may be failing to reach many of the poor. In particular, the current case detection strategy may be "missing" cases, especially in hard-to-reach or marginalized populations.
DOTS may be failing to reach the poor because of the constraints poverty may place on health seeking. Specifically, poverty-related barriers that obstruct access along the pathway to cure (from recognition of symptoms to achieving a cure) may delay or prevent poor TB patients from accessing TB control services. These barriers include: physical barriers; lack of information and awareness; economic costs; and lack of health system responsiveness, in both the public and private sectors.
Such impediments may undermine progress towards achieving the Regional targets for TB control. Strategies are thus needed to improve the accessibility of DOTS for the poor. These strategies will also begin to address inequity in the burden of TB and access to TB control. The first priority of NTPs is to ensure the availability of quality TB services by implementing DOTS across the country. As a next step, NTPs should focus on improving access for the poor to DOTS. A number of strategies can be identified to address the aforementioned barriers, which will be elaborated upon further in the forthcoming Regional Framework on TB and poverty.
vi EXECUTIVE SUMMARY
r e a c h i n g t h e P O O R
What is poverty?
An important feature
of poverty is that it often
overlaps with and reinforces
other types of social
exclusion, such as those
based on race, gender
or ethnicity.
1
r e a c h i n g t h e P O O R CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION
What is poverty?
Traditionally, poverty has been conceptualized in terms of income, with the poor being defined as those living below a given income level. Poverty can be also
1understood as pronounced deprivation in well-being. However, poverty is increasingly recognized as being a multidimensional phenomenon, encompassing not just low income but also lack of assets, access to skills, resources, opportunities, services, and power or voice to influence decisions that affect your life. This more comprehensive understanding of poverty also captures better how the poor themselves define their own
2situation.
An important feature of poverty is that it often overlaps with and reinforces other types of social exclusion, such as those based on race, gender or ethnicity. In the Western Pacific Region, the social exclusion of indigenous people is often reflected in the relatively lower levels of development in the areas where they live.
3The Human Development Index (HDI) of provinces in the Philippines, for example, ranges from a high of 0.925 in Metro Manila, to a low of 0.372 in provinces peopled by indigenous populations and other marginalized groups,
4 including the Muslims of Mindanao.
Using a measure of income poverty, the World Bank estimates that there are 1.2 billion people living in extreme poverty, equal to 23.3% of the population in low
5and middle-income countries. An estimated 24% of the world's poor live in the 6
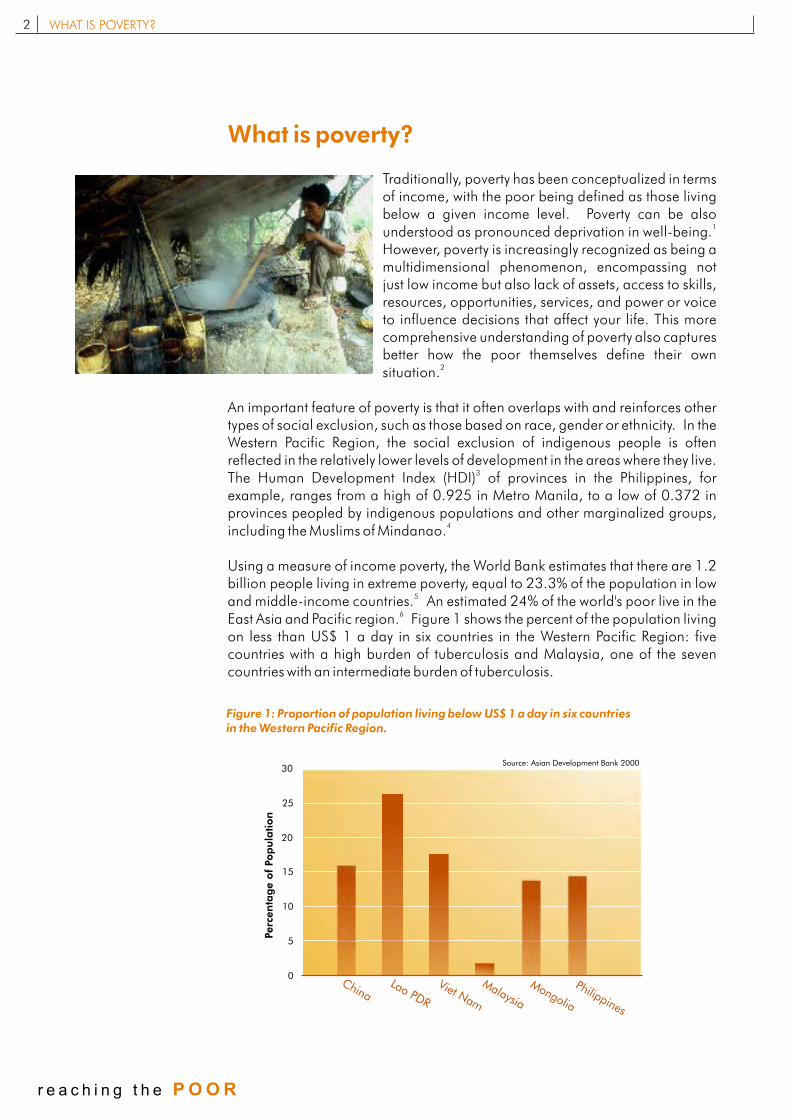
East Asia and Pacific region. Figure 1 shows the percent of the population living on less than US$ 1 a day in six countries in the Western Pacific Region: five countries with a high burden of tuberculosis and Malaysia, one of the seven countries with an intermediate burden of tuberculosis.
Figure 1: Proportion of population living below US$ 1 a day in six countries in the Western Pacific Region.
WHAT IS POVERTY?
5
10
15
20
25
30
0h n
Ci a o P
R
LaD
Viet Nam
Malaysia
M
o i
ongl a
Phil ppinei
s
Perc
en
tag
e o
f Pop
ula
tion
Source: Asian Development Bank 2000
2
r e a c h i n g t h e P O O R
How are poverty
and health related?
For poor households,
the relationship between
poverty and health
is clear: poverty leads
to ill health, and ill health
leads to increased poverty.
2
r e a c h i n g t h e P O O R CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION
How are poverty and health related?
2.1 Poverty shapes the global burden of disease
Poverty and health are closely interrelated. A simplified representation of this interrelationship consists of two reinforcing cycles:
! The vicious circle:Poverty breeds ill healthIll health causes poverty
! The virtuous circle:Higher income is linked to good healthGood health is linked to higher income and welfare
Whether at household, community or national level, poverty is recognized as a significant determinant of ill health. The global pattern of disease mirrors inequalities in income and wealth distribution across countries. The disparity in
7the global burden of communicable diseases is stark: the 20% of the global population living in the poorest countries suffers almost half the death and disability caused by communicable diseases, while the 20% of the global population living in the richest countries experiences a mere 4.2% of global
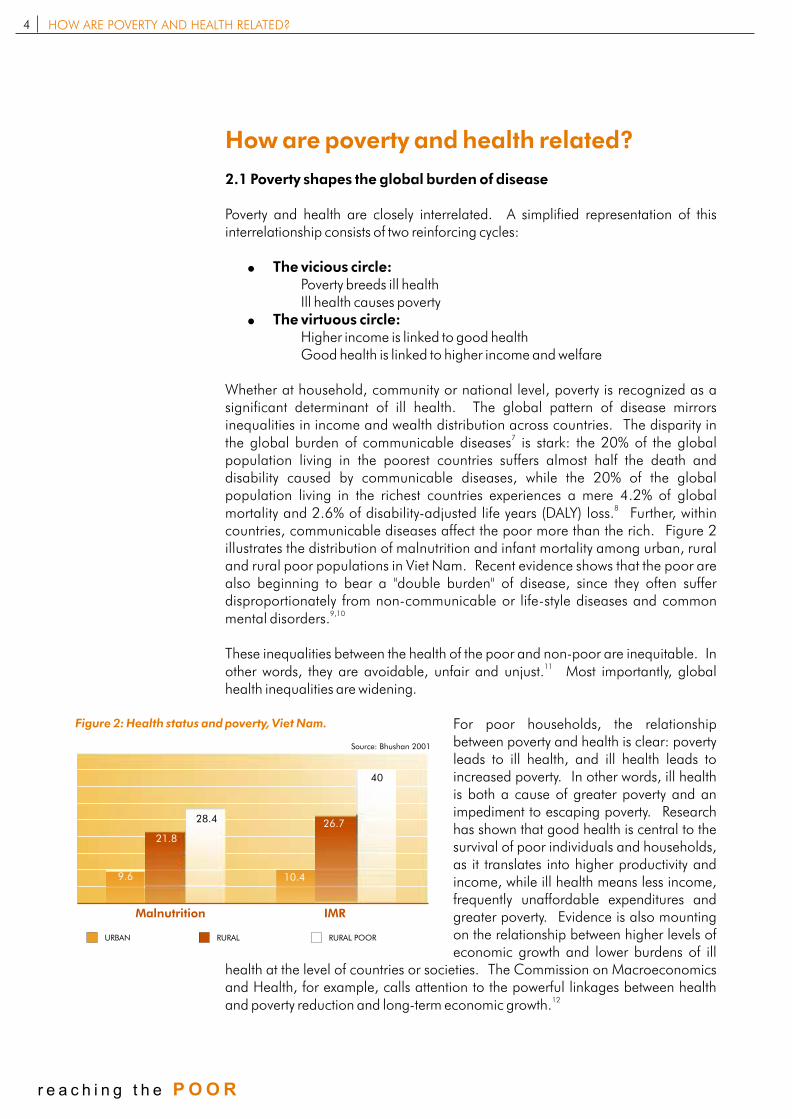
8mortality and 2.6% of disability-adjusted life years (DALY) loss. Further, within countries, communicable diseases affect the poor more than the rich. Figure 2 illustrates the distribution of malnutrition and infant mortality among urban, rural and rural poor populations in Viet Nam. Recent evidence shows that the poor are also beginning to bear a "double burden" of disease, since they often suffer disproportionately from non-communicable or life-style diseases and common
9,10mental disorders.
These inequalities between the health of the poor and non-poor are inequitable. In 11
other words, they are avoidable, unfair and unjust. Most importantly, global health inequalities are widening.
For poor households, the relationship between poverty and health is clear: poverty leads to ill health, and ill health leads to increased poverty. In other words, ill health is both a cause of greater poverty and an impediment to escaping poverty. Research has shown that good health is central to the survival of poor individuals and households, as it translates into higher productivity and income, while ill health means less income, frequently unaffordable expenditures and greater poverty. Evidence is also mounting on the relationship between higher levels of economic growth and lower burdens of ill
health at the level of countries or societies. The Commission on Macroeconomics and Health, for example, calls attention to the powerful linkages between health
12and poverty reduction and long-term economic growth.
Malnutrition IMR
URBAN RURAL RURAL POOR
9.6
21.8
28.4
10.4
26.7
40
Source: Bhushan 2001
Figure 2: Health status and poverty, Viet Nam.
HOW ARE POVERTY AND HEALTH RELATED?4
r e a c h i n g t h e P O O R
2.2 The poor have less access to quality health services
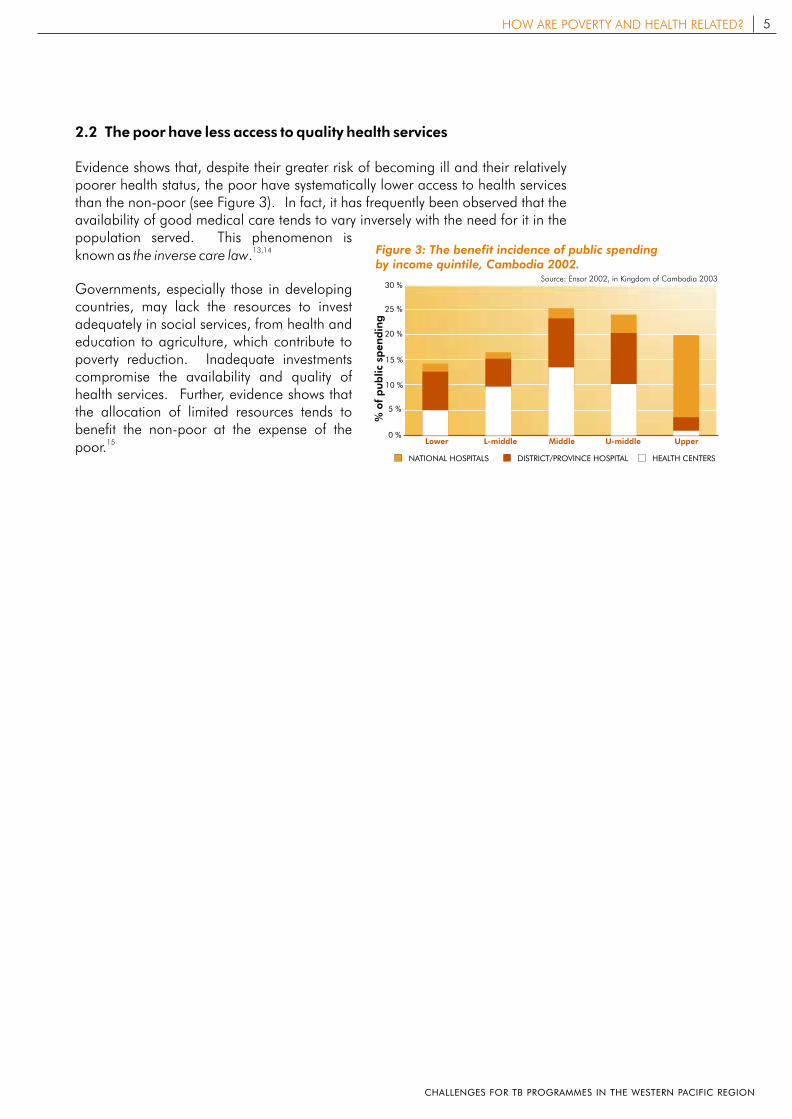
Evidence shows that, despite their greater risk of becoming ill and their relatively poorer health status, the poor have systematically lower access to health services than the non-poor (see Figure 3). In fact, it has frequently been observed that the availability of good medical care tends to vary inversely with the need for it in the population served. This phenomenon is
13,14known as the inverse care law.
Governments, especially those in developing countries, may lack the resources to invest adequately in social services, from health and education to agriculture, which contribute to poverty reduction. Inadequate investments compromise the availability and quality of health services. Further, evidence shows that the allocation of limited resources tends to benefit the non-poor at the expense of the
15poor.
NATIONAL HOSPITALS DISTRICT/PROVINCE HOSPITAL HEALTH CENTERS
% o
f p
ub
lic
spen
din
g
Lower L-middle
5 %
10 %
15 %
20 %
25 %
30 %
0 %Middle U-middle Upper
Figure 3: The benefit incidence of public spending by income quintile, Cambodia 2002.
Source: Ensor 2002, in Kingdom of Cambodia 2003
5HOW ARE POVERTY AND HEALTH RELATED?
CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION
What is the relationship
between poverty and TB?
Within countries, the distribution
of TB is higher among the poor
than among the non-poor
3
r e a c h i n g t h e P O O R CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION
What is the relationship
between poverty and TB?
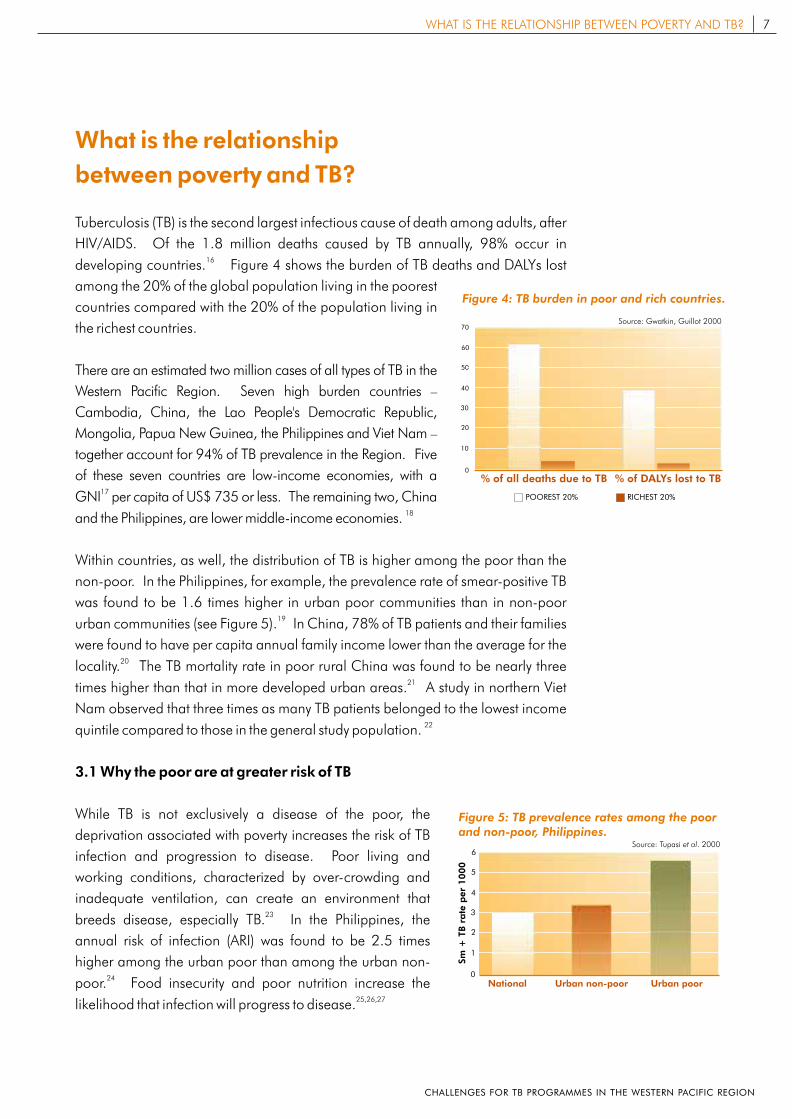
Tuberculosis (TB) is the second largest infectious cause of death among adults, after
HIV/AIDS. Of the 1.8 million deaths caused by TB annually, 98% occur in 16
developing countries. Figure 4 shows the burden of TB deaths and DALYs lost
among the 20% of the global population living in the poorest
countries compared with the 20% of the population living in
the richest countries.
There are an estimated two million cases of all types of TB in the
Western Pacific Region. Seven high burden countries –
Cambodia, China, the Lao People's Democratic Republic,
Mongolia, Papua New Guinea, the Philippines and Viet Nam –
together account for 94% of TB prevalence in the Region. Five
of these seven countries are low-income economies, with a 17
GNI per capita of US$ 735 or less. The remaining two, China 18and the Philippines, are lower middle-income economies.
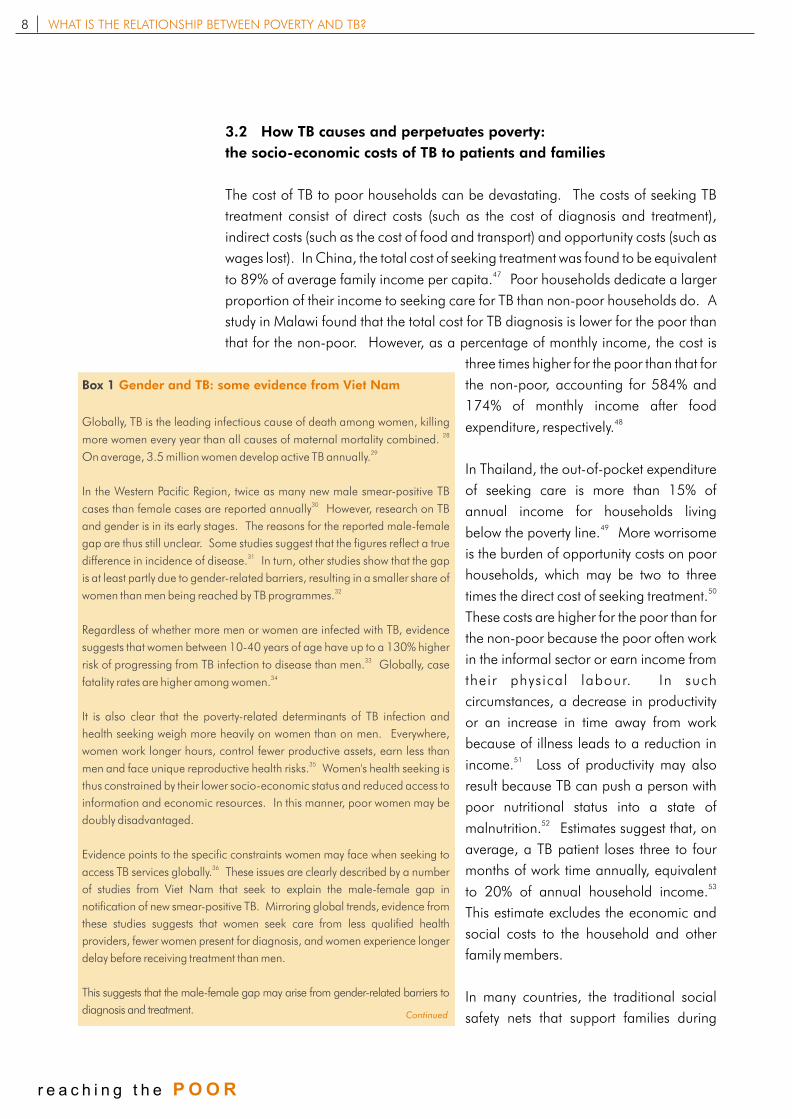
Within countries, as well, the distribution of TB is higher among the poor than the
non-poor. In the Philippines, for example, the prevalence rate of smear-positive TB
was found to be 1.6 times higher in urban poor communities than in non-poor 19
urban communities (see Figure 5). In China, 78% of TB patients and their families
were found to have per capita annual family income lower than the average for the 20locality. The TB mortality rate in poor rural China was found to be nearly three
21times higher than that in more developed urban areas. A study in northern Viet
Nam observed that three times as many TB patients belonged to the lowest income 22quintile compared to those in the general study population.
3.1 Why the poor are at greater risk of TB
While TB is not exclusively a disease of the poor, the
deprivation associated with poverty increases the risk of TB
infection and progression to disease. Poor living and
working conditions, characterized by over-crowding and
inadequate ventilation, can create an environment that 23breeds disease, especially TB. In the Philippines, the
annual risk of infection (ARI) was found to be 2.5 times
higher among the urban poor than among the urban non-24
poor. Food insecurity and poor nutrition increase the 25,26,27likelihood that infection will progress to disease.
POOREST 20% RICHEST 20%
% of DALYs lost to TB0
10
20
30
40
50
60
70
% of all deaths due to TB
Source: Gwatkin, Guillot 2000
Figure 4: TB burden in poor and rich countries.
Sm
+ T
B r
ate
per
1000
Urban poor0
1
2
3
4
5
6
National Urban non-poor
Source: Tupasi et al. 2000
Figure 5: TB prevalence rates among the poor and non-poor, Philippines.
7WHAT IS THE RELATIONSHIP BETWEEN POVERTY AND TB?
CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION
3.2 How TB causes and perpetuates poverty:
the socio-economic costs of TB to patients and families
The cost of TB to poor households can be devastating. The costs of seeking TB
treatment consist of direct costs (such as the cost of diagnosis and treatment),
indirect costs (such as the cost of food and transport) and opportunity costs (such as
wages lost). In China, the total cost of seeking treatment was found to be equivalent 47
to 89% of average family income per capita. Poor households dedicate a larger
proportion of their income to seeking care for TB than non-poor households do. A
study in Malawi found that the total cost for TB diagnosis is lower for the poor than
that for the non-poor. However, as a percentage of monthly income, the cost is
three times higher for the poor than that for
the non-poor, accounting for 584% and
174% of monthly income after food 48
expenditure, respectively.
In Thailand, the out-of-pocket expenditure
of seeking care is more than 15% of
annual income for households living 49below the poverty line. More worrisome
is the burden of opportunity costs on poor
households, which may be two to three 50
times the direct cost of seeking treatment.
These costs are higher for the poor than for
the non-poor because the poor often work
in the informal sector or earn income from
their physical labour. In such
circumstances, a decrease in productivity
or an increase in time away from work
because of illness leads to a reduction in 51
income. Loss of productivity may also
result because TB can push a person with
poor nutritional status into a state of 52malnutrition. Estimates suggest that, on
average, a TB patient loses three to four
months of work time annually, equivalent 53
to 20% of annual household income.
This estimate excludes the economic and
social costs to the household and other
family members.
In many countries, the traditional social
safety nets that support families during
8 WHAT IS THE RELATIONSHIP BETWEEN POVERTY AND TB?
r e a c h i n g t h e P O O R
Box 1
Globally, TB is the leading infectious cause of death among women, killing 28more women every year than all causes of maternal mortality combined.
29On average, 3.5 million women develop active TB annually.
In the Western Pacific Region, twice as many new male smear-positive TB 30cases than female cases are reported annually However, research on TB
and gender is in its early stages. The reasons for the reported male-female
gap are thus still unclear. Some studies suggest that the figures reflect a true 31difference in incidence of disease. In turn, other studies show that the gap
is at least partly due to gender-related barriers, resulting in a smaller share of 32women than men being reached by TB programmes.
Regardless of whether more men or women are infected with TB, evidence
suggests that women between 10-40 years of age have up to a 130% higher 33risk of progressing from TB infection to disease than men. Globally, case
34fatality rates are higher among women.
It is also clear that the poverty-related determinants of TB infection and
health seeking weigh more heavily on women than on men. Everywhere,
women work longer hours, control fewer productive assets, earn less than 35men and face unique reproductive health risks. Women's health seeking is
thus constrained by their lower socio-economic status and reduced access to
information and economic resources. In this manner, poor women may be
doubly disadvantaged.
Evidence points to the specific constraints women may face when seeking to 36access TB services globally. These issues are clearly described by a number
of studies from Viet Nam that seek to explain the male-female gap in
notification of new smear-positive TB. Mirroring global trends, evidence from
these studies suggests that women seek care from less qualified health
providers, fewer women present for diagnosis, and women experience longer
delay before receiving treatment than men.
This suggests that the male-female gap may arise from gender-related barriers to
diagnosis and treatment.
Gender and TB: some evidence from Viet Nam
Continued
periods of crisis have been eroded. Neither the state nor other actors have filled this 54gap, leaving families to fend for themselves. The poor are more vulnerable to
serious or prolonged illness; meagre resources are dedicated to daily basic needs,
leaving little, if any, savings to buffer against unexpected shocks or periods of 55
income loss.
The coping mechanisms used by poor families in such circumstances may reduce
household productivity in the longer term. Families may reduce expenditure on 56items such as food and clothing to meet the direct and indirect costs of treatment.
The loss of productive labour to illness may be offset by other family members, 57,58
including children, who may be pulled out of school. Households may also sell
their assets or borrow money to cover the
cost of seeking treatment. For example, a
study in Cambodia observed that 40% of 59new landlessness was due to ill health.
Selling assets, especially land, can deprive
households of a future income stream,
while taking children from school forfeits
the long-term economic advantages of
schooling.
TB has important social costs as well.
Stigma and isolation resulting from TB, for
example, can reduce an individual's power
and social position. Numerous studies
show that stigma is more likely to affect
women with TB than men. Negative social
responses to women's illness include
stigma and isolation from families and the
wider community. In contrast, men are
more likely to worry about the financial and
economic consequences of their illness,
such as loss of income, reduced 60,61,62productivity and possible job loss.
3.3 How TB causes and perpetuates
poverty: TB hinders economic
growth and social development
When the costs borne by individual TB
patients and their families are aggregated,
the loss to national productivity and socio-
economic deve lopmen t can be
9WHAT IS THE RELATIONSHIP BETWEEN POVERTY AND TB?
CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION
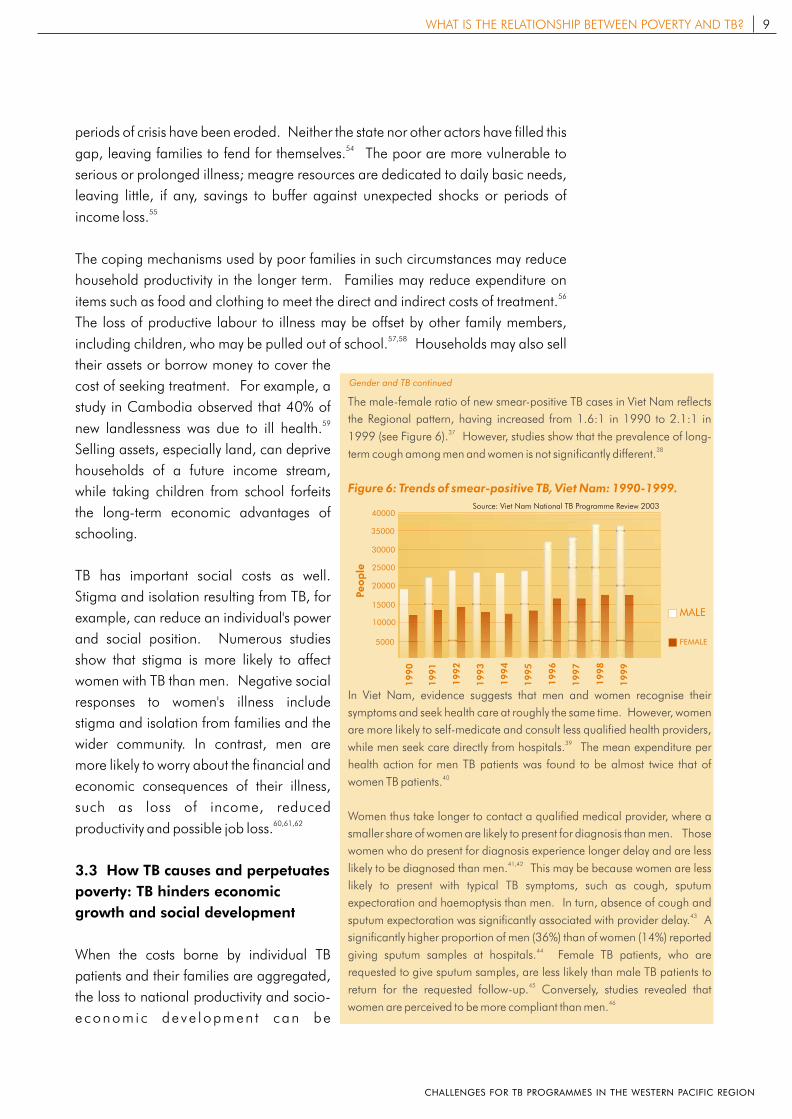
The male-female ratio of new smear-positive TB cases in Viet Nam reflects
the Regional pattern, having increased from 1.6:1 in 1990 to 2.1:1 in 371999 (see Figure 6). However, studies show that the prevalence of long-
38term cough among men and women is not significantly different.
In Viet Nam, evidence suggests that men and women recognise their
symptoms and seek health care at roughly the same time. However, women
are more likely to self-medicate and consult less qualified health providers, 39while men seek care directly from hospitals. The mean expenditure per
health action for men TB patients was found to be almost twice that of 40women TB patients.
Women thus take longer to contact a qualified medical provider, where a
smaller share of women are likely to present for diagnosis than men. Those
women who do present for diagnosis experience longer delay and are less 41,42likely to be diagnosed than men. This may be because women are less
likely to present with typical TB symptoms, such as cough, sputum
expectoration and haemoptysis than men. In turn, absence of cough and 43sputum expectoration was significantly associated with provider delay. A
significantly higher proportion of men (36%) than of women (14%) reported 44giving sputum samples at hospitals. Female TB patients, who are
requested to give sputum samples, are less likely than male TB patients to 45return for the requested follow-up. Conversely, studies revealed that
46women are perceived to be more compliant than men.
Figure 6: Trends of smear-positive TB, Viet Nam: 1990-1999.
Source: Viet Nam National TB Programme Review 2003
5000
10000
15000
20000
25000
30000
35000
40000
Peop
le
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
MALE
FEMALE
Gender and TB continued
tremendous. In the Western Pacific Region, 77% of TB deaths occur within the ages
of 15-54, the most economically and socially productive age group. The global cost
of TB is estimated to amount to US$ 12 billion annually. In 1998, for low and 69
middle-income countries, this meant an annual loss of approximately 0.2% of GDP.
3.4 The reinforcing cycle of poverty and TB
The interrelationship between poverty and TB is further compounded by obstacles
that delay or deter health seeking by the poor. The high cost of seeking treatment,
coupled with low income and other physical and social barriers, such as distance to
a health facility and stigma, reduce the ability of the poor to access health services.
Difficulties in access may be further exacerbated by inadequate quality and
coverage of health care services in both the public and private sectors. Thus, the
poor are less likely to seek and receive timely diagnosis and treatment for TB. A
study in Manila found that respondents with low family income (less than P2000 a 70
month ) were seven times more likely than those with medium and high incomes 71
not to seek medical care. These issues are discussed in greater depth in section 5.
10 WHAT IS THE RELATIONSHIP BETWEEN POVERTY AND TB?
r e a c h i n g t h e P O O R
Box 2
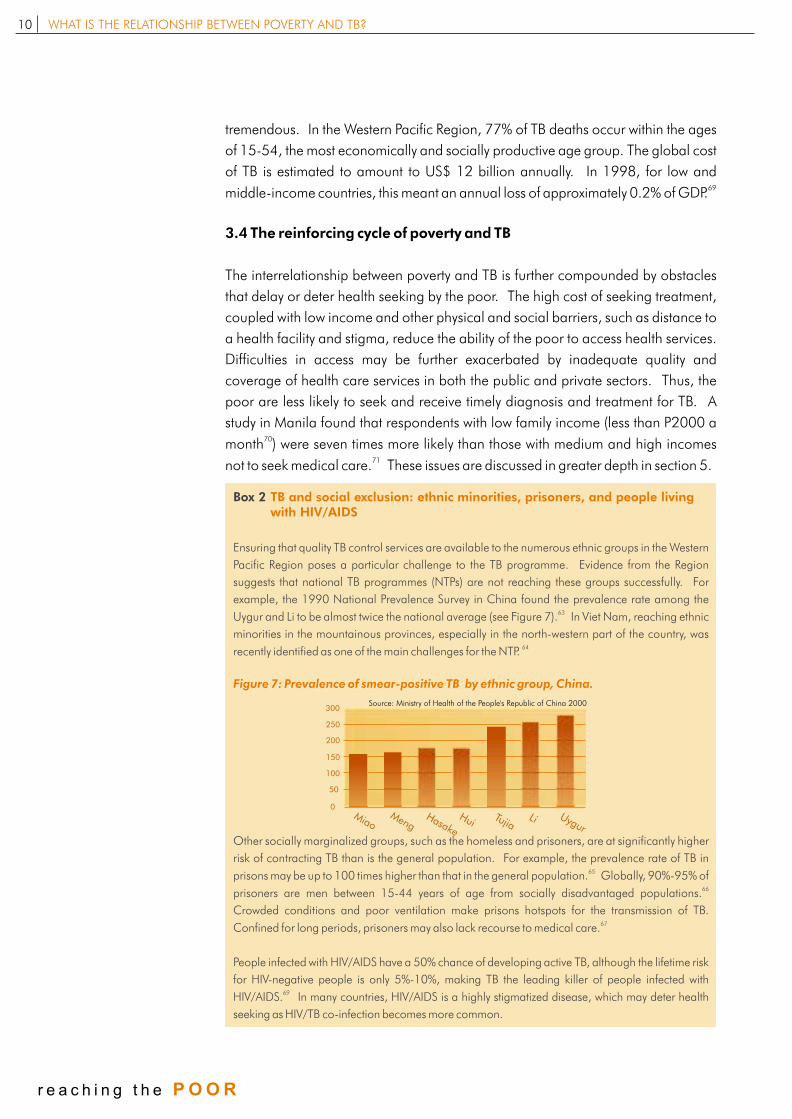
Ensuring that quality TB control services are available to the numerous ethnic groups in the Western
Pacific Region poses a particular challenge to the TB programme. Evidence from the Region
suggests that national TB programmes (NTPs) are not reaching these groups successfully. For
example, the 1990 National Prevalence Survey in China found the prevalence rate among the 63Uygur and Li to be almost twice the national average (see Figure 7). In Viet Nam, reaching ethnic
minorities in the mountainous provinces, especially in the north-western part of the country, was 64recently identified as one of the main challenges for the NTP.
Other socially marginalized groups, such as the homeless and prisoners, are at significantly higher
risk of contracting TB than is the general population. For example, the prevalence rate of TB in 65prisons may be up to 100 times higher than that in the general population. Globally, 90%-95% of
66prisoners are men between 15-44 years of age from socially disadvantaged populations.
Crowded conditions and poor ventilation make prisons hotspots for the transmission of TB. 67Confined for long periods, prisoners may also lack recourse to medical care.
People infected with HIV/AIDS have a 50% chance of developing active TB, although the lifetime risk
for HIV-negative people is only 5%-10%, making TB the leading killer of people infected with 69HIV/AIDS. In many countries, HIV/AIDS is a highly stigmatized disease, which may deter health
seeking as HIV/TB co-infection becomes more common.
TB and social exclusion: ethnic minorities, prisoners, and people living with HIV/AIDS
Figure 7: Prevalence of smear-positive TB by ethnic group, China.
Source: Ministry of Health of the People's Republic of China 2000
0
50
100
150
200
250
300
ygurULiTujia
HuiHasake
MengMiao
Does effective TB control
reduce poverty?
Almost twice as many patients
successfully complete their treatment
under DOTS than do those in
non-DOTS programmes.
In 2001, the regional treatment
success rate for new smear-positive
TB cases stood at 92%.
4
r e a c h i n g t h e P O O R CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION
Does effective TB control reduce poverty?
4.1 DOTS effectively reduces the risk of TB
Economic growth, to the extent it reduces poverty, has a role to play in TB control.
Reducing poverty mitigates some of the environmental factors that nurture the
spread of TB, such as poor housing and malnutrition, and thereby reduces the risk of
TB infection. But reducing poverty does not diminish the existing pool of infectious
TB cases, which are the primary source of infection. Without treatment, seven in ten
people with infectious TB will die of the disease, on average within four to five years 72of onset. Thus, the most effective means of tackling the high burden of TB is
through a comprehensive national TB control programme that cuts the cycle of
transmission, infection and disease. TB control ensures that active TB cases are
cured, reducing the risk of TB infection.
The Stop TB Special Project in the Western Pacific Region aims to reduce the
prevalence and mortality due to TB by half by 2010. The project intensifies efforts,
especially among countries with a high burden of TB, towards realizing the three key
global targets of 100% DOTS coverage, 70% case detection rate and 85%
treatment success.
DOTS is the basic strategy employed to realize this goal. The five elements of DOTS
– government commitment and resources; case detection by sputum microscopy;
standardized treatment with directly observed treatment (DOT) for at least the first
two months; regular uninterrupted supply of anti-TB drugs; and standardized
recording and reporting – together constitute the minimum package of 73
interventions necessary for effective tuberculosis control.
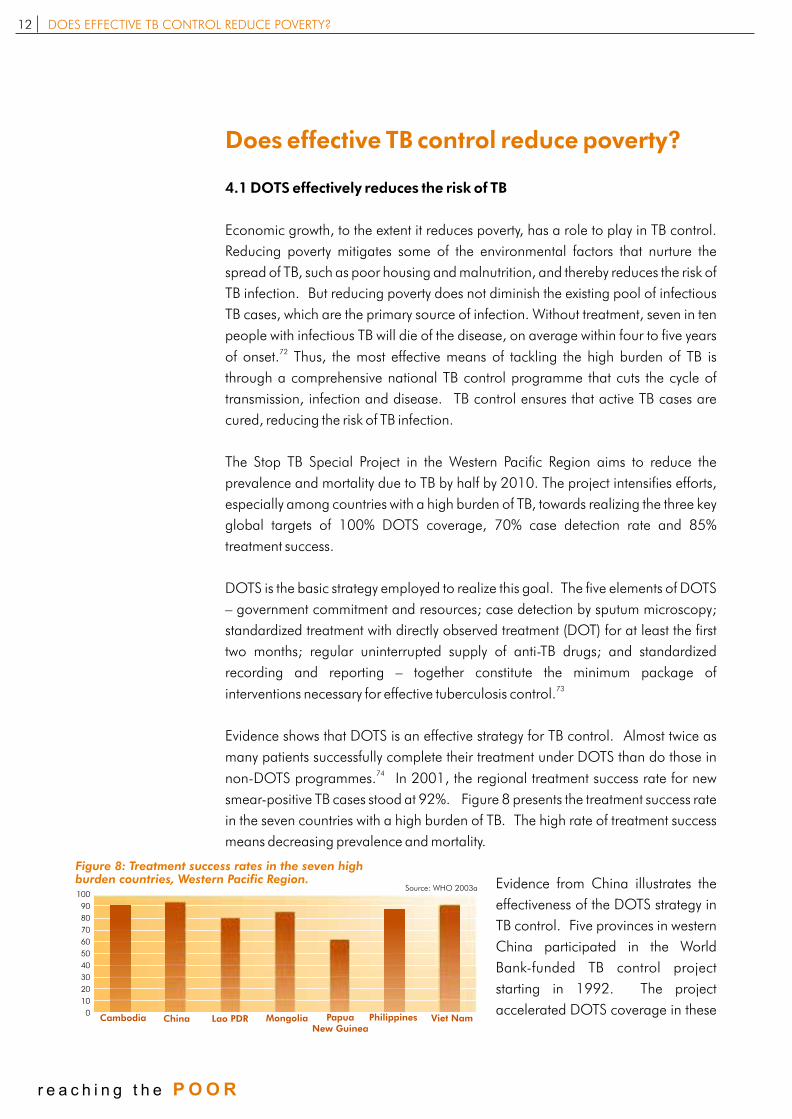
Evidence shows that DOTS is an effective strategy for TB control. Almost twice as
many patients successfully complete their treatment under DOTS than do those in 74
non-DOTS programmes. In 2001, the regional treatment success rate for new
smear-positive TB cases stood at 92%. Figure 8 presents the treatment success rate
in the seven countries with a high burden of TB. The high rate of treatment success
means decreasing prevalence and mortality.
Evidence from China illustrates the
effectiveness of the DOTS strategy in
TB control. Five provinces in western
China participated in the World
Bank-funded TB control project
starting in 1992. The project
accelerated DOTS coverage in these
12 DOES EFFECTIVE TB CONTROL REDUCE POVERTY?
r e a c h i n g t h e P O O R
Cambodia
100
90
80
70
60
50
40
30
20
10
0China Lao PDR Mongolia Papua
New GuineaPhilippines Viet Nam
Source: WHO 2003a
Figure 8: Treatment success rates in the seven high burden countries, Western Pacific Region.
areas. Over a decade, these provinces experienced a 27.2% decrease in the
prevalence of smear-positive pulmonary TB. In comparison, the seven provinces in
western China not covered by the project saw a 7.3% increase in the prevalence of 75
smear-positive pulmonary TB.
4.2 How DOTS contributes to poverty reduction
Since the social and economic costs of TB can be very high, reducing TB may also
reduce poverty indirectly, through longer lives and increased productivity of TB
patients and their families. Moreover, since it provides free diagnosis and treatment,
DOTS is specifically designed to reduce the economic burden of TB. A review of the
literature finds that DOTS is the most cost-effective TB intervention for both the 76,77
provider and the household in low and middle-income countries.
DOTS can also address some of the opportunity costs of seeking TB treatment by
ensuring effective cure and early return to work. In a study in Jakarta, among
patients who were unemployed when treatment was initiated, half were jobless
because of TB symptoms. After two months of weekly DOT, 40% of those
unemployed because of TB were employed and another 20% started working after 78
four months. The successful cure rates and lower cost of treatment under DOTS
can also partly address the social costs of TB, such as stigma.
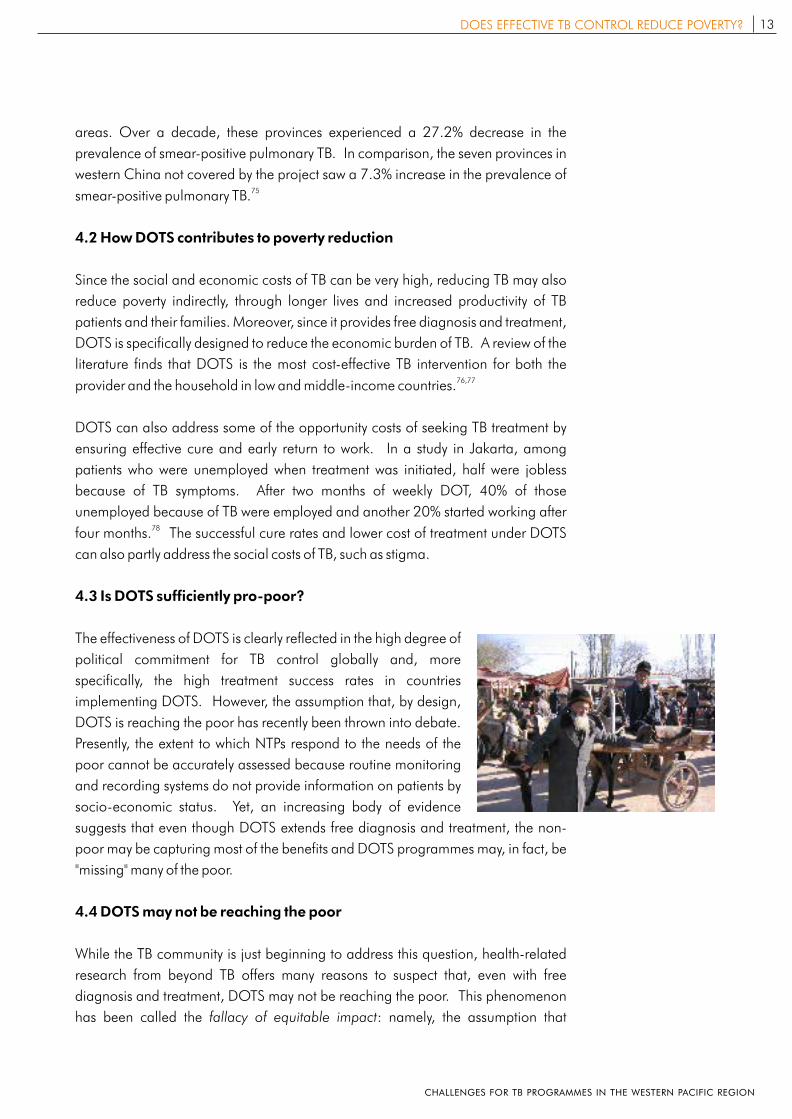
4.3 Is DOTS sufficiently pro-poor?
The effectiveness of DOTS is clearly reflected in the high degree of
political commitment for TB control globally and, more
specifically, the high treatment success rates in countries
implementing DOTS. However, the assumption that, by design,
DOTS is reaching the poor has recently been thrown into debate.
Presently, the extent to which NTPs respond to the needs of the
poor cannot be accurately assessed because routine monitoring
and recording systems do not provide information on patients by
socio-economic status. Yet, an increasing body of evidence
suggests that even though DOTS extends free diagnosis and treatment, the non-
poor may be capturing most of the benefits and DOTS programmes may, in fact, be
"missing" many of the poor.
4.4 DOTS may not be reaching the poor
While the TB community is just beginning to address this question, health-related
research from beyond TB offers many reasons to suspect that, even with free
diagnosis and treatment, DOTS may not be reaching the poor. This phenomenon
has been called the fallacy of equitable impact: namely, the assumption that
13DOES EFFECTIVE TB CONTROL REDUCE POVERTY?
CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION

interventions against conditions that are concentrated primarily among the poor 79can be expected to benefit primarily the poor victims of those conditions.
On TB specifically, two studies from Malawi suggest
that the poor may not be benefiting from DOTS. In
Lilongwe, TB notification rates from a densely
populated planned area, characterized by better socio-
economic status, were compared with those of a
similarly populated unplanned squatter area. The
study concluded that 46% of expected smear positive 80
TB cases were "missing" from the squatter area. A
cross-sectional survey of TB patients showed that 62%
were poor. Although this was a higher proportion of
poor than that seen in the general population, the poor
came from planned areas, indicating that the very poor from unplanned areas were 81not accessing DOTS. Similarly, in northern Brazil, TB notification rates were higher
82among middle socio-economic areas and lower in the more deprived areas.
These studies throw into question the assumption that DOTS is reaching the poor
and suggest rather that the current detection strategy may, in fact, be "missing"
cases, especially in hard-to-reach or marginalized populations.
14 DOES EFFECTIVE TB CONTROL REDUCE POVERTY?
r e a c h i n g t h e P O O R
Why may DOTS be failing
to reach the poor?
Poverty can influence the way
the poor perceive their illness, their
health seeking behaviour, when
and where they access diagnosis
and proper treatment, the quality
of care they receive and whether
they achieve a successful
outcome.
5
r e a c h i n g t h e P O O R CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION
Why may DOTS be failing
to reach the poor?
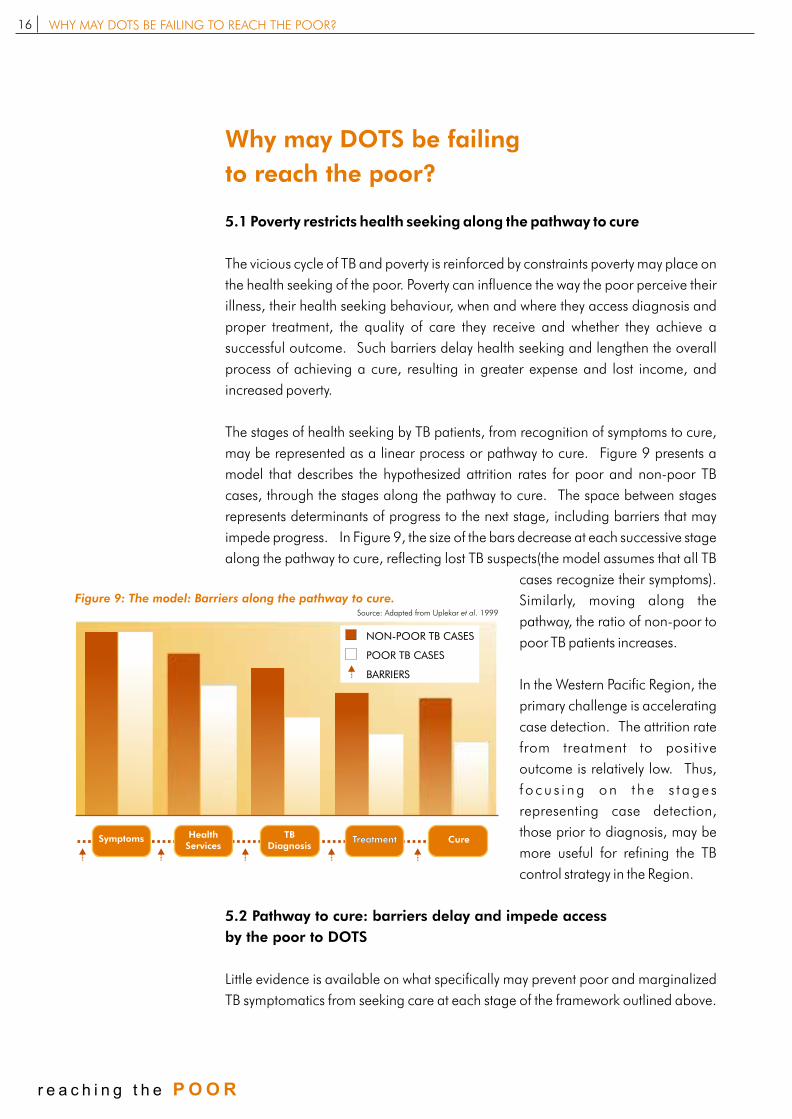
5.1 Poverty restricts health seeking along the pathway to cure
The vicious cycle of TB and poverty is reinforced by constraints poverty may place on
the health seeking of the poor. Poverty can influence the way the poor perceive their
illness, their health seeking behaviour, when and where they access diagnosis and
proper treatment, the quality of care they receive and whether they achieve a
successful outcome. Such barriers delay health seeking and lengthen the overall
process of achieving a cure, resulting in greater expense and lost income, and
increased poverty.
The stages of health seeking by TB patients, from recognition of symptoms to cure,
may be represented as a linear process or pathway to cure. Figure 9 presents a
model that describes the hypothesized attrition rates for poor and non-poor TB
cases, through the stages along the pathway to cure. The space between stages
represents determinants of progress to the next stage, including barriers that may
impede progress. In Figure 9, the size of the bars decrease at each successive stage
along the pathway to cure, reflecting lost TB suspects(the model assumes that all TB
cases recognize their symptoms).
Similarly, moving along the
pathway, the ratio of non-poor to
poor TB patients increases.
In the Western Pacific Region, the
primary challenge is accelerating
case detection. The attrition rate
from treatment to positive
outcome is relatively low. Thus,
f o cu s i ng on t he s t age s
representing case detection,
those prior to diagnosis, may be
more useful for refining the TB
control strategy in the Region.
5.2 Pathway to cure: barriers delay and impede access
by the poor to DOTS
Little evidence is available on what specifically may prevent poor and marginalized
TB symptomatics from seeking care at each stage of the framework outlined above.
16 WHY MAY DOTS BE FAILING TO REACH THE POOR?
Source: Adapted from Uplekar et al. 1999
Figure 9: The model: Barriers along the pathway to cure.
TreatmentSymptoms CureTreatmentTB
DiagnosisHealth
Services
NON-POOR TB CASES
POOR TB CASES
BARRIERS
r e a c h i n g t h e P O O R
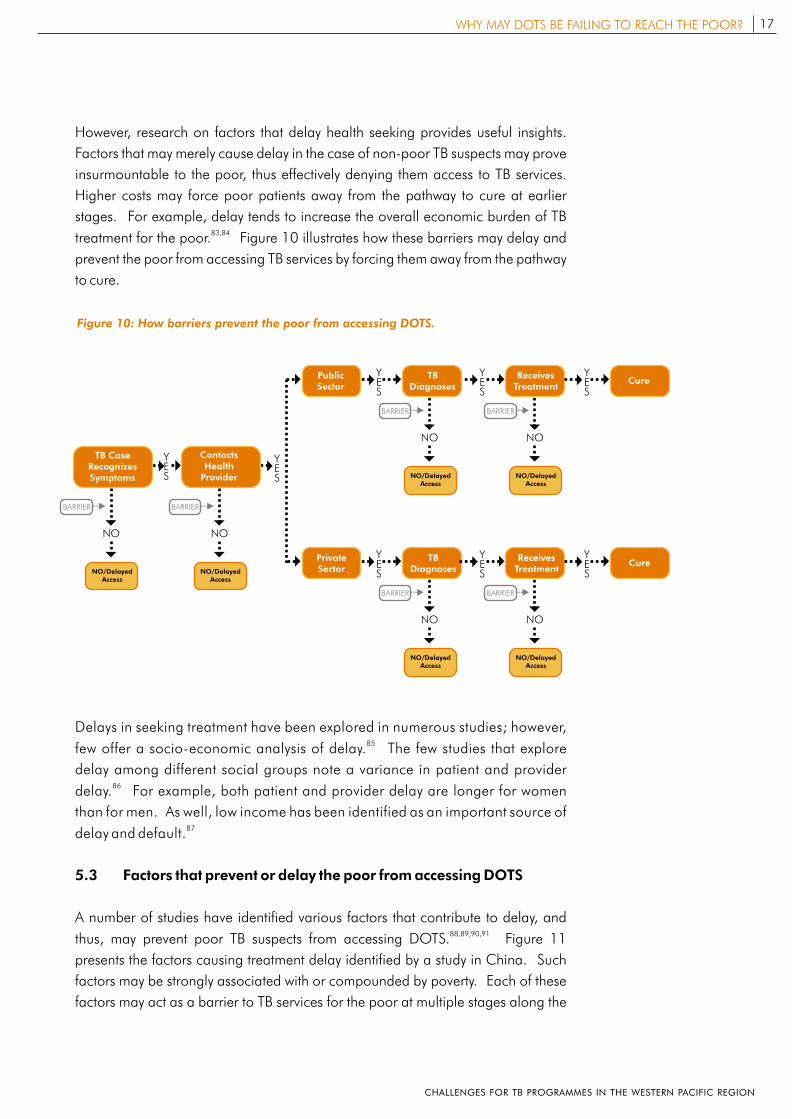
However, research on factors that delay health seeking provides useful insights.
Factors that may merely cause delay in the case of non-poor TB suspects may prove
insurmountable to the poor, thus effectively denying them access to TB services.
Higher costs may force poor patients away from the pathway to cure at earlier
stages. For example, delay tends to increase the overall economic burden of TB 83,84
treatment for the poor. Figure 10 illustrates how these barriers may delay and
prevent the poor from accessing TB services by forcing them away from the pathway
to cure.
Delays in seeking treatment have been explored in numerous studies; however, 85few offer a socio-economic analysis of delay. The few studies that explore
delay among different social groups note a variance in patient and provider 86
delay. For example, both patient and provider delay are longer for women
than for men. As well, low income has been identified as an important source of 87delay and default.
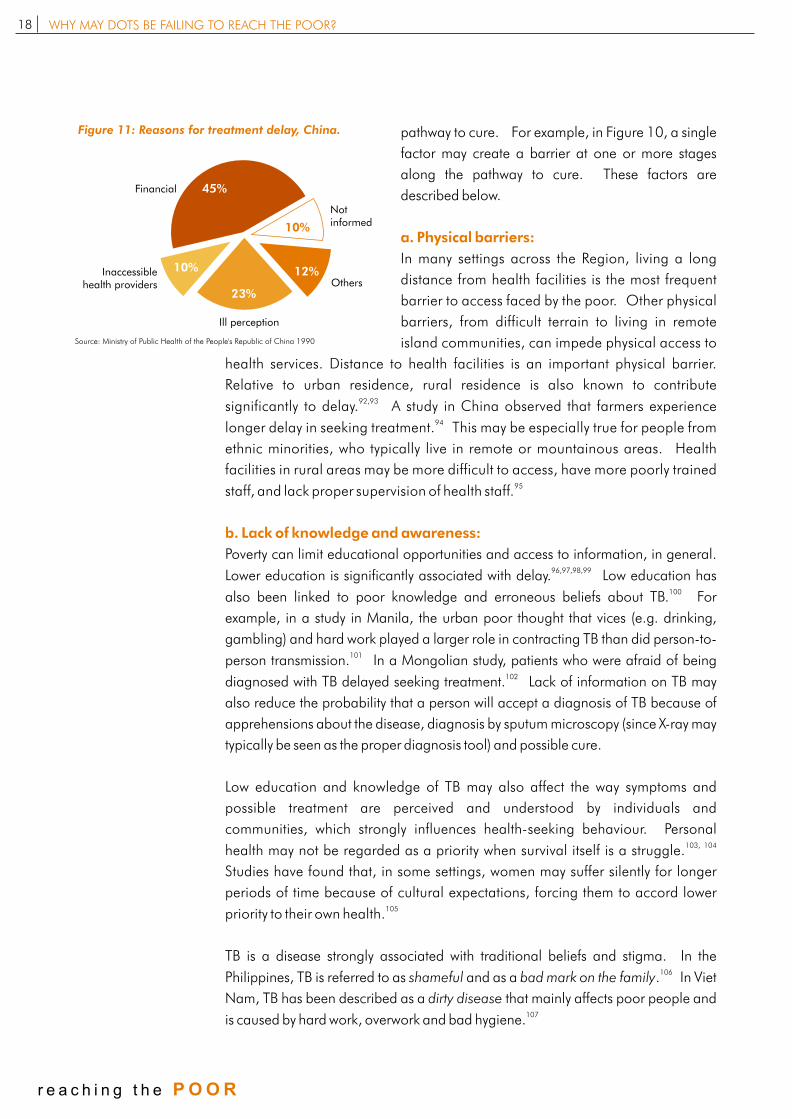
5.3 Factors that prevent or delay the poor from accessing DOTS
A number of studies have identified various factors that contribute to delay, and 88,89,90,91
thus, may prevent poor TB suspects from accessing DOTS. Figure 11
presents the factors causing treatment delay identified by a study in China. Such
factors may be strongly associated with or compounded by poverty. Each of these
factors may act as a barrier to TB services for the poor at multiple stages along the
Figure 10: How barriers prevent the poor from accessing DOTS.
17WHY MAY DOTS BE FAILING TO REACH THE POOR?
YES
YES
NO
NO/Delayed Access
BARRIER
NO
NO/Delayed Access
BARRIER
NO
NO/Delayed Access
BARRIER
NO
NO/Delayed Access
BARRIER
NO
NO/Delayed Access
BARRIER
YES
YES
YES
YES
PrivateSector
TBDiagnoses
ReceivesTreatment
Cure
PublicSector
TBDiagnoses
ReceivesTreatment
Cure
TB Case Recognizes Symptoms
Contacts Health
Provider
NO
NO/Delayed Access
BARRIER
YES
YES
CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION
pathway to cure. For example, in Figure 10, a single
factor may create a barrier at one or more stages
along the pathway to cure. These factors are
described below.
In many settings across the Region, living a long
distance from health facilities is the most frequent
barrier to access faced by the poor. Other physical
barriers, from difficult terrain to living in remote
island communities, can impede physical access to
health services. Distance to health facilities is an important physical barrier.
Relative to urban residence, rural residence is also known to contribute 92,93significantly to delay. A study in China observed that farmers experience
94longer delay in seeking treatment. This may be especially true for people from
ethnic minorities, who typically live in remote or mountainous areas. Health
facilities in rural areas may be more difficult to access, have more poorly trained 95staff, and lack proper supervision of health staff.
Poverty can limit educational opportunities and access to information, in general. 96,97,98,99Lower education is significantly associated with delay. Low education has
100also been linked to poor knowledge and erroneous beliefs about TB. For
example, in a study in Manila, the urban poor thought that vices (e.g. drinking,
gambling) and hard work played a larger role in contracting TB than did person-to-101person transmission. In a Mongolian study, patients who were afraid of being
102diagnosed with TB delayed seeking treatment. Lack of information on TB may
also reduce the probability that a person will accept a diagnosis of TB because of
apprehensions about the disease, diagnosis by sputum microscopy (since X-ray may
typically be seen as the proper diagnosis tool) and possible cure.
Low education and knowledge of TB may also affect the way symptoms and
possible treatment are perceived and understood by individuals and
communities, which strongly influences health-seeking behaviour. Personal 103, 104health may not be regarded as a priority when survival itself is a struggle.
Studies have found that, in some settings, women may suffer silently for longer
periods of time because of cultural expectations, forcing them to accord lower 105priority to their own health.
TB is a disease strongly associated with traditional beliefs and stigma. In the 106
Philippines, TB is referred to as shameful and as a bad mark on the family. In Viet
Nam, TB has been described as a dirty disease that mainly affects poor people and 107is caused by hard work, overwork and bad hygiene.
a. Physical barriers:
b. Lack of knowledge and awareness:
Figure 11: Reasons for treatment delay, China.
Financial
Not informed
Inaccessible health providers Others
Ill perception
10%
45%
23%
12%
10%
Source: Ministry of Public Health of the People's Republic of China 1990
18 WHY MAY DOTS BE FAILING TO REACH THE POOR?
r e a c h i n g t h e P O O R
Studies reveal that stigma is an important factor contributing to delay, as it seems to
weigh strongly on patients' decisions regarding diagnosis and treatment. TB
symptomatics who felt that they would be ostracized because of TB delayed seeking 108treatment longer. Women, especially, may "shop around" for a more appropriate
109diagnosis and treatment. Some studies have found that women may wait up to
twice as long as men before seeking treatment, citing fear of social isolation from 110,111families and community.
Upon diagnosis, TB patients may not accept the diagnosis, or may become 112,113,114
frustrated, disappointed or worried. This negative response to TB diagnosis
may result in their unwillingness to be officially registered as TB cases in health 115facilities. Patients may opt out of treatment or seek treatment from a private
provider because daily visits to the health centre can identify them as TB patients.
This is especially true for women who are more susceptible to stigma and wish to 116,117,118
keep their condition a secret. Importantly, a study in Viet Nam suggests that, 119once diagnosed, patients are likely to revert to a traditional understanding of TB.
Such negative responses to TB may also influence treatment outcomes. Notably,
social support, such as that offered by families, has been positively associated with
health seeking and treatment adherence by studies in the Philippines and 120,121
Singapore.
Although DOTS provides free diagnosis and treatment,
repeated visits to health facilities are required. The cost of
transportation and food, coupled with lost income because
of time away from work, may be more than poor TB patients 122
or families can afford. A study from Malawi estimated
that on average, TB patients spent US$ 13 and lost 22 days 123from work at the diagnosis stage alone. In a study in Viet
Nam, TB patients explained that poverty forced them to choose to work instead of 124
undergoing treatment. Poverty forced patients to default from treatment in
studies from India, Haiti and South Africa, while in other studies, TB patients cite 125,126,127,128,129,130economic constraints as a major factor leading to default. As well,
patients may face additional costs not covered by DOTS. For example, the recent
National TB Programme Review in Viet Nam found that although anti-TB drugs are
provided free of charge, patients were required to purchase the syringes and 131
distilled water for the injection during the intensive phase of treatment.
The opportunity cost of adhering to treatment appears to be different for men and
women. Men are more likely to default because of pressure to return to work,
alcohol and drug addiction. Pressure to do housework and the strain of keeping 132
their condition a secret seems to cause women to default. In other words, women
are pressured by both the economic and social costs of TB while men are more
c. Economic barriers:
19WHY MAY DOTS BE FAILING TO REACH THE POOR?
CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION

concerned with the economic burden. Interestingly, it has been reported that 133
women have higher treatment compliance rates than men.
Even when health services are available, the health system may not effectively
respond to the needs of poor TB patients. Systems-related barriers that patients
from poorer households may face include the (actual or perceived) poor quality of
services, biased or undignified treatment from providers, and higher user fees.
Public sector: In Cambodia, China and Viet Nam, the introduction of user fees in
the public health system has created an environment where formal and informal
public health fees taken together are similar to the amount charged by the private
sector. This has increased inequality between income groups and can deter or 134
delay the use of services. In addition, fees may not be seen to accurately reflect
the perceived value of services. Services provided by public health systems are
often described as involving long travel time, long waits, inconvenient hours, poor
quality of care and inadequate staff with unfriendly attitudes. Poor perception of 135,136,137
health services is strongly associated with delay, particularly for women.
The low regard for TB control services in public health centres is often based on the 138poor reputation of the public health system, in general. The quality of anti-TB
drugs in public health facilities is also often perceived to be poor and patients
anticipate a shortage of drugs and supplies. In India, the health centres'
inconvenient hours forced a rush of patients just after opening time (9:00 a.m.).
The rush prevented providers from offering the one-on-one support that could 139
encourage treatment adherence. General dissatisfaction with the quality of care 140discouraged TB patients in the Philippines from continuing treatment.
Interestingly, one study found that in the Philippines, distrust in successful TB 141
treatment outcomes was higher in people with low incomes.
In particular, TB programmes may fail to respond to the needs of specific groups
because of provider bias. Within the public health system, formal or informal
eligibility criteria may prevent patients from accessing TB services. A study in Viet
Nam found that TB patients must have a fixed address to be eligible for treatment, 142
while those who are not eligible for treatment are referred to private practitioners.
This practice can constitute a real barrier for homeless TB patients. A study from
New Delhi documents the informal selection criteria developed by DOTS providers
targeting patients who were seen to be at risk of treatment default. The criteria 144denied treatment to socially marginalized and vulnerable patients.
Studies from Viet Nam found that it took doctors significantly longer to diagnose 144,145
women with TB than men. This delay may partially be exampled by provider
bias in requesting sputum samples from women. The study in Viet Nam observed
d. Lack of health system responsiveness:
The low regard
for TB control
services in public
health centres is often
based on the poor
reputation of the
public health system,
in general.
20 WHY MAY DOTS BE FAILING TO REACH THE POOR?
r e a c h i n g t h e P O O R
that only 14% of female TB symptomatics reported giving a sputum sample in 146hospital compared with 36% of male TB symptomatics.
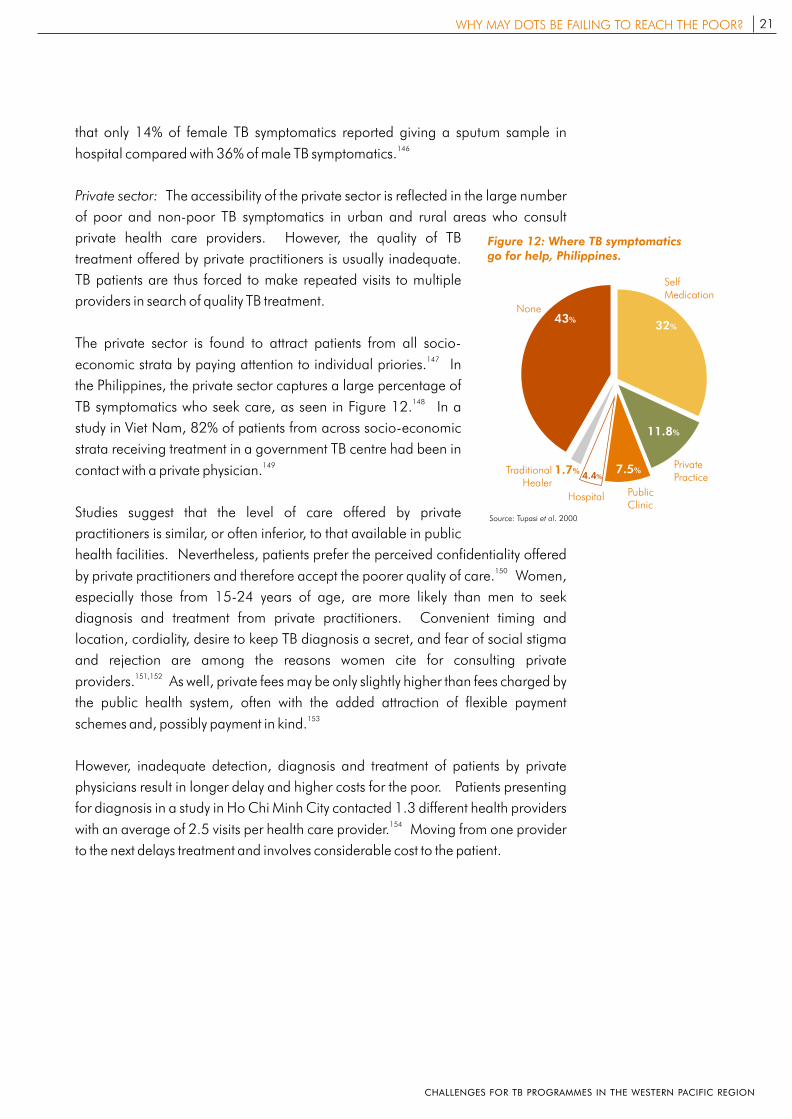
Private sector: The accessibility of the private sector is reflected in the large number
of poor and non-poor TB symptomatics in urban and rural areas who consult
private health care providers. However, the quality of TB
treatment offered by private practitioners is usually inadequate.
TB patients are thus forced to make repeated visits to multiple
providers in search of quality TB treatment.
The private sector is found to attract patients from all socio-147
economic strata by paying attention to individual priories. In
the Philippines, the private sector captures a large percentage of 148TB symptomatics who seek care, as seen in Figure 12. In a
study in Viet Nam, 82% of patients from across socio-economic
strata receiving treatment in a government TB centre had been in 149
contact with a private physician.
Studies suggest that the level of care offered by private
practitioners is similar, or often inferior, to that available in public
health facilities. Nevertheless, patients prefer the perceived confidentiality offered 150by private practitioners and therefore accept the poorer quality of care. Women,
especially those from 15-24 years of age, are more likely than men to seek
diagnosis and treatment from private practitioners. Convenient timing and
location, cordiality, desire to keep TB diagnosis a secret, and fear of social stigma
and rejection are among the reasons women cite for consulting private 151,152providers. As well, private fees may be only slightly higher than fees charged by
the public health system, often with the added attraction of flexible payment 153
schemes and, possibly payment in kind.
However, inadequate detection, diagnosis and treatment of patients by private
physicians result in longer delay and higher costs for the poor. Patients presenting
for diagnosis in a study in Ho Chi Minh City contacted 1.3 different health providers 154with an average of 2.5 visits per health care provider. Moving from one provider
to the next delays treatment and involves considerable cost to the patient.
Figure 12: Where TB symptomatics go for help, Philippines.
11.8%
PrivatePractice
Public Clinic
Hospital
Traditional Healer
None
32%43%
7.5%4.4%
1.7%
Self Medication
Source: Tupasi et al. 2000
21WHY MAY DOTS BE FAILING TO REACH THE POOR?
CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION
How should TB
programmes improve access
for the poor to DOTS?
There are three main reasons
for TB programmes to focus
on increasing access by the poor
to DOTS: efficiency, equity
and human rights.
6
r e a c h i n g t h e P O O R CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION

How should TB programmes improve
access for the poor to DOTS?
6.1. Improving access to meet the TB control targets
In the Western Pacific Region, the percentage of the population with access to
DOTS has increased from 58% in 1998 to 77% in 2002, and 100% coverage by
the end of 2005 is in sight. One major challenge remains: at 44%, the current case
detection rate for new smear-positive TB cases is still far from the 70% target, as
seen in Figure 13.
The analysis in previous sections
shows that, even in countries where
DOTS has reached 100% coverage,
various obstacles may place TB
services beyond the reach of the
poor. There are three main reasons
for TB programmes to focus on
increasing access by the poor to
DOTS. First, coupled with the
disproportionate burden of TB
among the poor, barriers to access have the potential to undermine progress
towards achieving the regional targets. Strategies are thus needed to increase
access to DOTS by the poor. Second, such strategies are also necessary to resolve
inequities in the burden of TB and access to TB control. Third, this will also ensure
that the basic human right to health is enjoyed by all.
There are a number of strategies that can help improve access to DOTS by the poor.
Some of these strategies can be initiated and/or implemented by NTPs; others
require coordination with the larger development community.
6.2 Strategies by the TB programme to improve
access by the poor to DOTS
DOTS is a highly effective strategy for TB control. Thus, the first priority for NTPs is to
ensure the availability of quality TB services by implementing DOTS across the
country. As a next step, TB programmes should focus on improving access for the
poor.
This section presents information on innovative strategies TB practitioners are using
to overcome barriers to access faced by the poor. As a result, evidence is slowly
Figure 13: Case detection rates in high burden countries in the Region, 2002.
Source: WHO 2002
amC
bodia
Cina
h Lo PDR
a
Mongl a
o i
PGN Ph lippines
iViet Nam
WPR
40
60
80
100
0
20
48 48
34
76
16
63
90
44
23HOW SHOULD TB PROGRAMMES IMPROVE ACCESS FOR THE POOR TO DOTS?
CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION
becoming available on how to increase access by poor and marginalized groups to
DOTS. These interventions are still in their early stages and have not yet been
rigorously evaluated or standardized. However, they suggest some ways forward.
Each strategy must be refined based on further analysis and country-specific
situations. Nor is this an exhaustive list of strategies, as the evidence base for pro-
poor strategies needs to be augmented through more systematic operational
research.
! Target investments to improve or to expand TB services to poor or more remote
geographic areas
! Community-based DOTS, which involves building partnerships with community
members and groups
! Innovative outreach strategies in remote and marginalized communities
! Appropriate information, education and communication (IEC) strategies and
material specifically targeting poor, marginalized and vulnerable populations
can effectively increase awareness, reduce misconceptions or stigma, and
motivate health seeking
! NTPs can consider interventions that target low-income or marginalized
populations by tailoring TB services to overcome economic barriers
! NTPs may mobilize financial support for TB patients by building alliances with
communities, nongovernmental organizations (NGOs) and other government
departments
! TB services: Maintaining the quality and responsiveness of DOTS is an
important means of ensuring that all patients receive appropriate care
! Private sector: Public-Private Mix DOTS (PPMD) can effectively ensure that the
poor have access to DOTS, by extending the coverage of DOTS to patients who
seek care in the private sector
! Active case finding: The high prevalence of TB among certain high-risk
populations, such as prisoners or those infected with HIV/AIDS, which are often
marginalized and underserved, may indicate the need for active case finding
! Disaggregated data analysis and operational research: As this paper has
shown, very little evidence currently exists on the extent to which NTPs are able to
respond to the needs of poorer populations. Data should thus be collected and
analysed by indicators of social exclusion, such as sex, income, ethnicity, locality
and employment status. Such analysis enables the appropriate refinement of
TB control strategies. More systematic operational research is also needed to
a. Strategies to address physical barriers:
b. Strategies to address lack of knowledge and awareness:
c. Strategies to address economic barriers:
d. Strategies to address the lack of health system responsiveness:
The first priority for
NTPs is to ensure
the availability of
quality TB services
by implementing
DOTS across the
country. As a next
step, TB programmes
should focus on
improving access for
the poor to DOTS.
24 HOW SHOULD TB PROGRAMMES IMPROVE ACCESS FOR THE POOR TO DOTS?
r e a c h i n g t h e P O O R
identify social, linguistic and other non-financial barriers to access, and to
propose and evaluate strategies to increase the accessibility of DOTS for the
poor.
6.3 Strategies beyond the TB programme
Efforts by the TB programme to address barriers that may
prevent the poor from accessing TB control services can
be further enhanced by a cross-sectoral response to the
non-health determinants of poverty and TB. For
example, by increasing access to education, improving
water and sanitation and enhanced social protection
through insurance schemes targeting the poor, important
progress can be made in reducing poverty. Furthermore,
efforts to make general health services more responsive
to the needs of the poor will strengthen the quality and
responsiveness of DOTS.
6.4 Integrating poverty into TB control: next steps
Recognizing that poor, vulnerable and marginalized populations may have limited
or no access to DOTS, the Stop TB Special Project is developing a Regional TB and
poverty framework. The framework will provide tools to identify the barriers that
prevent the poor from accessing TB services. Strategies to increase the accessibility
of DOTS for the poor will be outlined further. The framework will thus promote a
more systematic response from NTPs. By integrating a pro-poor focus in TB control,
the framework will contribute to reaching the TB control targets by 2005.
25HOW SHOULD TB PROGRAMMES IMPROVE ACCESS FOR THE POOR TO DOTS?
CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION
References
Asian Development Bank. Key Indicators 2003: Education for Global Participation. Manila, Asian Development Bank, 2003.
Ahlburg D. STOP TB Initiative 2000 Report: The Economic Impacts of Tuberculosis. Ministerial Conference. Amsterdam, World Health Organization, 2000.
Auer C. et al. Health seeking and perceived causes of tuberculosis among patients in Manila, Philippines. Tropical Medicine and International Health, 2000, 5(9):648-656.
Barnhoorn F., Adriaanse H. In search of factors responsible for non-compliance among tuberculosis patients in Wardha District, India. Social Science and Medicine, 1992, 34(3): 291-306.
Balasubramanian V., Oommen K., Samuel R. DOT or not? Direct observation of anti-tuberculosis treatment and patient outcomes, Kerala State, India. International Journal of Tuberculosis and Lung Disease, 2000, 4(5):405-413.
Bhushan I. Presentation to Health Systems Development TAG. Manila, World Health Organization, Regional Office for the Western Pacific, 2001 (powerpoint presentation).
Borgdorff M et al. Gender and tuberculosis: a comparison of prevalence surveys with notification data to explore sex differences in case detection. International Journal of Tuberculosis and Lung Disease, 2000, 4(2):123-132.
Chee C. et al. Patient and disease characteristics, and outcome of treatment defaulters from the Singapore TB control unit -- a one-year retrospective survey. International Journal of Tuberculosis and Lung Disease, 2000,4(6):496-503.
Diwan A., Thorson A. Sex, gender and tuberculosis. The Lancet, 1999, 353:1000-1001.
Edginton M., Sekatane C., Goldstein S. Patients' beliefs: do they affect tuberculosis control? A study in a rural district of South Africa. International Journal of Tuberculosis and Lung Disease, 2002, 6(12):1057-1082.
Evans T. et al. Challenging Inequalities in Health: From Ethics to Action. New York, Oxford University Press, 2001.
Farmer, P. et al. Tuberculosis, poverty, and "compliance": lessons from rural Haiti. Seminars in Respiratory Infections, 1991, 6(4):254-60
Fryatt R. Review of published cost-effectiveness studies on tuberculosis treatment programmes. International Journal of Tuberculosis and Lung Disease, 1997, 1(2):101-109.
Godfrey-Faussett P. et al. Why do patients with a cough delay seeking care at Lusaka urban health centres? A health systems research approach. International Journal of Tuberculosis and Lung Disease, 2002, 6(9):796-805.
Government of Mongolia. Economic Growth Support and Poverty Reduction Strategy. Ulaanbaatar, Government of Mongolia, 2003.
Gwatkin D. Reaching the Poor. Presentation to the Asian Development Bank, Manila, 2003 (powerpoint presentation)
26 REFERENCES
r e a c h i n g t h e P O O R
Gwatkin D., Guillot M. The Burden of Disease among the Global Poor: Current Situation, Future Trends, and Implication for Strategy. Washington D.C., World Bank, 2000.
Hanson C. Tuberculosis, poverty and inequality: a review of literature and discussion of issues. Geneva, Stop TB Partnership, World Health Organization, 2002.
Hanson, C. Poverty and TB Control. Presentation to the 2nd TAG Meeting in Beijing, China, World Health Organization, Regional Office for the Western Pacific, 2001 (powerpoint presentation, http://stoptb.wpro.who.int/StopTB_docs/tbandpoverty.ppt).
Holmes C, H. Hausler, et al. A review of sex difference in the epidemiology of tuberculosis. International Journal of Tuberculosis and Lung Disease, 1998, 2(2): 96--104
Huddleson P. Gender differentials in tuberculosis control: the role of socio-economic and cultural factors. The Journal of Tuberculosis and Lung Disease, 1996, 77:391-400.
Islam M. et al. Cost-effectiveness of community health workers in tuberculosis control in Bangladesh. Bulletin of the World Health Organization. 2000, 80(6).
Johansson E. et al. Gender and tuberculosis control: Perspectives on health seeking behaviour among women and men in Vietnam. Health Policy, 2000, 52:33-51.
Johansson E. et al. Attitudes to compliance with tuberculosis treatment among women and men in Vietnam. International Journal of Tuberculosis and Lung Disease, 1999, 3(10): 862-868.
Johansson E. et al. Staff and patient attitudes to tuberculosis and compliance with treatment: an exploratory study in a district in Vietnam. Tuberculosis and Lung Disease, 1996, 77:178-183.
Kamolratankul P. et al. Economic impact of tuberculosis at the household level. International Journal of Tuberculosis and Lung Disease, 1999, 3(7):1-7.
Khan A. et al. Tuberculosis in Pakistan: socio-cultural constraints and opportunities in treatment. Social Science and Medicine, 2000, 50:247-254.
Kingdom of Cambodia. National Poverty Reduction Strategy 2003 - 2004. Phnom Penh, Council for Social Development, Kingdom of Cambodia, 2003.
Knight L. STOP TB Initiative 2000 Report: Tuberculosis and Sustainable Development. Ministerial Conference. Amsterdam, World Health Organization, 2000.
Leon C. et al. Characteristics of the Colombian tuberculosis population (1999-2000), IUATLD Satellite Symposium, poster session and presentations. Montreal, 2002 (unpublished study).
Liefooghe R. et al. A randomised trial of the impact of counselling on treatment of tuberculosis patients in Sialkot, Pakistan. International Journal of Tuberculosis and Lung Disease, 1999, 3(12):1073-1080.
Lienhardt C. et al. Factors affecting time delay to treatment in a tuberculosis control programme in a sub-Saharan African country: the experience of The Gambia. International Journal of Tuberculosis and Lung Disease, 2001, 5(3): 233-239.
Long N., Diwan V., Winkvist A. Difference in symptoms suggesting pulmonary tuberculosis among men and women. Journal of Clinical Epidemiology, 2002, 55(2):115-120.
27REFERENCES
CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION
Long N. et al. Fear and social isolation as consequences of tuberculosis in Viet Nam: a gender analysis. Health Policy, 2001, 58:69-81.
Long N. et al. Longer delays in tuberculosis diagnosis among women in Vietnam. International Journal of Tuberculosis and Lung Disease, 1999a, 3(5):388-393.
Long N. et al. Different tuberculosis in men and women: beliefs from focus groups in Vietnam. Social Science and Medicine, 1999b, 49(6):815-822.
Lonnroth K. et al. Utilisation of private and public health-care providers for tuberculosis symptoms in Ho Chi Minh City, Viet Nam. Health Policy and Planning, 2001a, 16(1):47-54.
Lonnroth K. et al. Can I afford treatment? Perceived consequences of health care provider choices among people with tuberculosis in Ho Chi Minh City, Viet Nam. Social Science and Medicine, 2001b, 52:935-948.
Lui Y., Rao K., Hu S. People's Republic of China: Towards Establishing a Rural Health Protection System. Manila, Asian Development Bank, 2002.
Lui Y., Hsiao W., Eggleston K. Equity in health and health care: the Chinese experience. Social Science and Medicine, 1999, 49(10):1349-1356.
Mann G. et al. Expanding DOTS? Time for cost-effective diagnostic strategies for the poorest in Malawi. IUATLD Satellite Symposium, poster session and presentations. Montreal, 2002 (unpublished study).
Ministry of Health of the People's Republic of China. Report on nationwide random survey for the epidemiology of tuberculosis in 2000. Beijing, Ministry of Health of the People's Republic of China, 2000.
Ministry of Health of the People's Republic of China. Nationwide random survey for the epidemiology of tuberculosis in 1990. Beijing, Ministry of Public Health of the People's Republic of China, 1990.
Nair D., George A., Chacko K. Tuberculosis in Bombay: new insights from poor urban patients. Health and Policy Planning, 1997, 12(1):77-85.
Naranbat N. Description of risk factors for patients and doctors' delay of pulmonary smear positive tuberculosis in Mongolia, 2003 (unpublished document).
Needham D. et al. Socio-economic, gender and health services factors affecting diagnostic delay for tuberculosis patients in urban Zambia. International Journal of Tuberculosis and Lung Disease, 2001, 6(4):256-259.
Nhelma B. et al. A systematic analysis of TB and poverty. Geneva, Stop TB Partnership, World Health Organization, 2003.
O'Boyle S. et al. Factors affecting patient compliance with anti-tuberculosis chemotherapy using the directly observed treatment, short-course strategy (DOTS). International Journal of Tuberculosis and Lung Disease, 2002, 6(4):307-312.
Oxfam GB. Cambodia Land Study Project. Oxfam and the Ministry of Health of Cambodia, 2000.
Patel V., Kleinman A. Poverty and common mental disorders in developing countries. Bulletin of the World Health Organization, 2003, 81(8).
28
r e a c h i n g t h e P O O R
REFERENCES
Piot M. A simulation model of case finding and treatment in tuberculosis control programmes. Geneva, World Health Organization, 1967.
Portero, J., Rubio M. Private Practitioners and tuberculosis control in the Philippines: Strangers when they meet? International Journal of Tuberculosis and Lung Disease, 2003, 8(4):329-335.
Portero J., Rubio M., Pasicatan M. Socio-economic determinants of knowledge and attitudes about tuberculosis among the general population of Metro Manila, Philippines. International Journal of Tuberculosis and Lung Disease, 2002, 6(4):301-306.
Rajeswari R., et al. Socio-economic impact of tuberculosis on patients and families in India. International Journal of Tuberculosis and Lung Disease, 1999, 3(10):869-877
Reynolds K ed. A human rights approach to tuberculosis. Geneva, Stop TB Partnership Secretariat. World Health Organization, 2001.
Singh V et al. TB control, poverty, and vulnerability in Delhi, India. Tropical Medicine and International Health, 2002,7(8):693-700.
Thorson A. et al. Do women with tuberculosis have a lower likelihood of getting diagnosed? Prevalence and case detection of sputum smear positive pulmonary TB, a population based study from Vietnam. Journal of Clinical Epidemiology, 2003 (accepted).
Thorson A., Hoa N., Long N. Health-seeking behaviour of individuals with cough of more than 3 weeks. The Lancet, 2000, 356:1823-1824.
Tupasi T. et al. Bacillary disease and health seeking behaviour among Filipinos with symptoms of tuberculosis: implications for control. International Journal of Tuberculosis and Lung Disease, 2000a, 4(12):1126-1132.
Tupasi T. et al. Tuberculosis in the urban poor settlements in the Philippines. International Journal of Tuberculosis and Lung Disease, 2000b, 4(1):4-11.
United Nations Development Programme. Millennium Development Goals: A compact among nations to end human poverty. Human Development Report, 2003. New York, United Nations Development Programme, 2003.
Uplekar M. et al. Attention to gender issues in tuberculosis control. International Journal of Tuberculosis and Lung Disease, 2001, 5(3):220-224.
Uplekar M., Rangan S., Ogden J. Gender and Tuberculosis Control: Towards a Strategy for Research and Action. Draft strategy paper prepared for Communicable Disease Prevention, Control and Eradication, World Health Organization, 1999 (http://www.who.int/gtb/publications/Gender/Gender_paper.doc).
Uplekar M., Juvekar S., Morankar S. Tuberculosis patients and practitioners in private clinics. Bombay, The Foundation for Research in Community Health, 1996.
Vassal A. et al. Cost-effectiveness of different treatment strategies for tuberculosis in Egypt and Syria. International Journal of Tuberculosis and Lung Disease, 2002, 6(12):1083-1090.
Viet Nam National TB Programme Review, August 2003 (draft report).
Wandwalo E., Morkve O. Delay in tuberculosis case-finding and treatment in Mawanza, Tanzania. International Journal of Tuberculosis and Lung Disease, 2000, 4(2):133-138.
29REFERENCES
CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION

Wilkinson R., et al. Influence of vitamin D deficiency and vitamin D receptor polymorphisms on tuberculosis among Gujarati Asians in west London: a case-control study. The Lance, 2000, 355: 618-621
World Bank. World Development Report 2003: Sustainable Development in a Dynamic World. Washington D.C., World Bank, 2003
World Bank. World Development Report 2000/2001: Attacking poverty. Washington D.C., World Bank, 2001.
World Bank. World Development Report 1993: Investing in Health. Washington D.C., World Bank, 1993.
World Health Organization. Tuberculosis Control: In the WHO Western Pacific Region 2003 Report. Geneva, World Health Organization, 2003a.
World Health Organization. Community Contribution to TB Care: Practice and Policy. Geneva, World Health Organization, 2003b.
World Health Organization. Global Tuberculosis Control: Surveillance, Planning, Financing. WHO Report 2003. Geneva, World Health Organization, 2003c.
World Health Organization. Preliminary surveillance data. Manila, Stop TB Unit, Regional Office of the Western Pacific, 2003d (unpublished).
World Health Organization. An Expanded DOTS Framework for Effective Tuberculosis Control. Geneva, World Health Organization, 2002.
World Health Organization. Pro-poor Health Policies: The Challenges of Reaching the Poor. Draft Background Reading. Workshop on Evidence for Health Policy: Health and Poverty. Geneva, World Health Organization, 2002 (unpublished document).
World Health Organization. Global Tuberculosis Control. Geneva, World Health Organization, 2001a.
World Health Organization. The Global Plan to Stop Tuberculosis. Geneva, World Health Organization, 2001b.
World Health Organization. Macroeconomics and Health: Investing in Health for Economic Development. Report of the Commission on Macroeconomics and Health, 2001c.
World Health Organization. Gender and Tuberculosis. Gender and Health. Geneva, World Health Organization, 2001d
World Health Organization and World Bank. Dying for Change: Poor people's experience of health and ill health. Geneva, World Health Organization, 2001.
World Health Organization. Regional Strategic Plan to Stop TB in the Western Pacific. World Health Organization, Western Pacific Regional Office, 2000.
Xu Biao et al. Does Tuberculosis care reach the poor? A study of TB control programmes in two counties in rural China, 2003 (unpublished).
30
r e a c h i n g t h e P O O R
REFERENCES
Endnotes
1 World Bank 20012 WHO and World Bank 2001 3 Although it is challenging to create a comprehensive measure of poverty, the Human Development Index
(HDI), developed by the United Nations Development Programme (UNDP), is an example of a concerted move forward. The HDI is grounded in the belief that poverty restricts people's freedom. Increasing freedom means ensuring people have the capacity to make decisions. The most basic human capabilities are good health, knowledge and access to resources. The HDI captures these elements by measuring three variables: life expectancy, educational attainment and income.
4 UNDP 20035 World Bank 2003. The World Bank defines extreme poverty as US$ 1 a day, which is seen to be the
minimum amount necessary for survival. Such income measures of poverty allow comparison between regions and countries. To calculate extreme poverty in a country, the dollar-a-day measure is converted to local currency using the purchasing power parity (PPP) exchange rate. The PPP is based on the relative prices of consumption goods in each country.
6 UNDP 2003; Used by the World Bank, East Asia and the Pacific includes the following countries: Cambodia, China, Fiji, Indonesia, Kiribati, Korea, Republic of, Lao People's Democratic Republic, Malaysia, Marshall Islands, Micronesia, Federated States of, Mongolia, Myanmar, Palau, Papua New Guinea, Philippines, Samoa, Solomon Islands, Thailand, Timor-Leste, Tonga, Vanuatu, and Viet Nam
7 Gwatkin, Guillot 2000. To calculate the burden of disease on the global poor, Gwatkin, Guillot disaggregate deaths from all causes into three principal disease groups: 1. communicable diseases, maternal and perinatal conditions, and nutritional deficiencies; 2. non-communicable diseases; and 3. accidents and injures. However, for ease of expression, the authors refer to group 1 conditions as communicable diseases. The discussion in this section follows their terminology.
8 Gwatkin, Guillot 2000. 9 Evans et al. 200110 Patel, Kleinman 200311 Evans et al. 200112 WHO 2001c13 WHO 2002 (unpublished)14 World Bank 200315 World Bank 200316 WHO 2001b17 Gross National Income (GNI) differs from Gross National Product (GDP) in that it also includes a terms of
trade adjustment (http://www.worldbank.org/data/changinterm.html)18 Lower-middle-income countries have a GNI of $736 - $2,935. Considering a more comprehensive
measure of poverty, the HDIs of the high burden countries rank low among countries that have achieved middle human development; UNDP 2003
19 Tupasi et al. 2000a. The prevalence rate of smear+ TB among urban poor and non-poor urban communities presented in Figure 5 are based on extrapolations from the observed population to the general population assuming the bacillary dieses is unlikely to occur in those younger than 10 years.
20 Ministry of Health of China 200021 Xu et al. 200322 Thorson et al. 2003. Thorson et al. explain that 60% of male TB patients and 67% of female patients were
from the lowest income quintile. In contrast, 18% of men and 22% of women in the general study population were from the lowest quintile.
23 Nair et al. 199724 Tupasi et al. 2000b25 Rieder 1999, in Hanson 200226 Dallman 198727 Wilkinson et al. 200028 World Bank 199329 WHO 2001b30 WHO 2003a. In most countries, the male to female ratio of new sputum smear-positive cases is roughly
2:1 (WHO 2003c).31 See, for example, Borgdorff et al. 200032 See, for example, Huddleson 1996 and Uplekar et al. 199933 Holmes et al. 199834 Johansson et al. 2000. Specifically, Huddleson notes that the case fatality rate in women and girls between
the ages of 5 24 years is 27-41% higher than in men35 Uplekar et al. 199936 WHO 2001d37 Viet Nam National TB Programme Review 200338 Thorson, Hoa, Long, 2000. The prevalence of long-term cough was found to be 1% in men and 2% in
women. In another study in Viet Nam, Thorson et al. (2003) report that significantly more female TB cases were detected in a screening survey than in the NTP. The male-female ration in the screening survey was 0.8:1 verses 2.7:1 in the NTP. The authors estimate that the case detection rate among men TB patients is
31ENDNOTES
CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION

39% and a mere 12% for women TB patients.39 Thorson, Hoa, Long, 200040 Thorson, Hoa, Long, (2000) observe that the mean value per health care action was $4.99 for women and
$9.07 for men, with a mean difference of $ 4.07. This is data was colleted in an area where the average monthly income was $11.03.
41 Long et al. 1999b. On average, women experienced a delay of 5.4 weeks, while the delay for men was 3.8 weeks.
42 Long et al. 1999a43 Long et al. 2002 44 Thorson, Hoa, Long, 2000. Thorson notes that sputum exams were only conducted in hospitals and only
for 23% of TB cases45 Long et al. 200246 Long et al. 200247 Ministry of Health of China 200048 Mann et al. 2002 (unpublished)49 Kamolratanakul et al. 199950 Ramachandran et al. 1997 and Saunderson 1995, in Ahlburg 200051 In studies from India and Uganda, up to 80% of wage earners and 95% of subsistence farmers with TB
experienced lower income resulting from decreased productivity and wage earning capacity. See Saunderson 1995, in Ahlburg 2000 and Nair et al. 1997
52 Schwenk, Macallan 2000, in Hanson 2002, explain that TB has been associated with reduced nutritional status including anemia, low plasma concentrations of retinal and zinc, and wasting.
53 Ahlburg 200054 WHO and World Bank 200155 Ahlburg 200056 Kamolratanakul et al. 1999, and Rajasweri et al. 199957 Rajeshwari et al. 1999 58 Nhlema et al. 2003. In Lilongwe, Malawi, girls took on 28% of their mothers activities compared to 3% by
boys (Mann et al. 2002 (unpublished)).59 Oxfam GB 200060 Long et al. 200161 Johansson et al. 200062 Nair et al. 199763 Ministry of Health of China 199064 Viet Nam National TB Programme Review 200365 http://www.who.int/gtb/policyrd/TBPrisons.htm66 Reynolds 200167 WHO 2001b68 Reynolds 200169 Ahlburg 200070 Roughly US$ 37.0071 Portero, Rubio, Pasicatan, 200272 WHO 2001b73 WHO 200074 WHO 2001b75 Ministry of Health of China 200076 Fryatt 199777 Vassall et al. 2002. The World Bank recognises TB control using chemotherapy, as in DOTS, as one of the
most cost-effective public health interventions (World Bank 1993).78 Danusantoso et al. 2002, in Nhlema et al. 200379 Gwatkin 200380 Kemp et al. 2001 (unpublished), in Nhlema et al. 200381 Nhlema et al. 2002 (unpublished), in Nhlema et al. 200382 Souza et al. 2000, in Nhlema et al. 200383 Ahlburg 200084 Karnolratanakul et al. 199985 Nhlema et al. 200386 Nhlema et al. 2003. Total delay, from the onset of the first disease symptom until the patient is diagnosed
and starts treatment, can be broken down into: patient delay (from the onset of symptoms until a qualified medical practitioner is contacted) and provider delay (from the time of first visit to a health practitioner until the patient starts treatment).
87 Johansson et al. 1996, Barnhoorn, Adriaanse 1992, Farmer et al. 1991, in Nhlema et al. 2003, and Edginton 2002
88 Lienhardt et al. 200189 Needham et al. 200190 Wandwalo and Morkve 200091 Lonnroth et al. 2001a92 Lienhardt et al. 200193 Wandwalo, Morkve 200094 Xu et al. 2003 (unpublished)
32 ENDNOTES
r e a c h i n g t h e P O O R
95 Liendhart et al. 200196 Needham et al. 200197 Lienhardt et al. 200198 Wandwalo, Morkve 200099 Naranbat 2003 (unpublished)100 Portero, Rubio, Pasicatan 2002101 Auer et al. 2000. See also Nair et al. 1997 on how TB is perceived by TB patients in Bombay102 Naranbat 2003 (unpublished)103 Dick et al. 1996, in Tupasi et al. 2000a104 Auer et al. 2000105 Uplekar et al. 1999106 Nichter 1994, in Long et al. 2001107 Johansson et al. 1996108 Auer et al. 2000109 Uplekar et al. 1999110 Smith 1994 (unpublished), in Hanson 2002111 Johansson et al. 2000112 Liefooghe et al. 1999113 Johansson et al. 1996114 Khan et al. 2000115 Lonnroth et al. 2001b116 Balasubramanian, Oommen, Samuel 2000117 Uplekar et al. 1999118 Lonnroth et al. 2001a119 Long et al. 1999b and Johansson et al. 2000120 Chee et al. 2000121 Auer et al. 2000122 For example, see Lonnroth et al. 2001b 123 Mann et al. 2003 (unpublished)124 Johansson et al. 1996125 Barnhoorn, Adriaanse 1992126 Farmer et al. 1991127 Edginton, Sekatane, Goldstein 2002128 Khan et al. 2000129 O'Boyle et al. 2002130 Johansson et al. 1996131 Viet Nam National TB Programme Review 2003132 Uplekar et al. 1999133 Uplekar et al. 1999134 For example, Ensor, San 1996, Bloom 1998, and Gertler, Litvack 1998, in Lonnroth et al. 2001a explain
that the introduction of user fees has increased inequity in general access to health care in Viet Nam 135 Godfrey-Faussett et al. 2000136 Long et al. 2001137 Uplekar et al. 1999138 Auer et al. 2000139 Singh et al. 2002140 Auer et al. 2000141 Portero, Rubio, Pasicatan 2002142 Lonnroth et al. 2001a143 Singh et al. 2002144 Thorson, Hoa, Long 2000145 Long et al. 1999b 146 Thorson, Hoa, Long 2000147 Portero, Rubio 2003148 Tupasi et al. 2000a149 Lonnroth et al. 2001a 150 Khan et al. 2000151 Uplekar et al. 1999152 Lonnroth et al. 2001a153 Lonnroth et al. 2001a154 Lonnroth et al. 2001a
33
CHALLENGES FOR TB PROGRAMMES IN THE WESTERN PACIFIC REGION
ENDNOTES


Stop TBWorld Health Organization
Regional Office for the Western PacificUnited Nations Avenue
1000 Manila, Philippines
Tel.: 632 5288001Fax: 632 5211036
Email: [email protected] site: http://stoptb.wpro.who.int
Related Documents











