Cerebral Fat Embolism in ICU Dr.Tarek Sabri Helmi INTENSIVIST Fujairah Hospital UAE 17 October 2016

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Cerebral Fat Embolism in ICU
Dr.Tarek Sabri Helmi
INTENSIVIST
Fujairah Hospital
UAE 17 October 2016

History and Presentation
• 25 –year- old Indian male referred to our hospital from port clinic as he fall in the sea from a ship leader after hitted by heavy object , he remained in water for 45 minutes before they succeeded to pull him.
• On our ER he was drowsy hypothermic , hypotensive and bradycardia ,no head trauma but there was a wound in Lt side of the neck ,fracture Lt femur and both legs , patient resuscitated in ER and reheated then CT trauma done to brain ,chest and abdomen , and x-rays for long bones.
• CT brain was unremarkable , Ct chest revealed bilateral lung contusions and aspiration ,X-rays of long bones revealed comminuted fracture of Lt femur and bilateral fracture of both tibia .











Management
• PATIENT ADMITTED TO ICU on 11/12/15 , he was fully conscious oriented GCS 15/15 , so continued on non invasive ventilation , empirical antibiotics started + ICU care bundle ,conscious sedation given for skeletal traction and external fixation with adequate analgesia , then continued on morphine 4 mg every 4 hours prn for pain , blood transfusion started as HB decreased , patient was stable for 24 hours .
• On 12/12/15 became febrile , suddenly conscious level deteriorated with no hypoxemia , GCS 8/15 without lateralization then developed fits , fits aborted immediately and patient intubated and ventilated , Fat embolism syndrome suspected versus fat embolism with patent foramen oval or dissecting carotid vessels .


Management cont.
• CT brain , chest ,abdomen and neck with angiography done on 14/12/15 , no dissection , normal brain study .
• Transoesophageal Echocardiography don-- revealed intact atrial septum.
• Patient managed as FAT EMBOLISM SYNDROME –(supportive measures + methylprednisolone given 10 mg/kg/8h for 24 h + albumin )

Echocardigraphy (TOE).



Radiology Report
• CT scan done.No fresh changes as compared to old CT scan finding .
• CT Angio neck REVEALED --The arteries from the aortic arch to the carotid arteries up to the cerebral branchs in the brain were traced , no evidence of filling defect of embolisim, nor dissection.
• Head angio CT: REVEALED No evidence of filling defect or cut off at the cerebral arteries and circle of willis.
• No evidence of acute infract or bleed .
• CT chest Angio: REVEALED -Bilateral posterior & basal lung contusions, more on the Lt. side.
• -No evidence of filling defect of pulmonary emblisom at the pulmonary arteries.
• -No evidence of hemo pneumothoax .
• CT ABDOMEN (With i.v. contrast on venous ): REVEALED No free fluid or free air in abdomen,No associated bowel distension ,Normal liver parenchyma and gall-bladder,Normal pancreas, spleen and kidneys.
• Empty urinary bladder, containing foleys, ballon ,No evidence of bony fracture

Complications
Pneumonia MODS

Fractures Fixation
• On 20/12/15 as conscious level not improving on interrupting sedation and MRI was not working so INTERNAL FIXATION don for all fractures in one setting by ORTHOPEDIC TEAM.






MRI REPORT
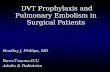
• MRI and MRA brain don on 21/12/15 , revealed On the T2-weighted images, and diffusion DWI show multiple nodular or punctate foci of high signal intensity were found within the brain parenchyma.
• The lesions were located in the white matter (subcortical white matter and centrum semiovale) as well as in the gray matter (basal ganglia and thalami).
• This appearance is highly suggestive of fat embolism syndrome.The rest of the study is normal and unremarkable , MRA --revealed intact cerebral vesseles .--

Complications cont. (pneumonia with sepsis )
• 22/12/15 assessment of conscious level don , Patient was fully conscious , oriented , GCS 14/15 , but with techy cardia du to fever , fever was started on 19/12 , on and off , then become persistent , chest xray revealed pneumonia , so antibiotic changed to tazocine and gentamycin empirically .
• On 23/12/15,patient developed recurrent tonic colonic fits, anti-epileptic started by neurologist (phenytoin)..
• On 24/12/15 fever subsided and patient improved , blood C/S revealed gram negative bacilli , on 25/12/15 revealed as Acinetobacter sensitive to tegicyclin only .
• gentamycin stopped and continued on tazocine plus tegecyclin and blood culture repeated to confirm the results , 2nd blood c/s confirmed Acinetobacter infection , so colistin added , tazocin stopped after 5 days of treatment .


Extubation
• On 26/12/15 Patient was fully conscious , oriented a febrile temp 36.8 , BP 120/68, HR 98 /m regular , SpO2 99% on FiO2 40%, ABG (pH 7.38 , PaO2 120 , PaCO2 38 , HCO3 20 ), patient EXTUBATED without complications .


Complications (Drug eruption)
• on 27/12/15 Patient is fully conscious , oriented a febrile , Stable vitals But he developed Skin rash on both shoulder (pustules acne like ) , discussed with neurologist --plan to withdrawal phenytoin , seen also by dermatologist ,diagnosed drug eruption du to phenytoin .


Discharge from ICU
• ON 28/12/15
• Patient was fully conscious , oriented a febrile temp 36.8 , He is on regular paracetamol 8 hourly PRN for pain , BP 112/64 , HR 94 /m regular , spo2 99% on fio2 28% through nasal cannula , discussed with orthopedist and infection control --planning to shift him to isolated room in the ward ,to continue colistin/tegecyclin to complet 7 days , repeat blood c/s and sputum c/s tomorrow , stop phenytoin , continue on levitracetam 1gm bid and to be to be followed by neurologist

FAT EMBOLISM SYNDROME(FES)

History
• First diagnosed in 1873 by Dr Von Bergmann
• In 1879 Fenger and Salisbury published description of Fat embolism syndrome

Fat Emboli: Fat particles or droplets that travel through the circulation Fat Embolism: A process by which fat emboli passes into the bloodstream and lodges within a blood vessel. Fat Embolism Syndrome (FES): serious manifestation of fat embolism occasionally causes multi system dysfunction, the lungs are always involved and next is
brain

FE vs. FES
• Fat embolization is a well-known complication of skeletal trauma and surgery involving instrumentation of the femoral medullary canal.
• Fat embolism syndrome (FES) is a physiological response to fat within the systemic circulation.
• Fat embolization and FES are not synonymus.
• The embolization of fat can be detected in almost all patients who sustain a pelvic or femoral fracture, but the incidence of FES is less than 1%.

Fat Embolism Syndrome
• Mortality: 10-20%
• Clinical diagnosis, No specific laboratory test is diagnostic.
• Mostly associated with long bone and pelvic fractures, and more frequent in closed fractures.
• Single long bone fracture has 1-3% chance of developing FES, and increases with number of fractures.
• Onset is 24-72 hours from initial insult.

Causes of fat embolism
TRAUMA RELATED: Blunt trauma: Long bone (Femur, tibia, pelvic) factures
orthopedic procedures
Soft tissue injury(chest compression with or without rib fracture)
Burn
Liposuction
Bone marrow harvesting and transplant.

NON TRAUMA RELATED
• Pancreatitis
• Diabetes mellitus
• Osteomyelitis and panniculitis
• Bone tumor lysis
• Steroid therapy
• Sickle cell hemoglobinopathy
• Alcoholic liver disease
• Fat infusion

• Most common cause of FES is blunt trauma.
• 90 % occurs after blunt trauma complicated by long-bone fractures
• Closed fractures had higher incidence compared to open fractures. The intramedullary bone pressure is lower in case of open fractures, which reduces the bulk of fat emboli propelled into the blood stream.

Non-traumatic fat embolism
• It occurs due to the process of fat or marrow necrosis or by the increased concentration of lipids in the blood.
• It may be caused by agglutination of chylomicrons and VLDL by high levels of plasma CRP.
• As in Acute pancreatitis in patients with types I, IV, and V hyperlipidaemia and avascular necrosis of bone in patients with corticosteroid-induced hyperlipidaemia.

Pathophysiology of FES
Exact mechanism unknown, but two main hypothesis
1. Mechanical Hypothesis
2. Biochemical Hypothesis

• Smaller fat droplets travel through the pulmonary capillaries into the systemic
circulation: Embolization to cerebral vessels or renal vessels also leads to central nervous system and renal dysfunction

Biochemical Hypothesis
Toxicity of free fatty acids
• Circulating free fatty acids directly affect the pneumocytes, producing abnormalities in gas exchange.
• Coexisting shock, hypovolemia and sepsis impair liver function and augment toxic effects of free fatty acids.

• Hormonal changes caused by trauma or sepsis induce systemic release of free fatty acids as chylomicrons.
• Acute-phase reactants( C-reactive proteins) cause chylomicrons to
coalesce.
• It explains non traumatic forms of fat embolism syndrome and why symptoms take 12 hours to develop.

FE in ARDS
• Fat emboli obstructs lung vessel (20microns), platelets and fibrin adhere to it
• Lipase increases FFA
• Inflammatory changes->endothelial damage->ARDS

TRAUMA

CLINICAL FEATURES
Asymptomatic for the first 12-48 hours
Pulmonary Dysfunction
Neurological (nonspecific)
Dermatological Signs

Hypoxemia
Neurological abnormalities
Petechial rash

Pulmonary
• Hypoxia, rales, pleural friction rub
• ARDS may develop.
• CXR usually normal early on, later may show ‘snowstorm’ pattern- diffuse bilateral infiltrates
• CT chest: ground glass opacification with interlobular septal thickening.

Neurological findings
• Usually occur after respiratory symptoms
• Incidence- 80% patients with FES
• Minor global dysfunction is most common-ranges from mild delirium to coma.
• Seizures/focal deficits
• Transient and reversible in most cases.
• CT Head: general edema, usually nonspecific
• MRI brain: Low density on T1, and high intensity T2 signal, correlates to degree of impairment.

Dermatological findings • Petechie
• Usually on conjunctiva, neck, axilla, upper limbs.
• Results from occlusion of dermal capillaries by fat globules and then extravasations of RBC.
• Resolves in 5-7 days. Usually fast resolving.
• Pathognomic, but only present in 20-50% of patients.

Other findings
• Retinopathy (exudates, cotton wool spots, hemorrhage)
• Lipiduria
• Fever
• DIC
• Myocardial depression (Right heart strain)
• Thrombocytopenia/Anemia
• Hypocalcemia.

Diagnostic Criteria
• Gurd criteria most commonly used.
Other indexes are
• Schonfeld Index
• Lindeque Index

Gurd & Wilson Criteria

Schonfeld Fat Embolism Syndrome Index
• It ranks signs and symptoms of FES in relation to their incidence of presentation.
• Score >5 required for diagnosis of fat embolism syndrome

Schonfeld FES Index sign score
Petechial rash 5
Diffuse alveolar infiltrate 4
Hypoxemia pao2<70 mm Hg, FIO2-100% 3
confusion 1
Fever ( >100.4 F) 1
Heart rate >120 beats/min 1
Respiratory rate >30/min 1

Lindeque's criteria
• Acc. to Lindeque FES can be diagnosed on the basis of respiratory system involvement alone.

Laboratory Studies
• Arterial Blood Gases (ABGs)
• Urine and sputum examination
• Haemotological Tests
• Biochemical tests

Imaging
• Chest x-ray – shows multiple flocculent shadows (snow storm appearance). picture may be
complicated by infection or pulmonary edema.

Imaging contd.
• MRI Brain
- Image showing minimal hypodense changes in periventricular region, which are more evident in DWI and T2WI as areas of high signals.

Treatment and management
Prophylaxis
• Immobilization and early internal fixation of fracture.
• Fixation within 24 hours has been shown to yield a 5 fold reduction in the incidence of ARDS.
• Continuous pulse oximeter monitoring in high-risk patients may help in detecting desaturation early, allowing early institution of oxygen and possibly steroid therapy.
• High doses of corticosteroids.

Supportive Medical Care
• Maintenance of adequate oxygenation and ventilation
• Maintenance of hemodynamic stability.
• Administration of blood products as clinically indicated.
• Hydration
• Prophylaxis of deep venous thrombosis .
• Nutrition.
Treatment and management contd.

Treatment and management contd.
Oxygenation and ventilation
• High flow rate oxygen is given to maintain the arterial oxygen tension in the normal range.
• Mechanical ventilation and PEEP may be required to maintain arterial oxygenation.

Treatment and management contd.
Hemodynamic stability
• Maintenance of intravascular volume is important, because shock can exacerbate the lung injury caused by FES.
• Albumin has been recommended for volume resuscitation in addition to balanced electrolyte solution, because it not only restores blood volume but also binds with the fatty acids and may decrease extent of lung injury

Steroids
• Steroid prophylaxis is controversial to prevent FES.
• It causes blunting of inflammatory response and complement activation
• Prospective studies suggests prophylactic steroids benefit in high risk patients.
• Preoperative use of methylprednisolone may prevent the occurrence of FES
• Once FES established, steroids have not shown improved outcomes.

Results of Randomized, Controlled Trials of Corticosteroids for Prevention of Fat Embolism Syndrome
Dose Model Timing Duration of study Effect on disease incidence
30mg/kg Dog Before event 60min None
10mg/kg q8h for 24 hrs
Human trauma At admission No data Declining
7.5mg/kg q6h for 12hrs or placebo
Human Trauma Within 12hrs 2 days Declining

Heparin
• Heparin has also been proposed for treatment as it "clears" lipemic plasma in vivo by causing the release of lipoprotein lipase into the circulation, but no evidence exists for its use in FES.

Prognosis
• The fulminant form presents as acute cor pulmonale, respiratory failure or embolic phenomena, leading to death within a few hours of injury.
• Most death contributed to pulmonary dysfunction
• Hard to determine exact mortality rate
• Estimated less than 10%

SUMMARY
• The incidence of FES ranges from < 1 to 29% in different studies.
• Actual incidence of FES is not known
• A high index of suspicion is needed to diagnose FES.
• A combination of clinical criteria and MRI brain will enable early and accurate diagnosis of FES.

THANK YOU
Mansoura- EGYPT


Related Documents