Case Management in Occupational Rehabilitation 1 Running Head: CASE MANAGEMENT IN OCCUPATIONAL REHABILITATION Case Management in Occupational Rehabilitation: Would the Real Case Manager Please Stand Up? Dianna T. Kenny PhD Director, Work and Rehabilitation Research Unit Faculty of Health Sciences The University of Sydney In Australian Journal of Rehabilitation Counselling, 1995, 1, 2, 104-117 Key words: case management, role conflict, occupational rehabilitation Address for correspondence: Dr Dianna Kenny, Department of Behavioural Sciences, Faculty of Health Sciences, The University of Sydney, PO Box 170, Lidcombe, NSW, Australia 2141. Telephone: 61 2 646 6644 Fax: 61 2 646 6540 This research was funded by a grant from the WorkCover Authority of New South Wales, Australia (Grant No 30 303 010)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Case Management in Occupational Rehabilitation 1 Running Head: CASE MANAGEMENT IN OCCUPATIONAL REHABILITATION
Case Management in Occupational Rehabilitation:
Would the Real Case Manager Please Stand Up?
Dianna T. Kenny PhD
Director, Work and Rehabilitation Research Unit
Faculty of Health Sciences
The University of Sydney
In Australian Journal of Rehabilitation Counselling, 1995, 1, 2, 104-117
Key words: case management, role conflict, occupational rehabilitation
Address for correspondence: Dr Dianna Kenny, Department of Behavioural Sciences, Faculty
of Health Sciences, The University of Sydney, PO Box 170, Lidcombe, NSW, Australia 2141.
Telephone: 61 2 646 6644 Fax: 61 2 646 6540
This research was funded by a grant from the WorkCover Authority of New South Wales,
Australia (Grant No 30 303 010)
Case Management in Occupational Rehabilitation 2
Abstract
Key stakeholders (injured workers, rehabilitation co-ordinators, rehabilitation providers,
treating doctors and insurers ) in the occupational rehabilitation process were interviewed to
gain their perspective concerning the degree to which case management was viewed as the
organising principle of post-injury management and to whom this role was most frequently
assigned. Findings indicated that there were differences in stakeholder perceptions about who
should fill this role for the injured worker, with the majority of each group claiming case
management as their proper role. In contrast, 35% of the injured workers interviewed stated
that they either did not have a case manager or that they case managed themselves. Although it
was argued that rehabilitation co-ordinators are suitably placed to act as case managers, they
were nominated least by injured workers. Three vignettes of successful case management were
presented and recommendations for policy and practice were made.
Case Management in Occupational Rehabilitation 3
Case Management in Occupational Rehabilitation:
Would the Real Case Manager Please Stand Up?
Case management of injured workers following workplace injury is viewed as a critical
feature of occupational rehabilitation programs in several countries (Morrison, 1993).The
emergence of case management as a central organising principle in the provision of
rehabilitation services has arisen because of the complex nature of the rehabilitation process
and because of the large number of stakeholders involved with the client throughout the post-
injury phase.
Case management has been defined as "a set of logical steps and a process of interaction
within a service network which assure that a client receives needed services in a supportive,
effective, efficient, and cost-effective manner" (Weil & Karls, 1985, p 2).
The essential elements of case management are "assessment of need, service planning, service
co-ordination and linking, and the monitoring and continuous evaluation of the client, of
service delivery, and of available resources" (Weil & Karls, 1985, p x).
In recent studies assessing the benefits of a case management approach, conflicting results
have been reported. For example, Blum and Mauch (1990) reported benefits of case
management using the rehabilitation nurse in the role of case manager, in the form of cost
reduction, higher return to work rates amongst injured workers and decreased litigation. On the
other hand, Greenwood et al. (1990) found that neither the costs of injury nor the amount of
time lost from work decreased with an early intervention case management approach compared
with routine claims management. However, the quality of the case management was not
assessed in either study, thus making interpretation of the results difficult. Further, little
attention has been paid to the team dynamics in case management, with the result that
stakeholders often have difficulty understanding the roles, responsibilities and perspectives of
other participants. Where disparate and conflicting values exist, such as the basic conflict
Case Management in Occupational Rehabilitation 4 between profit and safety in occupational rehabilitation (Williams & Thorpe, 1992), dilemmas
arise in practice which cannot be resolved at the practitioner-client level. Tarvydas & Cottone
(1991) advocate structural and policy change as the appropriate level of organisational
intervention that would need to be targeted to resolve such dilemmas.
Different countries practise different methods of case management. For example, in the
Netherlands, a team of experts provide joint case management to injured workers. In Germany,
however, the case management function resides in the physician who is responsible for
assessing the needs of injured workers and for arranging rehabilitation if necessary (see for
example, Bockting & Hulsman, 1990; Dean, 1990). In Australia, each state is responsible for
the provision of workers' compensation benefits and rehabilitation to its injured workers. In all
workplaces within the state of New South Wales, for example, employers are required to
establish a workplace rehabilitation program which is developed in consultation between
workers and employers. Part of this program involves the appointment of a rehabilitation co-
ordinator in workplaces which employ more than 20 workers, whose function is to provide
information to the injured worker, liaise with key personnel such as the worker's supervisor and
treating doctor, and to negotiate suitable duties. The rehabilitation co-ordinator may also be
involved in referring to specialist occupational rehabilitation providers (eg, Commonwealth
Rehabilitation Service) for assistance in, for example, workplace modification, development of
upgraded return to work programs or vocational redirection.
Although rehabilitation co-ordinators are in an ideal position to take on the role of case
management for the injured workers in their workplaces, difficulties exist in the rehabilitation
co-ordinator role. Two main reasons have been proposed (Kenny, 1995c). Firstly, there are
currently no requirements within the legislation for the rehabilitation co-ordinator to possess a
set of minimum competencies for the position. Nor are there currently any pre-requisite
qualifications and the person can be selected from among existing staff at the workplace. The
Case Management in Occupational Rehabilitation 5 second difficulty pertains to the conflict of interest which arises for persons occupying this role,
as they are simultaneously employees who owe allegiance to their employers and advocates for
injured workers whose needs do not always coincide with those of their employers. In a series
of studies involving in-depth interviews of injured workers, difficulties with the rehabilitation co-
ordinator were one of the most frequently cited problems (Kenny,1995a; Kenny, 1995b).
Injured workers complained that the rehabilitation co-ordinator was often temperamentally
unsuited to the position, did not understand the requirements of the job, had insufficient
authority within the workplace to serve an advocacy role for the injured worker and was often
unable to implement appropriate workplace modifications. The difficulties identified in the role
of the rehabilitation co-ordinator imply a gap in service provision, in particular, in case
management of injured workers at the worksite.
The aim of this study was threefold: firstly, to describe the current practices of case
management within the post-injury period for injured workers; secondly, to determine which of
the key stakeholders in the rehabilitation process perceived their role as case manager; and
thirdly, to ascertain who was perceived by injured workers to fulfill the role of case manager in
the post-injury period.
Method
Subjects and sampling
Subjects comprised a group of 49 injured workers from the Newcastle/ Hunter regions of New
South Wales, who were drawn from a study population provided by the WorkCover Authority
(see Kenny, 1994, for sampling details), and key stakeholders who operated in the region and
who had employed (n=23 employers) or who had serviced the study group. Either insurance
claims officers or claims managers from each of the major workers' compensation insurers in
the region were interviewed (n=14), as were representatives from each of the accredited
rehabilitation providers (n=19). From the 23 workplaces, 14 rehabilitation co-ordinators were
Case Management in Occupational Rehabilitation 6 interviewed. From a list of 12 treating doctors in the region who had at least 25% of workers'
compensation claimants in their caseloads, nine agreed to be interviewed.
Interview
An in-depth semi-structured interview protocol was developed for all stakeholders, based on
a review of the rehabilitation literature pertaining to the identification of relevant variables which
impact on return to work, on the Workers' Compensation Act (1987) and on policy documents
and brochures for stakeholders developed by the WorkCover Authority of New South Wales.
Only the results of the questions related to case management are reported in this study. The
principal question asked of each of the stakeholders was, "With respect to occupational
rehabilitation, what are your roles and responsibilities as an insurer, a treating doctor, a
rehabilitation co-ordinator, a rehabilitation provider?"
Analysis
Interviews were conducted by the author, a trained research assistant and two contract
interviewers. These same four people also coded the interview transcripts which were tape-
recorded (with permission) and transcribed verbatim for coding and analysis. Thematic
categories, specifically, whether a statement about perceived roles constituted a case
management function, based on the definition and list of essential elements provided by Weil
and Karls (1985), were developed. Inter-rater reliability for assignment of interviewee
statements to thematic categories was assessed at 94% (range 90% to 97%) for five
transcriptscoded independently by each of the four coders (one from each stakeholder group).
Results and Discussion
The role of the insurer
Only two of the 14 insurers interviewed did not perceive case management to be their
primary role. Of the 12 insurers who nominated a case management role, eight identified
multiple roles for themselves, most of which could be subsumed under the case management
Case Management in Occupational Rehabilitation 7 umbrella. For example, one insurer perceived his role to be simultaneously an administrator, a
"watchdog", and a case manager. Other specific roles identified by insurers included supporting
stakeholders, monitoring, and liaising. The need to adopt multiple role functions was
perceived by insurers to arise out of a system which required them to serve multiple clients
simultaneously. These included the WorkCover Authority to whom they are directly
accountable, the employer who pays premiums and the injured worker who has entitlements
under the Act to Workers' Compensation.
Administrative functions included paying wages, processing claims, paying claims and
handling inquiries from injured workers.The support role was identified as "giving assistance to
the employer", "doing whatever we can in assisting the main players in helping to get this person
back to work"; "our role is to support all the other parties involved - employer, injured worker,
rehabilitation provider and doctors."
Insurers were aware that they were in possession of information not readily available to
other parties but which would be of assistance to them. Insurers who identified the role of
communication/liaison as important did so because they perceived that no other conduit
existed. One stated that "insurers get a lot of medical information not generally passed on to the
rehabilitation provider." Another identified the liaison role of insurers as critical, that is, "we
pass on all relevant information between the parties." Monitoring included "monitoring by
medical and vocational evidence the suitability of the plans presented by rehabilitation
providers." Other monitoring functions focused upon the progress of the graded return to work
of the worker, the progress of suitable duties and the outcomes of retraining programs.
Case management was the most frequently identified role. This role was primarily
conceptualised as one of involvement in the identification of those workers who required the
services of a rehabilitation provider, the initiation of those services and subsequently the
provision of guidance and assistance in the rehabilitation process.
Case Management in Occupational Rehabilitation 8 The role of the treating doctor
All doctors identified treatment of the injury as their key function. Seven of the nine treating
doctors interviewed were emphatic about their role as case manager of the injured worker.
They perceived this role to entail a number of functions, including referral to medical
specialists, occupational therapy, physiotherapy, rehabilitation providers and even solicitors.
Doctors took on this role because of their perception that "no-one else would do it." One
doctor expressed his role succinctly - "I am the captain of the ship. It is my job to co-ordinate
the whole show." Below are typical comments from doctors about their perceived role in the
occupational rehabilitation process.
You provide total care . . . you have the role of co-ordinating services. In the country, it is
not as easy to access global rehabilitation services. We have to co-ordinate their seeing a
physiotherapist or an occupational therapist . . . or sending them to an appropriate
specialist.
My primary role is to treat and manage the injury. My second role is case manager and
to assist with the overall approach by all parties, specialists etc, and my third role is to be
patient advocate.
Three doctors commented on the complexity of the rehabilitation system and the variable
quality of services provided. For example, one doctor reported that, "I have to guide my injured
worker clients through the whole confusing system because there are a plethora of
rehabilitation providers out there who are not supplying the goods." Another stated that "There
is an enormous amount of money being wasted on rehabilitation providers . . . the main
problem is that they do not have a sufficient comprehension of the workplace." This comment
notwithstanding, none of the doctors perceived liaison with the workplace as part of the
function of their case manager role. The comment below generally summarises the doctors'
position on this issue.
Case Management in Occupational Rehabilitation 9
I use private occupational therapy firms to liaise between me and the employer, because,
you know, I don't have any direct contact with the workplace. I'll ask the Occupational
Therapist to look at what sort of suitable duties they have. I'm fairly specific in what I want
when I send someone back...I make the decision and supervise the whole thing.
Both of the doctors who did not perceive their role as a case manager identified patient
advocacy as their main function. This entailed "ensuring that the patient's needs were met, for
example, getting an insurer to move on a patient's file;" or "if there is some problem, like the
insurer has rejected an application for physiotherapy, I will ring the insurer and talk to them
about it."
Seven of the nine doctors clearly stated that their principal responsibility was to the patient.
My main role is to relieve pain . . . to get them back to near normal . . . sending them
back to the workforce is important . . . but I don't see myself as having responsibilities
beyond my patient. I forget that they are workers' compensation. They are basically my
patients. The relationship exists and it continues.
The role of the rehabilitation co-ordinator
Unlike other stakeholders, rehabilitation co-ordinators did not use the language of case
management. However, many of the responsibilities cited by the 14 rehabilitation co-ordinators
interviewed included case management functions. Their responsibilities in decreasing order of
frequency (numbers in parentheses), were as follows:
(i) to keep the employer informed about the number of injuries, rehabilitation plans and
progress of cases (7)
(ii) to assess the rehabilitation plan and to organise the services of a rehabilitation provider,
if necessary (7).
(iii) to assist the injured worker to return to work as soon as possible (5).
(iv) to control the costs of injury for the employer (4).
Case Management in Occupational Rehabilitation 10
(v) to advise and educate the injured worker regarding their entitlements under the
legislation (4).
Other responsibilities cited by at least three rehabilitation co-ordinators were to keep their
employers up-to-date on changes to the legislation; to ensure that the worker did not return to
work too early, thereby risking an aggravation of the injury; to show concern and to be the point
of contact for the injured worker.
Rehabilitation co-ordinators were asked an additional question regarding conflict of interest,
as follows: "Do you experience any conflict of interest in meeting your obligations to both your
employer and to the injured worker?"
Six of the fourteen rehabilitation co-ordinators experienced role conflict. The conflicts were
related to budgetary pressures or to management's difficulty in understanding the full
circumstances of a case. Below are some examples.
Everyone is so budget conscious. We are under a managed fund system and we are being
told constantly to keep the cost of individual claims down, so when you are lobbying to get
assistance for the injured worker in the form of a rehabilitation provider or equipment or
aids, which require you to spend more money, it is a conflict.
Sometimes protecting our liability may mean it is detrimental to the employee. Being a
self-insured company puts me too close to the costs of accepting a claim.
Management feel that some rehabilitees are not genuine, and I agree with them. But I
have to take into account both the physical condition and the emotional outlook on the
injury. We had a young bloke who was emotionally upset about a love affair, after having 3
months off for a bad back. It took me a long while, daily, to stop management from
terminating him.
The five rehabilitation co-ordinators who did not experience a conflict of interest cited
management's commitment to occupational rehabilitation as the major reason for harmonious
Case Management in Occupational Rehabilitation 11 relations. Below are some examples. "I am rather lucky . . . I have the respect of both workers
and management. Management give me their full co-operation. And time off for training"; "I
am lucky with this company. They don't pressure you. They let you work honestly."
I don't have conflicts because we are all moving in the same direction. My company is very
responsible and caring about its employees . . . safety is a priority . . . they have more safety
equipment than I have ever seen. They are very aware of their legal responsibilities.
Three of the rehabilitation co-ordinators were ambivalent about their position in the company.
"It's funny . . . I think the supervisors see me as being for the injured workers. The workers see
me as a company man and I see myself in the middle. Neutral."
The role of the rehabilitation provider
Rehabilitation providers are, for the most part, independent practitioners in service delivery
related to rehabilitation of workplace injury. A small proportion of providers are owned and
operated by insurance comapnies. The professions represented include occupational therapists,
physiotherapists, psychologists, vocational counsellors and rehabilitation physicians.
Rehabilitation providers must obtain accreditation from the WorkCover Authority of New
South Wales to practise. They have joint responsibility to insurers, to whom they submit their
plans for payment, to employers, whose workplaces they are servicing, and to the injured
worker, whose rehabilitation they manage.
Up to 1992, 8% of injured workers, on average, were referred to accredited rehabilitation
providers (Kenny, 1994; WorkCover Authority of New South Wales, 1992). However, the
number of claims referred to a rehabilitation provider in the period 1993/1994 rose to 18%
(WorkCover Authority of New South Wales, 1994). In this sample, derived from a study
population taken from the 1991/1992 database, 18.4% workers had been referred to
rehabilitation providers, reflecting the intentional sampling bias towards the more seriously
injured and/or workers with more time lost. Rehabilitation providers answered the question
Case Management in Occupational Rehabilitation 12 only for the subgroup with whom they had contact.
Eleven of the 19 rehabilitation providers interviewed stated that the case management
approach was the central organising principle of management of injured workers. This meant
that one professional from within the organisation was appointed as case manager at the time of
referral and maintained this position with respect to the worker until the case was closed. The
responsibilities cited for this role included initial assessment, development of a rehabilitation
plan, referral and liaison with specialists and other stakeholders, monitoring costs of treatment
and negotiating with the insurer.
It is possible that the remaining nine rehabilitation providers interviewed who did not
explicitly mention case management as the operating principle, assumed the case management
approach as a given, as WorkCover's accreditation system requires that they operate on a case
management principle in order to achieve accreditation. Their responses to the question
implied a case management function. These included monitoring the progress of the injured
worker, assisting the injured worker to be actively involved in his/her own rehabilitation,
maintaining the dignity of the injured worker, and liaising with the workplace, the insurer and
the treating doctor.
Once an injured worker was referred to the rehabilitation provider, providers perceived
themselves to be the case manager for that worker, the central point of contact between the
workplace, the insurer and the treating doctor. Below are some verbatim responses from
providers which highlight their case management philosophy.
Case management in our organisation means referring a case to a designated
professional who is responsible from beginning to end; responsible for arranging
services, for keeping clients informed, for documenting, for monitoring costs and for
liaising with other stakeholders.
Normally the Occupational Therapist would manage the case and do all the liaison with
Case Management in Occupational Rehabilitation 13 other parties such as consultants and referrals. If the employer can't accommodate the person
(ie, provide suitable duties), s/he is then referred across to our rehabilitation counsellor.
Although these comments imply a case management function in relation to other
stakeholders in the system, accreditation guidelines do not require providers to assume such a
function, which may more properly be occupied by the rehabilitation co-ordinator or the
treating doctor at the time of the initial contact with the provider.
Case management from the injured workers' perspective
Injured workers were asked the following question, with probe, "After you were injured, who
was responsible for your case management? Probe: Who advised you about procedures,
treatment and return to work plans?"
The 49 workers interviewed came from 23 workplaces. Each of their employers were also
interviewed and the results of their interview have been reported elsewhere (see Kenny, 1995b).
Of interest in this study was the fact that there were 12 workplaces which employers stated had
a rehabilitation co-ordinator but which injured workers stated either did not have a co-ordinator
or that they did not know whether there was a rehabilitation co-ordinator at the workplace. To
resolve the discrepancy, employers were contacted for clarification. In most cases the problem
arose because the person designated as the rehabilitation co-ordinator was also employed in
some other capacity in the workplace, such as pay clerk, receptionist, "bosses' wife",
occupational health and safety nurse, or personnel officer and was known to the injured worker
only in his/her primary capacity. Further, rehabilitation co-ordinators do not routinely identify
their co-ordinating role to the injured worker. Table 1 summarises injured worker perceptions
of who acted in the capacity of case manager for them during the period of their injury.
Insert Table 1 here
From the table, it can be seen that more than one third (34.7%) of workers believed that none
of the people with whom they had contact post-injury acted in the capacity of case manager. In
Case Management in Occupational Rehabilitation 14 four cases, injured workers stated that they did not need a case manager because the course of
their injury was straightforward and they were able to return to work without such assistance. In
the remaining 13 (26.5%) cases, the injured worker was not contacted by any-one (9) or found
the case management of the person involved to be inadequate, necessitating that they take on
their own case management. One injured worker said, "I did have a rehabilitation provider but
they did not seem to know what they were doing. They put together a return-to-work plan that
had nothing to offer me. In the end, I had to organise things for myself." Another said, "It was
mainly up to me. I did all the ringing up and chasing up. There really is no-one around who will
help you through it."
Seven of the eight workers who were referred to rehabilitation providers identified the
provider as the case manager with the one exception quoted above. This may be the case
because rehabilitation providers use the language of case management and referred workers
were familiar with the terminology. For example, some rehabilitation providers introduce
themselves to the injured worker as "your case manager." The injured workers who identified
the insurer as the case manager were all insured by companies who operated their own
rehabilitation services. Only three workers identified the rehabilitation co-ordinator as the case
manager.
Summary of major findings from the interviews
The majority from each group of stakeholders identified themselves as the most appropriate
group to function in the case management role. In these situations, role confusion arises
whereby each stakeholder may mistakenly believe that other stakeholders are performing
necessary functions or they may vie with each other for case control. This situation leads to
polarisation, competitiveness and conflict between stakeholders and jeopardises a successful
outcome for the client (Kenny, 1995b).
The perception of injured workers was that the case management role was not filled in 35%
Case Management in Occupational Rehabilitation 15 of the sample, and was not adequately filled for half of those (32.7%) who did identify a case
manager. This group felt dissatisfied with at least one aspect of their contact with the nominated
person. The main problematic areas identified were suitable duties, conflict of interest in
service providers resulting in sub-optimal management, and rivalry between stakeholders.
Key issue: Suitable alternative duties
Workers most at risk of post-injury difficulties are those who require suitable alternative
duties, and are hence in most need of a case manager. The provision of suitable alternative
duties may be pivotal in determining the course and outcome of attempts to return to work
(Kenny, 1994), as the following example illustrates.
A severely injured slaughterman in an abattoir, who had lost the use of an arm, described
his experience as follows. He said that the rehabilitation co-ordinator
. . . tried to give me suitable duties, if that's what you call it. They gave me a job looking
after lockers in the work area. Then they got me folding up other blokes' clothing in a
laundry with women. . . . Here I was a leading hand and they got me folding clothes. Every
other bugger who walked past me would say, "Nice to see you working in the women's
quarters, mate." It pissed me off. . . . I walked out because of what I was copping out there.
The provision of inappropriate duties may be likened to employed people working in what
they perceive to be unsatisfactory jobs. Although there is a public perception that "bad" jobs are
preferable to unemployment (Jahoda, 1981), such a view is not supported by the available
evidence. Two recent large scale studies of unemployed young people clearly demonstrated
that those employed in unsatisfactory jobs scored in the same low range on various measures of
mental health as those who were unemployed (O'Brien & Feather, 1990; Winefield,
Tiggemann, Winefield & Goldney, 1993).
Key issue: Conflict of interest
Some workers were unhappy with providers owned by insurers because, "You are put under
Case Management in Occupational Rehabilitation 16 the thumb . . . you do as she (ie, rehabilitation provider) tells you or you go nowhere. But then,
she was under the thumb (of the insurer) and it goes down the line and it is bad."
In cases in which key stakeholders experience conflict of interest, as has occurred with some
of the rehabilitation co-ordinators interviewed in this study and some of the rehabilitation
providers who are owned by insurance companies, optimum service delivery may be
compromised by the constraints which arise in trying to serve two clients.
Key issue: Rehabilitation Co-ordinator as case manager?
When a case manager was identified, the rehabilitation provider was most frequently cited
as the case manager, but for the 92% of injured workers who were not referred to rehabilitation
providers, there was not a systematic process for ensuring that each worker had a case manager.
The finding that many workers were unsure about the existence of a rehabilitation co-ordinator
in their workplaces and that only three workers identified their rehabilitation co-ordinator as
their case manager indicates that incumbents in this role do not currently have a sufficient
profile in their organisations to adequately serve their clients. They, above all other
stakeholders, are in the best position to occupy this role, but currently appear least equipped to
do so.
Case vignettes
Case management perceived by 16 of the workers interviewed to assist in their return to
work are summarised below in three case vignettes demonstrating the different forms that
successful case management currently takes in the Workers' Compensation system.
Case 1: Hans, a 45 year old contract diesel mechanic for a large manufacturing industry
suffered severe muscle and ligament damage to his right arm and shoulder. Following
surgical repair, he was referred by the orthopaedic surgeon to a physiotherapist, who took
on the role of case manager. Hans described his role thus: "He worked out an individual
program and made sure I had mobility in the shoulder and strengthened the muscles. He let

Case Management in Occupational Rehabilitation 17
my GP (ie treating doctor) know what was happening. We decided together when I was
ready to go back to work. ....When I went back to work, my physiotherapist came with me
on the first day. The bosses have to understand that you can't do the same things straight
away. They should be told by some-one else, not the worker, what is wrong and what
treatment you have had and what the restrictions are. I had no problems going back to work
because I still had a place to go back to. The physiotherapist smoothed the way, educated
the bosses. It was a year before I could work as much as I did before. Now I can do
anything."
Case 2: Jill, a 24 year old medical intern in a paediatric ward of a large public hospital
suffered two lumbo-sacral disc herniations. Although there were some difficulties
experienced in her transition back to work, related to the type of work she was offered post-
injury, Jill was fortunate in receiving the appropriate support, both medically and
administratively. She found her rehabilitation co-ordinator to be both "knowledgable and
sympathetic", and her rehabilitation physician "was willing for us both to plan my
rehabilitation and return to work." She was referred to a rehabilitation provider by her
employer (via the rehabilitation co-ordinator) four weeks after her injury, and described her
case manager as . . . "able to give me a lot of direction as to what I was supposed to do. She
(the case manager) talked to the physiotherapist and to the rehabilitation physician and then
worked out a coherent plan. My return to work plan was a joint decision between all the
treating health professionals and me. It worked well because of this and also because I had a
good registrar (immediate superior) who was supportive.
Case 3: Darren, a 26 year old tyre fitter with a large firm, suffered ligament and cartilage
damage to his left knee, which required surgical repair. Although Darren made several
attempts to return to his former position, his injury was aggravated with each return to work
attempt. His employer wanted to terminate him and referred him to a rehabilitation
Case Management in Occupational Rehabilitation 18
provider for retraining. Darren described his experience with the provider: "We put our
heads together and discussed what I'd like to do. They told me what was possible and what
wasn't. I settled on a business operations course at Tech . . . Then I went on the JobCover
Scheme1, which the provider organised for me and now I am an Assistant Manager of a
(different) tyre company."
Each of the three successful cases presented above demonstrates how effective a case
management approach can be if appropriately applied. In the first case, the worker was
fortunate to have been referred to a private physiotherapist who was willing to assume a case
management function, to the point of accompanying the worker to his workplace on his first
day back at work after his injury. This action was, in the opinion of the worker, pivotal to his
smooth transition back to work. The second case demonstrates the ideal functioning of the
team approach to case management, where a number of stakeholders move in and out of the
case management role depending on the needs of the client. Adequate information exchange
and sufficient competencies in each of the stakeholders ensured this worker's successful return
to work. The third case, in which referral to a rehabilitation provider was the "last step before
termination", appropriate case management resulted in retraining and re-employment,
preventing the bleaker alternative of long term unemployment for this capable and motivated
worker.
1The JobCover Scheme is an initiative of te WorkCover Authority of New South Wales, designed to provide incentives to employers via premium exemptions for 12 weeks, to employ workers who have bee rehabilitated or retrained for another position following workplace injury/illness.
In the current system of occupational rehabilitation in New South Wales, authority and
responsibility for care of the injured worker is shared by a number of stakeholders, and each
Case Management in Occupational Rehabilitation 19 stakeholder perceived the major function of case management to reside in his/herown
profession. Their differing perceptions raise an interesting question about the definition of case
management for each of the stakeholders interviewed, with each stakeholder implicitly defining
the "case" differently. For example, for the insurer, the "case" is the workers' compensation
claim; for the treating doctor, the "case" is the injury; for the rehabilitation co-ordinator and the
rehabilitation provider, the "case" is the return to work outcome and for the injured worker,
who is the "case", the overriding need is to be treated with care and respect, to be kept informed
and to be involved in treatment and management decisions. In some circumstances, it is
appropriate and necessary that the responsibility for case management shifts throughout the
person's recovery. In the case of Jill, each of the stakeholders case managed their part of the
case to the mutual satisfaction of the both the client and employer. The difficulty which needs
to be addressed in this multiple case manager model is how the system can ensure a smooth
transition in function between stakeholders, and how to reduce the risk of over-servicing the
client and managing the associated costs involved.
Clear policy and practice guidelines and education about these, together with clear
assignment of roles to key stakeholders need to be established for this central role in injury
management.
Case Management in Occupational Rehabilitation 20
References
Blum, A., & Mauch, R. (1990). R.N. case manager can help provide appropriate care, cost
management. Occupational Health and Safety, 59,4,68-69.
Bockting, A., & Hulsman, T. (1990). The link between disability assessment and
rehabilitation: The system in the Netherlands. In M. Berkowitz (Ed.), Forging linkages:
Modifying disability programs to encourage employment (pp 95-120). New York:
Rehabilitation International.
Dean, D. H. (1990). Vocational rehabilitation innovations for disabled persons within the
Federal Republic of Germany. In M. Berkowitz (Ed.). Forging linkages: Modifying disability
benefit programs to encourage employment (pp 43-66). New York: Rehabilitation
International.
Greenwood, J.G., Wolf, H.J., Pearson, J.C., Woon, C.L., Posey, P., & Main, C.F. (1990).
Early intervention in low back disability among coal miners in west Virginia: Negative findings.
Journal of Occupational Medicine, 32, 1047-1052.
Jahoda, M. (1981). Work, employment and unemployment: Values, theories and
approaches in social research. American Psychologist, 36, 184-191.
Kenny, D. T. (1994). Determinants of time lost from workplace injury: The impact of the
injury, the injured, the industry, the intervention and the insurer. International Journal of
Rehabilitation Research. 17, 333-342.
Kenny, D. T. (1995a). Barriers to Occupational Rehabilitation: An exploratory study of long
term injured workers. Journal of Occupational Health and Safety - Australia and New Zealand,
11, 3, 249-256.
Kenny, D. T. (1995b) Common themes, different perspectives: A systemic analysis of
employer-employee experiences of occupational rehabilitation. Journal of Rehabilitation
Counseling , 39, 1, 54-77.
Case Management in Occupational Rehabilitation 21
Kenny, D. T. (1995c). Occupational rehabilitation in New South Wales. A report to the
WorkCover Authority of New South Wales on the practice of occupational rehabilitation in the
Newcastle, Hunter and Upper Hunter regions. (ISBN 0909353 51 4).
Morrison, M. H. (1993). Rehabilitation and return to work: do other countries succeed?
Work, 3, 48-54.
O'Brien, G. E., & Feather, N.T. (1990). The relative effects of unemployment and quality of
employment on the affect, work values, and personal control of adolescents. Journal of
Occupational Psychology, 63, 151-165.
Tarvydas V.M., & Cottone, R.R. (1991). Ethical responses to legislative, organisational and
economic dynamics: A four level model of ethical practice. Journal of Applied Rehabilitation
Counselling, 22, 4, 11-18.
Weil, M., & Karls, J. M. (1985). Case Management in Human Service Practice. California:
Jossey-Bass Ltd.
Williams, C., & Thorpe, B. (1992). Beyond Industrial Sociology. Sydney: Allen and Unwin.
Winefield, A.H., Tiggemann, M., Winefield, H.R., & Goldney, R.D. (1993). Growing up
with unemployment: A longitudinal study of its psychological impact. London:Routledge.
WorkCover Authority of New South Wales. (1992,1993, 1994). WorkCover Statistics.
Author.
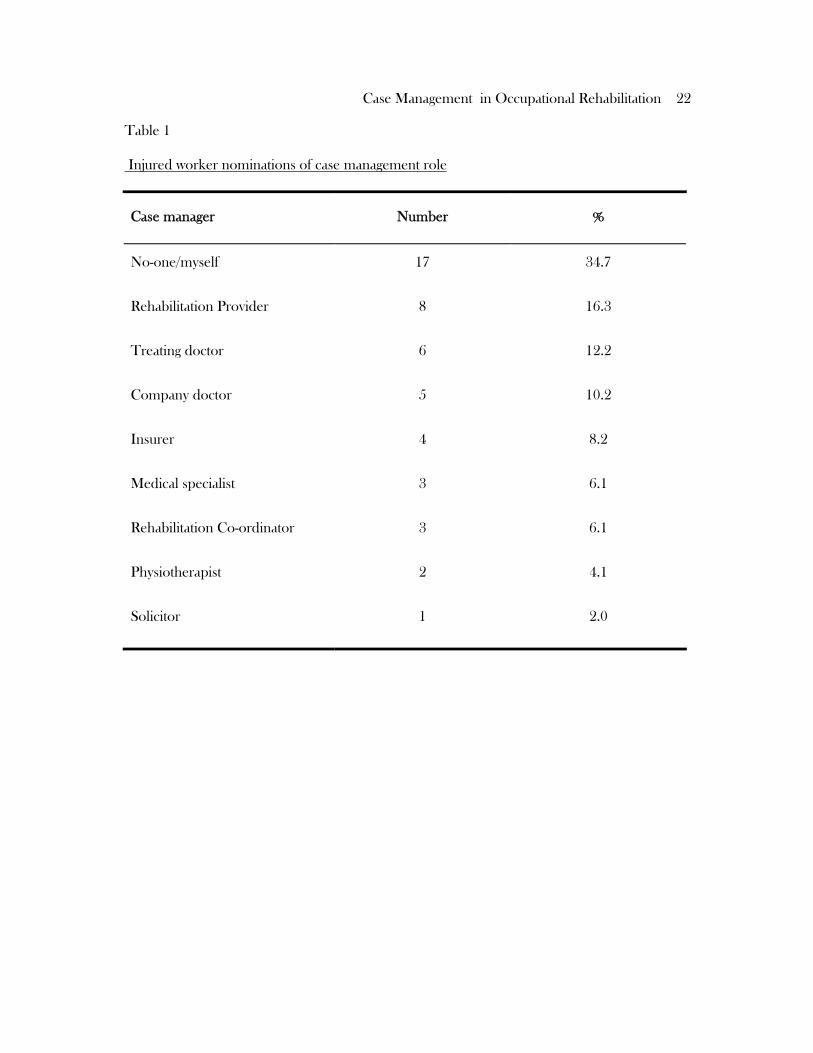
Case Management in Occupational Rehabilitation 22 Table 1
Injured worker nominations of case management role
Case manager
Number
%
No-one/myself
17
34.7
Rehabilitation Provider
8
16.3
Treating doctor
6
12.2
Company doctor
5
10.2
Insurer
4
8.2
Medical specialist
3
6.1
Rehabilitation Co-ordinator
3
6.1
Physiotherapist
2
4.1
Solicitor
1
2.0
Related Documents











