Care Transitions- Easy as Child’s Play –Right? Bronwyn Bartle DNP, CPNP-AC/PC Duke Children’s Heart Center

Care Transitions- Easy as Child’s Play –Right? Bronwyn Bartle DNP, CPNP-AC/PC Duke Children’s Heart Center.
Jan 01, 2016
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Care Transitions-Easy as Child’s Play –Right?
Bronwyn Bartle DNP, CPNP-AC/PCDuke Children’s Heart Center
I do not have any relevant financial relationships with any commercial interests to
disclose.
Disclosure Statement
Do you have a script that drives your care transition from ICU floor
A. Yes
B. No
A few questions to get us started

Do you have a script that drives your care transition from floor to home?
A. Yes
B. No
Question #2

Do you have a “transition of care meeting” with the care team and the family prior to transferring?
A. Yes
B. No
Question #3

Who calls the pediatrician prior to discharge?
A. No one doesB. AttendingC. FellowD. Nurse practitioner
Question #4

Is the family aware of “milestones” to be met prior to transitioning?
A. Yes
B. No
Question #5

Every time we make strides forward we find ourselves sliding backwards.
How can we make it more predictable than a roll of the dice?
Do you ever feel Stuck in this game?
How can we feel less like this? -
We try so hard to “get it right”, always feeling under pressure, hoping at the final hour it does not all blow up
We know we cannot read into
the future – but we have to prepare
for it.
And more like this?
Shift our thinking:Strategic, collaborative,
shared goals,multidisciplinary
What do you use to coordinate care transitions?
A. Journey boardB. Scripted handoffsC. We rely on one person to take care of thisD. No one does thisE. I’m not sure how it happens
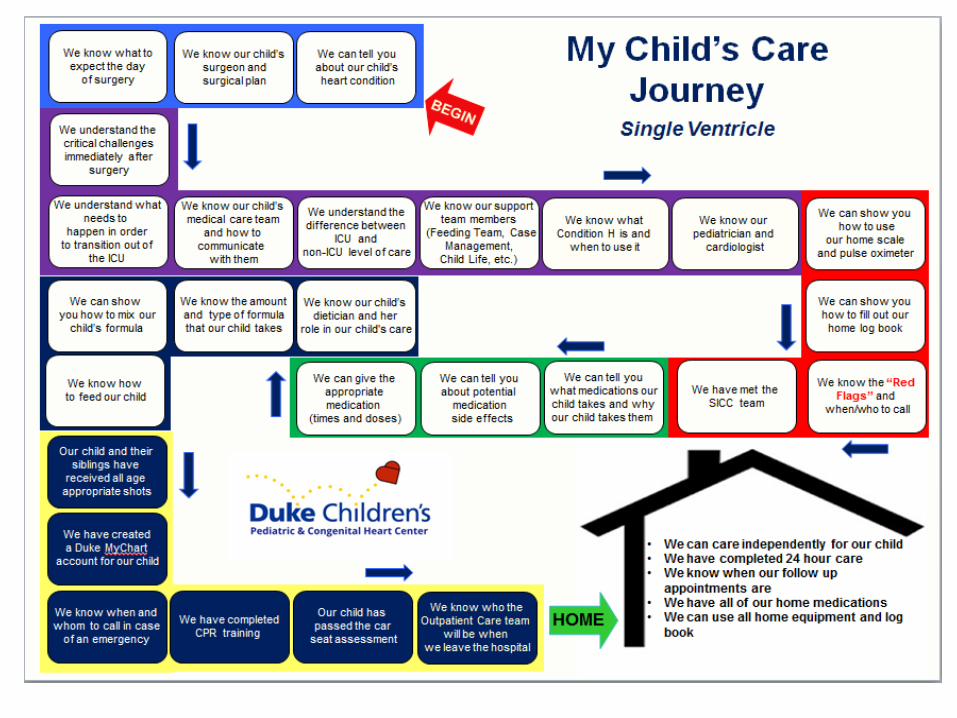
Great idea – but how do we get there?

It’s charted – why the extra step?
Its like story cubes – we all use each of the 6 sided dice to tell the patient’s story.
No one tells the story in quite the same way.
The end user is the reader of the story.

Partner with entire care team- Multidisciplinary
Engage all of your resources (social work, discharge planner, community resources, nursing staff)
Parent/family engagement Critical to success Secondary caregiver identified and trained Teach back method
Transparency of goals
Critical to shift your thinking

Problem list – active and resolved Medications Patient’s current status and most recent
changes Procedures (and results)
Read the op note/cath report/echo yourself Consulted services Family update
Understanding, availability, concerns
What needs to be communicated?
Where do I start??
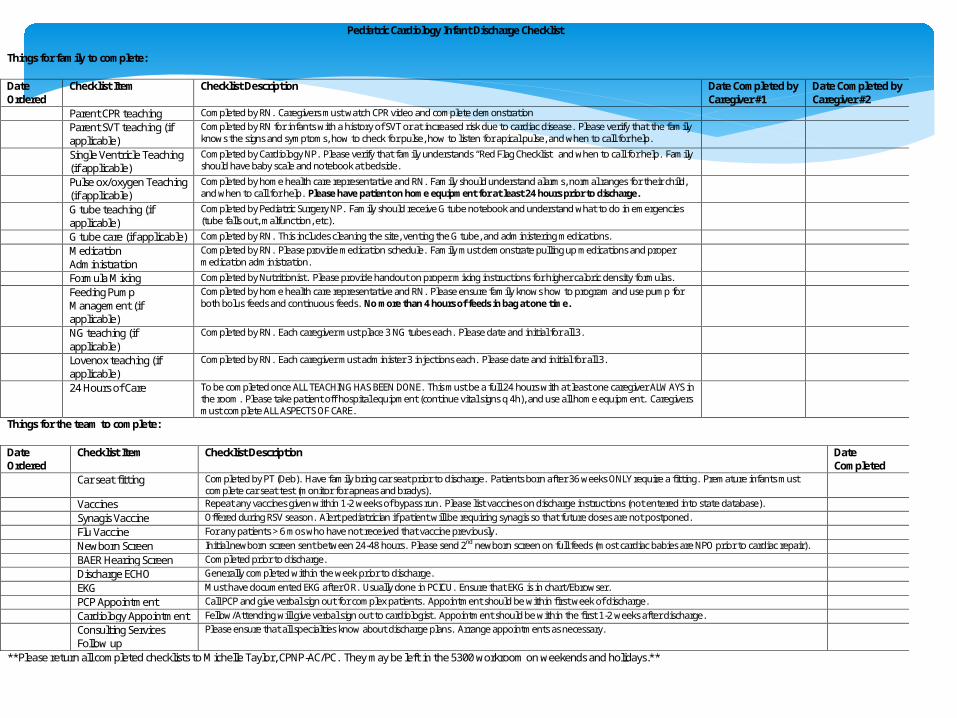
Pediatric Cardiology Infant Discharge Checklist
Things for family to complete:
Date Ordered
Checklist Item Checklist Description Date Completed by Caregiver #1
Date Completed by Caregiver #2
Parent CPR teaching Completed by RN. Caregivers must watch CPR video and complete demonstration Parent SVT teaching (if
applicable) Completed by RN for infants with a history of SVT or at increased risk due to cardiac disease. Please verify that the family knows the signs and symptoms, how to check for pulse, how to listen for apical pulse, and when to call for help.
Single Ventricle Teaching (if applicable)
Completed by Cardiology NP. Please verify that family understands “Red Flag Checklist” and when to call for help. Family should have baby scale and notebook at bedside.
Pulse ox/oxygen Teaching (if applicable)
Completed by home health care representative and RN. Family should understand alarms, normal ranges for their child, and when to call for help. Please have patient on home equipment for at least 24 hours prior to discharge.
G tube teaching (if applicable)
Completed by Pediatric Surgery NP. Family should receive G tube notebook and understand what to do in emergencies (tube falls out, malfunction, etc).
G tube care (if applicable) Completed by RN. This includes cleaning the site, venting the G tube, and administering medications. Medication
Administration Completed by RN. Please provide medication schedule. Family must demonstrate pulling up medications and proper medication administration.
Formula Mixing Completed by Nutritionist. Please provide handout on proper mixing instructions for higher caloric density formulas. Feeding Pump
Management (if applicable)
Completed by home health care representative and RN. Please ensure family knows how to program and use pump for both bolus feeds and continuous feeds. No more than 4 hours of feeds in bag at one time.
NG teaching (if applicable)
Completed by RN. Each caregiver must place 3 NG tubes each. Please date and initial for all 3.
Lovenox teaching (if applicable)
Completed by RN. Each caregiver must administer 3 injections each. Please date and initial for all 3.
24 Hours of Care To be completed once ALL TEACHING HAS BEEN DONE. This must be a full 24 hours with at least one caregiver ALWAYS in the room. Please take patient off hospital equipment (continue vital signs q 4h), and use all home equipment. Caregivers must complete ALL ASPECTS OF CARE.
Things for the team to complete:
Date Ordered
Checklist Item Checklist Description Date Completed
Car seat fitting Completed by PT (Deb). Have family bring car seat prior to discharge. Patients born after 36 weeks ONLY require a fitting. Premature infants must complete car seat test (monitor for apneas and bradys).
Vaccines Repeat any vaccines given within 1-2 weeks of bypass run. Please list vaccines on discharge instructions (not entered into state database). Synagis Vaccine Offered during RSV season. Alert pediatrician if patient will be requiring synagis so that future doses are not postponed. Flu Vaccine For any patients > 6 mos who have not received that vaccine previously. Newborn Screen Initial newborn screen sent between 24-48 hours. Please send 2nd newborn screen on full feeds (most cardiac babies are NPO prior to cardiac repair). BAER Hearing Screen Completed prior to discharge. Discharge ECHO Generally completed within the week prior to discharge. EKG Must have documented EKG after OR. Usually done in PCICU. Ensure that EKG is in chart/Ebrowser. PCP Appointment Call PCP and give verbal sign out for complex patients. Appointment should be within first week of discharge. Cardiology Appointment Fellow/Attending will give verbal sign out to cardiologist. Appointment should be within the first 1-2 weeks after discharge. Consulting Services
Follow up Please ensure that all specialties know about discharge plans. Arrange appointments as necessary.
**Please return all completed checklists to Michelle Taylor, CPNP-AC/PC. They may be left in the 5300 workroom on weekends and holidays.**
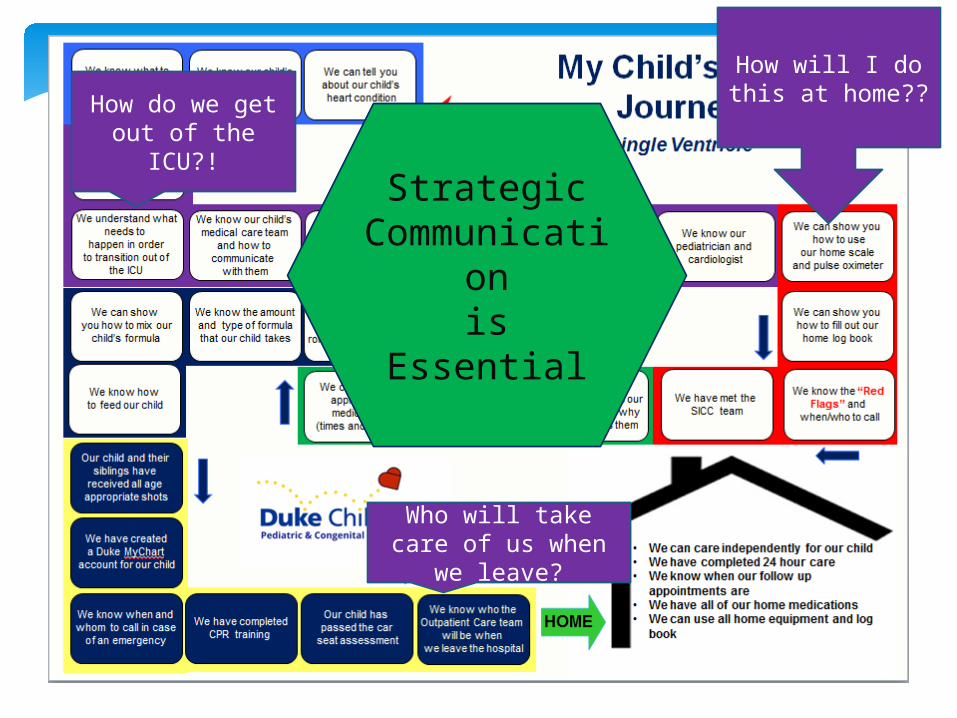
How do we get out of the ICU?!
Who will take care of us when we
leave?
Strategic Communicati
onis Essential
How will I do this at home??
Engages parents even before admission Teach back method builds confidence Listen to how they explain their child to other
family members – a window into their understanding
Satisfies list-makers and slackers alike! Ensures everyone receives the same teaching. Visual reminders Always, always state – AT LEAST 24 hours of care
Overwhelming? I think not…
Reassure them that bumps in the road are to be expected - at EVERY transition point
Hands on practice, practice, practice is essential
Encourage them to ask questions Knowledge is power – be clear in your
communication
For Parents
Don’t be afraid to ask for clarity Don’t accept “I’ve only taken care of them
today” Know what you want to know Ask where the parents are on their journey Face to face bedside hand off is best Transition of care meetings are essential Minimize free text options in charting Know the integral part you play
For team members
Give careful thought to care transitions Be transparent Be sure the story you are writing is not a
cliffhanger! Supply the next caregiver with tools to
succeed – whether that is the next provider or the parent or the pediatrician
The “system” you implement should run without you
Take Home Points
Related Documents








![CARDIOLOGY 101 [Read-Only] - UNC Gillingssph.unc.edu/files/2013/08/nciph-sn14-bartle-cardiology.pdf · CARDIOLOGY 101 Bronwyn Bartle, DNP, ... diastolic timing, increase with valsalva,](https://static.cupdf.com/doc/110x72/5a9e49227f8b9a36788db020/cardiology-101-read-only-unc-101-bronwyn-bartle-dnp-diastolic-timing.jpg)

