ASTHMA Calcium-sensing receptor antagonists abrogate airway hyperresponsiveness and inflammation in allergic asthma Polina L. Yarova, 1 Alecia L. Stewart, 2 * Venkatachalem Sathish, 2 * Rodney D. Britt Jr., 2 * Michael A. Thompson, 2 * Alexander P. P. Lowe, 4 * Michelle Freeman, 2 Bharathi Aravamudan, 2 Hirohito Kita, 3 Sarah C. Brennan, 1 Martin Schepelmann, 1 Thomas Davies, 1 Sun Yung, 1 Zakky Cholisoh, 4 Emma J. Kidd, 4 William R. Ford, 4 Kenneth J. Broadley, 4 Katja Rietdorf, 5 Wenhan Chang, 6 Mohd E. Bin Khayat, 7 Donald T. Ward, 7 Christopher J. Corrigan, 8 Jeremy P. T. Ward, 8 Paul J. Kemp, 1 Christina M. Pabelick, 2 Y. S. Prakash, 2† Daniela Riccardi 1† Airway hyperresponsiveness and inflammation are fundamental hallmarks of allergic asthma that are accompanied by increases in certain polycations, such as eosinophil cationic protein. Levels of these cations in body fluids correlate with asthma severity. We show that polycations and elevated extracellular calcium activate the human recombinant and native calcium-sensing receptor (CaSR), leading to intracellular calcium mobilization, cyclic adenosine monophos- phate breakdown, and p38 mitogen-activated protein kinase phosphorylation in airway smooth muscle (ASM) cells. These effects can be prevented by CaSR antagonists, termed calcilytics. Moreover, asthmatic patients and allergen- sensitized mice expressed more CaSR in ASMs than did their healthy counterparts. Indeed, polycations induced hyper- reactivity in mouse bronchi, and this effect was prevented by calcilytics and absent in mice with CaSR ablation from ASM. Calcilytics also reduced airway hyperresponsiveness and inflammation in allergen-sensitized mice in vivo. These data show that a functional CaSR is up-regulated in asthmatic ASM and targeted by locally produced polycations to induce hyperresponsiveness and inflammation. Thus, calcilytics may represent effective asthma therapeutics. INTRODUCTION Despite substantial advances in our understanding of its pathophys- iology and improved therapeutic regimens, asthma remains a tremen- dous worldwide health care burden with around 300 million individual sufferers. Although the symptoms of asthma are potentially controllable in most asthma sufferers using conventional therapy such as topical bronchodilators and corticosteroids, these are troublesome to adminis- ter efficiently and present unwanted side effects. There remains a signif- icant minority of patients whose symptoms fail to be controlled with these approaches and who face chronically impaired quality of life with increased risk of hospital admission and even death, although in a minority such patients account for the major share of asthma health care costs. Accordingly, there is an urgent unmet need for identification of novel asthma therapies that target the root cause of the disease rather than its clinical sequelae. Asthma is characterized by inflammation-driven exaggeration of airway narrowing in response to specific and nonspecific environmental stimuli [nonspecific airway hyperresponsiveness (AHR)], as well as chronic remodeling of the conducting airways (1). A number of mech- anisms, many driven by inflammation, have been hypothesized to con- tribute to AHR and/or remodeling. Among these, there is increasing recognition that airway inflammation results in augmented local con- centrations of polycations (2–7). The polycations eosinophil cationic protein (ECP) and major basic protein are well-established markers for asthma severity and stability, with some evidence that they may con- tribute directly to the pathogenesis of asthma (6, 8–10). Furthermore, in asthma, increased arginase activity diverts L-arginine toward increased production of the polycations spermine, spermidine, and putrescine (4, 5, 11). Although in human peripheral blood monocytes spermine exhibits anti-inflammatory properties (12), associations between in- creases in polycations in the asthmatic airway mucosa and AHR/airway remodeling and inflammation (4, 5, 13) have long been apparent and ascribed to their positive charge ( 9). However, the cause-effect relationship remains hitherto unexplained. Here, we provide evidence that activation of the cell surface, G protein (heterotrimeric guanine nucleotide–binding protein)–coupled calcium-sensing receptor (CaSR) by polycations drives AHR and inflammation in allergic asthma. The CaSR is the master controller of extracellular free ionized calci- um ion (Ca 2+ o ) concentration via the regulation of parathyroid hor- mone (PTH) secretion (14). Accordingly, CaSR-based therapeutics is used for the treatment of systemic disorders of mineral ion metabolism. Pharmacological activators of the CaSR (calcimimetics) are used to treat hyperparathyroidism, and negative allosteric modulators of the CaSR (calcilytics) are in clinical development for treating autosomal domi- nant hypocalcemia (15). In addition to its pivotal role in divalent cation homeostasis, the CaSR is expressed in tissues not involved in mineral ion metabolism such as the blood vessels, breast, and placenta, where the CaSR regulates many fundamental processes including gene expression, ion channel activity, and cell fate (16). Furthermore, altered CaSR expression has also been associated with several pathological conditions including in- flammation, vascular calcification, and certain cancers (16–19). In these noncalciotropic tissues, the CaSR responds to a range of stimuli including 1 School of Biosciences, Cardiff University, Cardiff CF10 3AX, UK. 2 Department of Anes- thesiology, Mayo Clinic, Rochester, MN 55905, USA. 3 Department of Medicine, Mayo Clinic, Rochester, MN 55905, USA. 4 Division of Pharmacology, Cardiff University, School of Pharmacy and Pharmaceutical Sciences, Cardiff University, Cardiff CF10 3XF, UK. 5 Department of Life, Health and Chemical Sciences, The Open University, Milton Keynes MK7 6AA, UK. 6 Department of Medicine, UCSF School of Medicine, San Francisco, CA 94143, USA. 7 Faculty of Life Sciences, University of Manchester, Manchester M13 9PT, UK. 8 Division of Asthma, Allergy and Lung Biology, King’ s College London, London SE1 9RT, UK. *These authors contributed equally to this work. †Corresponding author. E-mail: [email protected] (D.R.); [email protected] (Y.S.P.) RESEARCH ARTICLE www.ScienceTranslationalMedicine.org 22 April 2015 Vol 7 Issue 284 284ra60 1 CORRECTED 27 APRIL 2015; SEE FULL TEXT by guest on June 5, 2021 http://stm.sciencemag.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
-
R E S EARCH ART I C L E
CORRECTED 27 APRIL 2015; SEE FULL TEXT
ASTHMA
Calcium-sensing receptor antagonists abrogateairway hyperresponsiveness and inflammationin allergic asthmaPolina L. Yarova,1 Alecia L. Stewart,2* Venkatachalem Sathish,2* Rodney D. Britt Jr.,2*Michael A. Thompson,2* Alexander P. P. Lowe,4* Michelle Freeman,2 Bharathi Aravamudan,2
Hirohito Kita,3 Sarah C. Brennan,1 Martin Schepelmann,1 Thomas Davies,1 Sun Yung,1
Zakky Cholisoh,4 Emma J. Kidd,4 William R. Ford,4 Kenneth J. Broadley,4 Katja Rietdorf,5
Wenhan Chang,6 Mohd E. Bin Khayat,7 Donald T. Ward,7 Christopher J. Corrigan,8
Jeremy P. T. Ward,8 Paul J. Kemp,1 Christina M. Pabelick,2 Y. S. Prakash,2† Daniela Riccardi1†
http://stm.
Dow
nloaded from
Airwayhyperresponsiveness and inflammationare fundamental hallmarksof allergic asthma that are accompaniedbyincreases in certain polycations, such as eosinophil cationic protein. Levels of these cations in body fluids correlatewith asthma severity. We show that polycations and elevated extracellular calcium activate the human recombinantandnative calcium-sensing receptor (CaSR), leading to intracellular calciummobilization, cyclic adenosinemonophos-phate breakdown, and p38 mitogen-activated protein kinase phosphorylation in airway smooth muscle (ASM) cells.These effects can be prevented by CaSR antagonists, termed calcilytics. Moreover, asthmatic patients and allergen-sensitized mice expressed more CaSR in ASMs than did their healthy counterparts. Indeed, polycations induced hyper-reactivity inmousebronchi, and this effectwaspreventedby calcilytics andabsent inmicewithCaSR ablation fromASM.Calcilytics also reduced airway hyperresponsiveness and inflammation in allergen-sensitized mice in vivo. These datashow that a functional CaSR is up-regulated in asthmatic ASM and targeted by locally produced polycations to inducehyperresponsiveness and inflammation. Thus, calcilytics may represent effective asthma therapeutics.
sc
by guest on June 5, 2021
iencemag.org/
INTRODUCTION
Despite substantial advances in our understanding of its pathophys-iology and improved therapeutic regimens, asthma remains a tremen-dous worldwide health care burden with around 300 million individualsufferers. Although the symptoms of asthma are potentially controllablein most asthma sufferers using conventional therapy such as topicalbronchodilators and corticosteroids, these are troublesome to adminis-ter efficiently and present unwanted side effects. There remains a signif-icant minority of patients whose symptoms fail to be controlled withthese approaches and who face chronically impaired quality of life withincreased risk of hospital admission and even death, although in aminority such patients account for the major share of asthma healthcare costs. Accordingly, there is an urgent unmet need for identificationof novel asthma therapies that target the root cause of the disease ratherthan its clinical sequelae.
Asthma is characterized by inflammation-driven exaggeration ofairwaynarrowing in response to specific andnonspecific environmentalstimuli [nonspecific airway hyperresponsiveness (AHR)], as well aschronic remodeling of the conducting airways (1). A number of mech-anisms, many driven by inflammation, have been hypothesized to con-tribute to AHR and/or remodeling. Among these, there is increasingrecognition that airway inflammation results in augmented local con-
1School of Biosciences, Cardiff University, Cardiff CF10 3AX, UK. 2Department of Anes-thesiology, Mayo Clinic, Rochester, MN 55905, USA. 3Department of Medicine, MayoClinic, Rochester, MN 55905, USA. 4Division of Pharmacology, Cardiff University, Schoolof Pharmacy and Pharmaceutical Sciences, Cardiff University, Cardiff CF10 3XF, UK.5Department of Life, Health and Chemical Sciences, The Open University, Milton KeynesMK7 6AA, UK. 6Department of Medicine, UCSF School of Medicine, San Francisco, CA 94143,USA. 7Faculty of Life Sciences, University of Manchester, Manchester M13 9PT, UK. 8Division ofAsthma, Allergy and Lung Biology, King’s College London, London SE1 9RT, UK.*These authors contributed equally to this work.†Corresponding author. E-mail: [email protected] (D.R.); [email protected] (Y.S.P.)
www.Scie
centrations of polycations (2–7). The polycations eosinophil cationicprotein (ECP) and major basic protein are well-established markersfor asthma severity and stability, with some evidence that theymay con-tribute directly to the pathogenesis of asthma (6, 8–10). Furthermore, inasthma, increased arginase activity diverts L-arginine toward increasedproduction of the polycations spermine, spermidine, and putrescine(4, 5, 11). Although in human peripheral blood monocytes spermineexhibits anti-inflammatory properties (12), associations between in-creases in polycations in the asthmatic airwaymucosa andAHR/airwayremodeling and inflammation (4, 5, 13) have long been apparent andascribed to their positive charge (9). However, the cause-effect relationshipremains hitherto unexplained.Here, we provide evidence that activation ofthe cell surface, G protein (heterotrimeric guanine nucleotide–bindingprotein)–coupled calcium-sensing receptor (CaSR) by polycations drivesAHR and inflammation in allergic asthma.
The CaSR is the master controller of extracellular free ionized calci-um ion (Ca2+o) concentration via the regulation of parathyroid hor-mone (PTH) secretion (14). Accordingly, CaSR-based therapeutics isused for the treatment of systemic disorders of mineral ionmetabolism.Pharmacological activators of theCaSR (calcimimetics) are used to treathyperparathyroidism, and negative allosteric modulators of the CaSR(calcilytics) are in clinical development for treating autosomal domi-nant hypocalcemia (15).
In addition to its pivotal role in divalent cation homeostasis, theCaSR is expressed in tissues not involved in mineral ion metabolismsuch as the blood vessels, breast, and placenta, where the CaSR regulatesmany fundamental processes including gene expression, ion channelactivity, and cell fate (16). Furthermore, altered CaSR expression hasalso been associated with several pathological conditions including in-flammation, vascular calcification, and certain cancers (16–19). In thesenoncalciotropic tissues, theCaSR responds to a range of stimuli including
nceTranslationalMedicine.org 22 April 2015 Vol 7 Issue 284 284ra60 1
http://stm.sciencemag.org/content/7/284/284ra60.fullhttp://stm.sciencemag.org/
-
R E S EARCH ART I C L E
CORRECTED 27 APRIL 2015; SEE FULL TEXT by guest on June 5, 2021
http://stm.sciencem
ag.org/D
ownloaded from
not only Ca2+o but also polyvalent cations,aminoacids, ionic strength, andpH,makingthis receptor uniquely capable of integratingmultiple environmental signals. Owing toits ability to act as a multimodal chemo-sensor, the potential relevance of CaSRto asthma pathophysiology is manifold,yet there is currently no evidence regard-ing CaSR expression or function in asth-ma. In this regard, a fundamental aspectof asthma pathophysiology is elevatedintracellular calcium ion concentration([Ca2+]i) in airway smooth muscle (ASM)cells that is not only critical to the enhancedbronchoconstriction of nonspecific AHRbut also implicated in longer-term, likelygenomic effects that result in airway re-modeling such as increased ASM cellproliferation (leading to airwaywall thick-ening) and deposition of extracellularmatrix components (20, 21). There is cur-rently no information as to whether theCaSR can regulate [Ca2+]i in the asthmaticairways, even though a polycation sensorsuch as the CaSR, whose activation leadsto an increase in [Ca2+]i, seems a likely can-didate. Therefore, we hypothesized thatif a CaSR was to be found in the airways,it would sense and respond not only toinflammation-enhanced Ca2+o but alsoto polycations such as the ECPs andL-arginine–derivedpolyaminesputrescine,spermidine, and spermine, whose produc-tion is markedly increased during asth-ma (3–7, 11) or bymany RNA respiratoryviruses that exacerbate asthma, such as in-fluenza A and Newcastle disease virus,which either contain polyamines in the vi-ral envelope or produce them as part oftheir requirement for replication (22, 23).To test our hypothesis, we examined hu-man ASM samples from nonasthmaticand asthmatic subjects, and used two mod-els of allergen-induced airway inflammation,together with a mouse model of targetedCaSR gene ablation from ASM.
RESULTS
CaSR expression in human andmouse airways is increasedduring asthmaIn human bronchial biopsies and inmouseinterlobular bronchi, CaSR was immu-nolocalized within the SM22a-positivesmooth muscle layer, with additional ex-pression in bronchial epithelium (Fig. 1A).
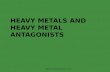
Fig. 1. CaSR immunolocalizes to human andmouse airways and is overexpressed in asthma. (A) Hu-man airway biopsy (upper panels) or mouse intralobular bronchi (lower panels) stained with CaSR antibody
(red) and SM22a (green) show immunoreactivity in both smooth muscle and epithelium. Scale bars,10 mm.(B) Human and mouse ASM cells stained with anti-SM22a antibody and showing CaSR immunoreactivity.Scale bars,100 mm. (C) qRT-PCR shows higher CaSR expression in moderate asthmatics than in healthysubjects [n = 4 patients per group, fold change versus healthy, mean (line) ± SD (box)]. (D) Western analysisof CaSR protein shows substantially elevated CaSR expression in moderate asthmatics (n = 5 patients pergroup). (E) Exposure of healthy human ASM cells to TNF-a (20 ng/ml) or IL-13 (50 ng/ml) for 48 hours signifi-cantly increased CaSR protein expression (n = 5 patients per group) compared to vehicle control for either cy-tokine. (F) CaSRmRNA expression was significantly greater in mice after induction of airway inflammation withMAs in comparison to unsensitized mice [n = 4 mice per group; 10 airways per mouse, fold change versusunsensitized, mean (line) ± SD (box)]. Statistical comparisons were performed [on DDCt values for (C) and(F)] by two-tailed, unpaired Student’s t tests (C, D, and F) and one-way analysis of variance (ANOVA) withBonferroni post hoc test (E). *P
-
R E S EARCH ART I C L E
CORRECTED 27 APRIL 2015; SEE FULL TEXT by guest on June 5, 2021
http://stm.sciencem
ag.org/D
ownloaded from
Isolated human and mouse ASM cells retained CaSR expression(Fig. 1B).
Quantitative reverse transcription polymerase chain reaction (qRT-PCR)and Western analysis of human ASM cells demonstrated that bothCaSRmRNA (Fig. 1C) and protein (Fig. 1D) expression were increasedabout threefold in moderate asthmatics compared to nonasthmatics(“healthy”). Furthermore, in human ASM cells from healthy indivi-duals, 48 hours of exposure to the asthma-associated proinflammatorycytokines, tumor necrosis factor–a (TNF-a) and interleukin-13 (IL-13),significantly increased CaSR protein expression (Fig. 1E and fig. S1C).qRT-PCR of laser capture microdissected ASM layers of intralobularbronchi in lung sections showed an about threefold increase in CaSRmRNA expression in mixed allergen (MA)–sensitized mice comparedto ASM from unsensitized mice (Fig. 1F). Together, these results indi-cate that the CaSR is present in human andmouse ASM and its expres-sion is increased in asthma. Furthermore, in vitro effects of cytokines onhuman ASM, and the effects of MA sensitization in a mouse model ofallergic asthma, provide an evidence for the role of inflammation in up-regulation of CaSR expression.
Polycations implicated in asthma pathogenesis activatethe human CaSRInmany cell types, CaSR activation results in an increase in intracellularCa2+ concentration ([Ca2+]i) arising frommobilization of Ca
2+i (14). To
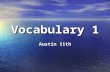
test the hypothesis that polycations that are up-regulated during asthmaactivate theCaSR,wemeasured changes in [Ca2+]i inhumanembryonickid-ney (HEK) 293 cells stably expressing the human CaSR (HEK-CaSR),or HEK293 cells stably expressing an empty vector (HEK-0). A repre-sentative Western blot of HEK-CaSR and HEK-0 is shown in fig. S2A.Consistent with this hypothesis, HEK-CaSR, but not HEK-0, cells ex-hibited significant increases in [Ca2+]i after exposure to (i) ECP [10mg/ml,a concentration well below the cytotoxic levels (24) and comparable tothose measured in the sputum of some asthmatic subjects (6, 7)], (ii)the polycationic peptide poly-L-arginine [PLA; 300 nM; amimetic ofma-jor basic protein (8)], and (iii) the polycation spermine (1 mM) (Fig. 2Aand fig. S2, B to D, for single traces). For each of these agonists, the in-crease in [Ca2+]i was inhibited by the calcilytic NPS89636 (100 nM) (Fig.2A and fig. S2, B to D, for single traces). Additional calcilytics, NPS2143(1 mM) or Calhex 231 (1 mM), also prevented spermine-induced CaSRactivation (Fig. 2A and fig. S2D).
Calcilytics prevent increases in Ca2+i in ASM fromasthmatic patientsIn human ASM, several endogenously produced agents such as acetyl-choline (ACh) and histamine evoke increases in [Ca2+]i, which driveAHR, remodeling, and production of a range of inflammatory cytokinesand other mediators in asthma (20, 25). Accordingly, we hypothesizedthat activation of CaSR in ASM also leads to an increase in [Ca2+]i, andpredicted that this effect would be enhanced in asthmatics.
We found that the sensitivity of human asthmatic ASM in the ab-sence of agents that increase [Ca2+]i was significantly higher than that ofASM from nonasthmatics in the presence of 2mM [Ca2+]o (Fig. 2B, leftpanel, and fig. S3, A andB, for single traces). Inhibition of theCaSRwiththe calcilytic NPS2143 (1 mM) blunted the [Ca2+]o hyperresponsivenessof asthmatic ASM cells, highlighting the functional role of CaSR in thissetting (Fig. 2B, right panel, and fig. S3, A and B, for single traces).
Having determined the sensitivity of human ASM to [Ca2+]o, wethen tested the ability of the CaSR to alter [Ca2+]i responses to ACh
www.Scie
in human asthmatic and healthy ASM. In the presence of physio-logical [Ca2+]o [that is, 1 mM, at which the CaSR is half-maximallyactive (14)], exposure to 1 mM ACh produced the expected increase in[Ca2+]i, which was significantly greater in ASM from asthmatic pa-tients (Fig. 2C). Inhibiting CaSR with NPS2143 reduced the [Ca2+]iresponse to ACh to levels that were not significantly different fromthose measured in healthy ASM (Fig. 2C and fig. S3C). These effectswere even more pronounced in the presence of 2 mM Ca2+o, a con-centration at which the CaSR is fully active, whereas they could not beobserved in the presence of 0.5 mM [Ca2+]o, which is below thethreshold for CaSR activation (fig. S3C).
Histamine (1 mM) also evoked an increase in [Ca2+]i in both healthyand asthmatic ASM, which was significantly greater in asthmatic ASM(Fig. 2D). Preexposure of asthmatic ASM to calcilytic also reduced [Ca2+]iresponses to histamine so that they did not differ statistically fromthose in healthyASM (Fig. 2D). Furthermore, an alternative,membrane-impermeant CaSR agonist, Gd3+ (0.1 mM), evoked a further increase in[Ca2+]i in human ASM in the absence (fig. S3D) or presence (fig. S3E) ofhistamine, effects that were greater in asthmatic than in nonasthmaticASM cells. Together, these results demonstrate that, in ASM cells, theCaSR is functional and contributes to the regulation of baseline ASM[Ca2+]i. Accordingly, in asthmatic ASM cells, the CaSR may contributeto a higher baseline [Ca2+]i, a leading cause of AHR, whereas calcilyticsrestore baseline [Ca2+]i.
Calcilytics abrogate signaling pathways characteristic ofairway contractility and asthma in human ASMTo determine potential mechanisms by which CaSR modulates con-tractility relevant to asthma, we explored two mechanisms in non-asthmatic and asthmatic ASM: cyclic adenosine monophosphate(cAMP), which should induce bronchodilation, and phospholipaseC (PLC)/inositol 1,4,5-trisphosphate (IP3), an important contributorto bronchoconstriction, with the idea that CaSR activation shouldsuppress cAMP but elevate IP3 (16). Indeed, in the presence of 2 mMCa2+o, cAMP levels were low, and calcilytics increased cAMP, partic-ularly in asthmatic ASM (fig. S3F). Measurements of cellular IP3 con-tent showed that, particularly in asthmatic ASM, CaSR antagonistsuppressed the elevated levels of IP3 in the presence of 2 mM Ca
2+o
(fig. S3G).In addition to targeting phosphodiesterases to inhibit cAMP
breakdown, many of the pipeline or existing drugs for asthma targetactivation of signaling pathways dependent on extracellular signal–regulated kinase 1/2 (ERK1/2), p38 mitogen-activated protein kinase(MAPK), and phosphatidylinositol 3-kinase/Akt phosphorylation (26, 27).Therefore, we examined the effect of activation of the ASM CaSR onthese pathways in human ASM cells. In healthy ASM, CaSR activationwith 5mMCa2+o induced a significant increase in p38MAPKphospho-rylation, an effect that was prevented by co-incubation with a calcilytic.Calcilytic treatment reduced ERK1/2 andAkt phosphorylation at 5mMCa2+o (Fig. 2, E and F, and fig. S4 for technical replicates). Overall, thesedata highlight the ability of CaSR to modulate signaling pathways acti-vated during asthma, which may contribute to altered ASM functionbeyond [Ca2+]i.
SM22aCaSR∆flox/∆flox mice are protected frompolycation-induced bronchoconstrictionTo determine whether activation of the CaSR in ASM leads to AHRin vivo, we generated mice with targeted CaSR ablation from visceral
nceTranslationalMedicine.org 22 April 2015 Vol 7 Issue 284 284ra60 3
http://stm.sciencemag.org/
-
R E S EARCH ART I C L E
www.ScienceTranslationalMedicine.org
CORRECTED 27 APRIL 2015; SEE FULL TEXT by guest on June 5, 2021
http://stm.sciencem
ag.org/D
ownloaded from
SM cells by breeding LoxP-CaSRmice withSM22a-Cre mice (28, 29). The resultingSM22aCaSR∆flox/∆flox mice [knockout (KO);fig. S5] were comparable to Cre-negative[wild-type (WT)] littermates in appear-ance, reproductive abilities, body weight,and life expectancy (fig. S5, B and C).Fluorescence-activated cell sorting analysisshows that molecular CaSR ablation fromASM resulted in a significant reduction inCaSR immunoreactivity in KO cells, whichwas 27% of that seen in WT cells. In con-trast, CaSR ablation from ASM cells didnot significantly alter the expression ofthe smooth muscle marker SM22a (fig.S5D). Successful ASM CaSR ablation wasdemonstrated functionally by the evidencethat Ca2+o (1 to 5 mM) and an alternative,membrane-impermeant CaSR agonist,Gd3+ (100 mM to 1 mM), evoked an in-crease in [Ca2+]i in WT ASM cells, whichwas significantly greater than that mea-sured in cells from KO mice (fig. S5E,upper panels for single traces and lowerpanels for biological replicates). Never-theless, lungs from KOmice appeared his-tomorphologically comparable to those ofWT mice and did not exhibit fibrosis, in-flammation, or impaired alveolarization(fig. S5F). Intralobular bronchi from WTandKOmice also had comparable luminaldiameters (fig. S5G).
The intrinsic baseline contractility ofintralobular bronchi was not affected byCaSR ablation from ASM cells, as shownby exposure either to high K+ (40 mM,fig. S5H) or to increasing concentrationsof ACh (1 nM to 30 mM), both of whichevoked bronchoconstriction of compa-rable magnitude in WT and KO mousebronchi (Fig. 3A). In intralobular bron-chi from WT mice, treatment with eitherspermine (300 mM, Fig. 3B) or 2.5 mM[Ca2+]o (Fig. 3E) enhanced the broncho-constrictor response to ACh. CaSR ablationfrom ASM blunted both spermine-induced(Fig. 3C) and [Ca2+]o-induced (Fig. 3F)sensitization of the ACh response. Further-more, spermine (10 mM to 3 mM) inducedsensitization of the ACh response in pre-contractedWT, but not inKOmouse bron-chi (Fig. 3D).Consistentwith these findings,spermine also enhanced the response toACh (0.5 mM) in precision-cut lung slicesfromWT animals (Fig. 3G, and summaryin Fig. 3H). This effect was prevented bycalcilytic treatment (NPS89636, 300 nM,Fig. 3H). However, the effects of either
Fig. 2. Polycations activate the human CaSR in recombinant systems and human ASM cells, partic-ularly those from asthmatics. (A) ECPs (n = 7), PLA (n = 6), or spermine (n = 17) each increased [Ca2+] in
iHEK-CaSR, but not in HEK-0 cells (ECP, n = 3; PLA, n = 6; spermine, n = 6). In HEK-CaSR cells, the calcilyticNPS89636 prevented these increases (ECP, n = 3; PLA, n = 3; and spermine, n = 4). Two alternative calcilytics,NPS2143 (n=4) andCalhex 231 (n=5), also prevented spermine-inducedCaSR activation. (B) In humanASMcells, exposure to 2 mM [Ca2+]o increased [Ca2+]i in asthmatic but not in healthy ASM cells (left), an effectpreventedby the calcilytic NPS2143 (right) (n=3each). (C andD) In the presenceof 1mMCa2+o, exposure toACh (C) (n = 4 healthy, n = 4 asthmatic) or histamine (D) (n = 5 healthy, n = 4 asthmatic) resulted in increasesin [Ca2+]i, which was greater in asthmatic ASM cells. This effect was prevented by NPS2143. ns, not signif-icant. (E and F) Western analysis [exemplar gel (E) and summary data (F)] of healthy ASM cell lysates showsthe effects of 5 mM Ca2+o in the absence or presence of NPS2143 on Akt, p38 MAPK, and ERK phosphoryl-ation (n=17 to 19 independent experiments fromcells isolated fromn=2nonasthmatic patients). Statisticalsignificance was determined by one-way ANOVA with Bonferroni post hoc test (A), two-way ANOVA withBonferroni post hoc test (B to D), or one-way ANOVAwith Dunn post hoc test (F). *P< 0.05, **P < 0.01, ***P <0.001, significantly different from control HEK-CaSR (A), from control healthy or asthmatic ASM (B to D), orfrom 5mMCa2+o (B). Source data, details of the statistical analysis, and P values are given in the Supplemen-tary Excel spreadsheet.
22 April 2015 Vol 7 Issue 284 284ra60 4
http://stm.sciencemag.org/
-
R E S EARCH ART I C L E
CORRECTED 27 APRIL 2015; SEE FULL TEXT by guest on June 5, 2021
http://stm.sciencem
ag.org/D
ownloaded from
spermine or calcilytic were not observedin lung slices from KO mice (Fig. 3G, andsummary in Fig. 3I). Together, these obser-vations suggest that activation of the ASMCaSR leads to AHR, an effect that can beprevented by calcilytic treatment.
Calcilytics reduce airway resistancein MA-sensitized mice in vivoTo test the effects of pharmacologicalCaSR activators and inhibitors on pul-monary resistance, we directly measuredairflow resistance (RL) in anaesthetized,paralyzed, mechanically ventilatedmice.In naïvemice, acute preexposure (10min)to the nebulized calcimimetic R568 (1 mM)resulted in an increase inRL across the lungsafter inhalational challenge with the syn-thetic muscarinic receptor agonist metha-choline (MCh; 0 to 50 mg/ml), whereasthe calcilytic NPS2143 (1 mM) was able toreverse this effect (Fig. 4A). Next, we devel-oped an MA murine asthma model thatleads to robust inflammation and remodel-ing in the lungs ofMA-sensitizedmice (fig.S6). In these mice, there was a marked in-crease in RL after MCh challenge, and pre-exposure toR568 resulted in an even greaterincrease in RL. Moreover, the calcilytic wasable to significantly reduce AHR in thesemice (Fig. 4B).
Calcilytics reduce AHR andinflammation in ovalbumin-sensitized,ovalbumin-challengedmice in vivoIncreased arginase activity drives AHR viathe production of polyamines (4, 5, 11),but whether the CaSR is involved in thisprocess is unknown. To test the ability ofcalcilytics to prevent polycation-inducedAHR in vivo, we assessed the effects ofnebulizedPLA(3mM)in thepresenceor ab-sence of the calcilytic NPS89636 (3 mM).As an alternative, noninvasive methodformeasurement of AHR (30, 31), we per-formed whole-body plethysmography inconscious, unrestrained naïve mice bymeasuring enhanced pause (Penh). Al-though Penh does not directly measureairway resistance, particularly in obligatenasal breathers such as mice, it has beenwidely used as an indicator of airway ob-struction in response to inhaledMCh (0.1to 100 mg/ml) (31). PLA significantlyincreased Penh at MCh concentrationsgreater than 10 mg/ml, an effect that wasabolishedbycotreatmentwith thenebulized
Fig. 3. CaSR ablation fromASM cells blunts polycation-induced bronchoconstriction. (A to F) Tensionmeasurements in intralobular bronchi frommice with targeted CaSR ablation from ASM cells (SM22aCaSR∆flox/∆flox,
KO) and from SM22a-Cre mice (WT). (A) Under control conditions, bronchial contractility to ACh was notaffected by CaSR ablation (WT, n = 14; KO, n = 12). Exposure to spermine enhanced contractility to AChin WT (B, n = 6) but not in KO mice (C, n = 7). (D) Spermine alone induced constriction in WT but not inKOmouse intralobular bronchi, whichwas significant at 1mM (WT,n=4; KO,n=7) and above (WT,n=3; KO,n=7). The sensitivity to AChwas increasedwhen [Ca2+]owas raised from thephysiological 1 to 2.5mM inWTmice (E, n = 6) but not in KO mice (F, n = 7). (G to I) In precision-cut lung slices fromWT mice, ACh-inducedcontraction of intralobular bronchi was potentiated by spermine and prevented by the calcilytic NPS89636(G, upper panels) [representative of seven experiments; summary in (H); n= 7], whereas therewas no sperm-inepotentiationor calcilytic effect in KOmice (G, lower panels) [representativeof four experiments; summaryin (I); n = 4]. Scale bar,100 mm. Statistical comparisons were made by two-way ANOVA (A to F) (between curvesand for WT versus KO for identical agonist concentrations) or two-tailed, paired Student’s t test (H and I) (per-formed on the nonnormalized data). *P < 0.05, **P < 0.01, ***P < 0.001, statistically different from respectiveWTcontrols. Source data, details of the statistical analysis, and P values are given in the Supplementary Materials.
www.ScienceTranslationalMedicine.org 22 April 2015 Vol 7 Issue 284 284ra60 5
http://stm.sciencemag.org/
-
R E S EARCH ART I C L E
CORRECTED 27 APRIL 2015; SEE FULL TEXTD
ow
calcilytic. Calcilytic treatment per se significantly reduced Penh in naïveanimals treated with MCh (30 mg/ml) (Fig. 5A).
Having demonstrated the ability of calcilytics to reduce AHR evokedby polyamines, we tested their anti-inflammatory properties in an es-tablishedmodel of allergic asthma (31), the ovalbumin (OVA)–sensitized,OVA-challengedmouse. Calcilytic inhalation significantly reduced AHRinduced by OVA sensitization (Fig. 5B). Bronchoalveolar lavage fluid(BALF) collected from the calcilytic-treated mice also showed a significantreduction in inflammatory cell infiltration (total numbers, macrophages, eo-sinophils, and lymphocytes; Fig. 5C) and concentrations of ECP, IL-5, IL-13,and TNF-a (Fig. 5D) when compared to their vehicle-treated counterparts.Biochemical analysisof terminalbloodsamples showed that inhaledcalcilyticdid not significantly affect serum ionized calcium at 1 hour after inhalation(vehicle control 0.9 ± 0.1mMversus calcilytic 0.8 ± 0.1mM;P > 0.05; n=3 per experimental group) and up to 24 hours (1.0 ± 0.1 mM and 1.0 ±0.1 mM, 4 and 24 hours after calcilytic treatment, respectively; P > 0.05;n=3per experimental group).These results suggest that theobservedeffectsof the calcilytics are not ascribed to systemic changes in Ca2+o homeostasis.
http:nloaded from
DISCUSSION
Our study highlights the expression of the CaSR inASMand identifies afundamental pathophysiological role for this receptor in the context of
www.Scie
by guest on June 5, 2021//stm
.sciencemag.org/
asthma. The fact that inflammatory cationic proteins known to corre-late with asthma severity can activate the CaSR expressed by ASM cellsat physiologically relevant concentrations to elevate [Ca2+]i and increasethe contractility of the ASMnonspecifically provides both a rational ex-planation for the genesis of nonspecific AHR in asthma and a basis forthe direct mechanistic link between this phenomenon and airway in-flammation. These findings raise the possibility that the CaSR directlyinfluences mechanisms involved in inflammatory cell recruitment andactivation. In turn, production of asthma-relevant cytokines can furtherincrease CaSR expression, thereby generating a positive feedback loop.Thus, locally delivered calcilytics would have the advantage of breakingthis cycle by reducing inflammation and by blunting ASM hyperre-sponsiveness. Indeed, in two different in vivomodels of allergic asthma,interfering with CaSR signaling positively affects multiple aspects ofairway disease, benefits not achieved by single-drug therapies. In thissense, the CaSR represents a truly novel potential therapeutic targetin asthma.
[Ca2+]o is known to be increased at inflammation sites (18, 32),therefore activating the CaSR, leading to an increase in [Ca2+]i andp38 MAPK activation and a decrease in the intracellular cAMP pool.In addition, the CaSR is activated by a plethora of molecules, particu-larly polyamines, which act orthosterically (independently of [Ca2+]o) tohelp stabilize the unique conformations of the receptor. This leadsto preferential coupling to different G proteins, a process defined asligand-directed targeting of receptor stimulus (33). The relevance of theCaSR to local and systemic symptoms in asthma and other airway dis-eases is potentially immense, extending beyond its innate expression inASM and any local regulation of [Ca2+]o. In asthma, airway inflamma-tion leads to increased release of polycations, which are acceptedmarkersof asthma severity, locally and into the systemic circulation (2–7). SputumECP concentrations in asthmatics have been reported to attain about10 mg/ml (6, 7), which here we show to be well within the concentrationrange sufficient to activate the CaSR. Added to this is arginase-drivenproduction of spermine, spermidine, and putrescine, which are increas-ingly implicated in asthma pathophysiology (4, 5, 11). From an envi-ronmental perspective, CaSR agonists may also be presented to theairways in the form of smoke (Ni2+) or car fumes (Pb2+ and Cd2+)(34) and bacterial/viral infections (polyamines) (22, 23).
In addition to elevating [Ca2+]i and, therefore, priming ASM cells torespond with a lower threshold to pathophysiological stimuli, CaSRmay also enhance sensitization of airways to Ca2+, for example, via cou-pling to protein kinase C and Rho kinase, as demonstrated in other cellsystems, namely, HEK-CaSR (35), a topic that is currently unexploredin the lung but is highly relevant to the increasing interest in targetingsensitization mechanisms (36). Beyond contributions to AHR andairway remodeling (25), calcilytics prevent activation of intracellularpathways, which are currently being targeted by pipeline asthma drugs,specifically p38 MAPK and phosphodiesterase inhibitors (26). Indeed,both classes of inhibitors target various inflammatory cells, which re-lease key mediators responsible for the remodeling and inflammationcharacteristic of these diseases. For this reason, local delivery of calcily-tics has the potential to target not only one of the key possible causes forasthma but also the production of proinflammatory cytokines that con-tribute to its exacerbations. Consistent with this hypothesis is the abilityof the calcilytics to reduce inflammatory cell infiltration in the BALF ofOVA-sensitized mice.
Our ex vivo experiments show that activation of the airway CaSRincreases responses to bronchoconstrictors by about 20 to 25%. Albeit
Fig. 4. Activation of the airway CaSR exacerbates AHR in vivo. (A) In me-chanically ventilated, unsensitized mice, acute exposure to the calcimimetic
R568 increasedbronchoconstriction toMChchallenge,measured as increasedairway resistance (RL). The calcilytic prevented the AHR induced by R568, butevinced little effect on its own. (B) MA-sensitized mice showed enhanced re-sponse to MCh. Preexposure to the calcimimetic resulted in a further increasein RL , whereas the calcilytic NPS2143 reducedAHR. Statistical comparisons be-tween the curvesweremadeby two-wayANOVA, Bonferroni post hoc test.n=5per condition. **P < 0.01, ***P < 0.001 statistically different from control, ###P <0.001 statistically different from calcimimetic. Source data, details of the sta-tistical analysis, and P values are given in the Supplementary Materials.
nceTranslationalMedicine.org 22 April 2015 Vol 7 Issue 284 284ra60 6
http://stm.sciencemag.org/
-
R E S EARCH ART I C L E
CORRECTED 27 APRIL 2015; SEE FULL TEXT by guest on June 5, 2021
http://stm.sciencem
ag.org/D
ownloaded from
apparently small, this effect is substantial if we consider that resistanceto the air flow increases to the reciprocal of the fourth power of thebronchial radius. Indeed, direct measurements of airway resistance innaïve animals show that CaSR activators increase RL by roughly three-fold. Thus, antagonizing theCaSRmight provide a highly beneficialma-neuver for the treatment of AHR in vivo.
Individually, each of the approaches used in the current study has itsinherent limitation. Concerning the ex vivo studies, wire myography rec-ords small airway tension in isolation, and although lung slices allowairway lumen size measurements in a system where the local paracrineenvironment is intact, there is no active innervation. For in vivo studies,flexiVent data are obtained in anaesthetizedmice,which aremechanicallyventilated, and even thoughwhole-animal plethysmography records lungfunction in freely moving, spontaneously breathing animals, it can onlyreport indirectly on airway resistance. However, this broad set of exper-imental approaches has generated complementary data sets that, as thecomplexity of themeasuring systems steadily builds, have provided com-prehensive, overlapping evidence to show calcilytic-dependent diminu-tion of airway responsiveness in normal and pathological paradigms.This idea is central to the thesis that locally delivered calcilytics may rep-resent a brand new therapeutic approach to the treatment of asthma.
www.ScienceTranslationalMedicine.org
Asthma represents a multifactorial dis-ease, involving many cell types in the air-way beyond immune cells, including theepithelium and ASM. Accordingly, the ex-pression and potential role of CaSR incells of the airways become important. Al-though our study focused on the ASMCaSR, it is worth noting that our observa-tions demonstrate CaSR expression inairway epithelial cells. Epithelial cell dam-age is pathognomonic of asthma, whereasthe presence of environmental polyaminesand other CaSR activators might directlyactivate a functional epithelial CaSR, whichmight in turn contribute to airway remod-eling and altered epithelial permeabilityin asthma, as demonstrated by CaSR ac-tivation in other epithelia (16). On theother hand, CaSR is functionally expressedin human andmouse macrophages, whereit plays a crucial role in activation ofNLRP3inflammasome and release of IL-1b (17, 18),known to be involved in asthma patho-genesis. In addition, we found CaSR ex-pression in human eosinophils (fig. S7),and previous studies have shown that eo-sinophil degranulation (37) and migra-tion across the lung epithelium (38) isalso Ca2+o-dependent. Although our dataclearly show a role for the ASMCaSR, par-ticularly in the context of airway inflamma-tion and asthma, given the expression ofCaSR on both immune and epithelial cells,exploring their role will be important in fu-ture studies in the context of identifyingCaSR modulators to alleviate AHR and al-lergic asthma.
Owing to their ability to evoke rapid fluctuations in plasma PTH, aknown anabolic stimulus to bone growth, systemic calcilytics were ini-tially developed as anti-osteoporotic drugs and reached phase 2 clinicaltrials for this purpose in humans (39). Our in vivo data indicate thatlocally delivered calcilytics do not significantly affect plasma [Ca2+]olevels (hence, presumably PTH levels) up to 24 hours after treatment,suggesting that calcilytic administration directly to the lung in humansshould not negatively affect mineral ion homeostasis.
Amajor implication of CaSR in the airway is its potential for targetingin the context of disease. Accordingly, calcilytic-based therapeutics coulddo both, prevent as well as relieve AHR. What is unclear at present iswhether CaSR overexpression and/or its responsiveness to polycationsand calcilytics is uniform across the entire spectrum of asthma, particu-larly in view of the understanding that severe asthmamay differ in patho-physiology and responsiveness to conventional pharmacotherapy (40).This reservation notwithstanding, it would certainly seem likely thatone appealing line of future research will be the possibility that the CaSRcan contribute to the development of asthma in some patients by creatinga permissive environment for polycation action, with the corollary thatsuch patients can be identified and treated prophylactically. Furthermore,given the involvement of polycations in other environmental airway
Fig. 5. Nebulized calcilytics prevent AHR and inflammation in mice in vivo. (A) Nebulized calcilytic(NPS89636) prevented PLA-induced AHR in unsensitized, consciousmice. Data are presented as percentage
changes in enhanced pause, Penh (DPenh, %), in MCh-challenged mice (n = 6 mice per condition). (B to D)Calcilytic abrogated hyperresponsiveness (B) (n = 5 for control, n = 6 each for vehicle and calcilytic), reducedinflammatory cell infiltration (C) (n=11), and the concentrations of ECP (n=11), IL-5, IL-13, and TNF-a (D) (n=10 for vehicle, and n = 11 for calcilytic) into the BALF from OVA-sensitized, OVA-challenged mice. *P < 0.05,**P
-
R E S EARCH ART I C L E
CORRECTED 27 APRIL 2015; SEE FULL TEXT
insults, such as from pollution and respiratory infection, one mightspeculate that the potential exists for CaSR-targeted approaches to al-leviate other inflammatory airway diseases.
by guest on June 5, 2021http://stm
.sciencemag.org/
Dow
nloaded from
MATERIALS AND METHODS
Study designThe objectives of the study were to test the hypothesis that the CaSR is apotential anti-AHR and anti-inflammatory target for asthma therapy.
For experiments in primary human ASM cells, all protocols wereapproved by the Mayo Clinic Institutional Review Board. Surgical lungspecimens of patients undergoing lobectomy for focal, noninfectiousdisease were obtained, and normal areas of third- to sixth-generationbronchi were identified and dissected for further use. Patient clinicaldata (combination of physician diagnosis, pulmonary function tests in-cluding bronchodilator responses, and imaging results) were used toidentify those with moderate asthma versus not. However, once thesedata were recorded, all patient identifiers were deleted, and sampleswere stored and processed with unique number identifiers, preventingretrospective identification of patients. Accordingly, the protocol wasconsidered “minimal risk” and did not require explicit patient consent.For both asthmatics (all moderate, n = 5) and nonasthmatics (healthy;patients with no documented history of asthma, n = 5), patient agesranged from 40 to 80 years. Both groups included only those patientsundergoing thoracic surgery for focal, noninfectious pathology (for ex-ample, localized tumor with negative lymph nodes; bronchoalveolarcarcinomawas excluded). Samples in either groupwere used for a rangeof experimental protocols, although not all five patient samples wereused for every protocol.
All animal procedures were approved by local ethical review andconformed with the regulations of the UK Home Office and theAnimal Care and Use Committees of all the participating institutions.Procedures were in strict accordance to the guidelines of the AmericanPhysiological Society.
Mice with CaSR-targeted gene ablation from ASM cells were gener-ated by breeding SM22a-Cre recombinase mice (28) with LoxP CaSR(flanking exon 7 of CaSR) (29). The floxed CaSRmouse strain was gen-erated from C57BL/6 × SVJ129 mice backcrossed with C57BL/6 for atleast eight generations. SM22a-Cre+ were bred with floxed-CaSR+/+ togenerate SMCaSR∆flox/∆flox mice (lacking full-length CaSR in ASM),which were used as KO mice, and SM22a-Cre−/− × floxed-CaSR+/+
(expressing full-length CaSR in ASM) acted as WT, control mice.CaSR-LoxP × SM22a-Cre mice were inbred for at least three genera-tions before being used for experiments. Both WT and KO mice arefertile and viable with a normal life span (fig. S5, B and C). For theMA model, 6- to 8-week-old C57/Bl6 mice were purchased from TheJackson Laboratory, and for noninvasive Penh measurements, 6- to 8-week-old BalbC male mice were used (Harlan). For laser capture mi-croscopy experiments, lungs from four mice (10 airways per mouse)were used. For Ca2+i imaging in human ASM, wire myography, andlung slice experiments, on the basis of our previous experience, aminimum of three patients per condition (at least 15 cells per experi-ment per patient) or a minimum of three mice per genotype are re-quired to achieve statistical significance. For experiments in humanASM, wire myography, lung slices, and in vivo plethysmography, lackof responses to ACh (in vitro and ex vivo experiments) orMCh (in vivoexperiments) was a preestablished exclusion criterion, as was obvious
www.Scie
epithelial damage or denudation in lung slice experiments whensamples were observed under light microscopy. Data are presented asaverage ± SEM, which was calculated invariably from n (the number ofpatients or animals, biological replicates), with the exception ofWesternanalysis of Akt, p38MAPK, and ERK1/2 phosphorylation, where n rep-resents the number of individual experiments (technical replicates).Animals were assigned to the experimental groups at random, butthe investigators were not blinded.Where appropriate, data were testedfor normality (Shapiro-Wilk test).
In vitro studiesHuman ASM cells. Human ASM cells were isolated and cultured
as previously described (41) in Dulbecco’s modified Eagle’s medium/F12 (Life Technologies) supplementedwith 10% fetal bovine serum, pen-icillin, and streptomycin. Culturingwas limited to less than four passages,and retention of the ASM phenotype was verified by expression ofsmooth muscle cell markers SM22a or calponin.
HEK-293 studies. Cells stably transfectedwith humanCaSR (HEK-CaSR) or empty vector (HEK-0, negative control) were generatedand cultured as described previously (42). All cells tested negativefor mycoplasma.
Mouse ASM cells. Cells were obtained using previously describedtechniques (43). Passage 1 to 4 cells were serum-starved for 24 hoursbefore experimentation.
Ca2+i imaging. Techniques using the ratiometric Ca2+ indicator
fura-2 AM have been previously described (25, 41). An inverted micro-scope (Olympus IX71) and fluorescence source (Xenon arc or LED)along with rapid perfusion system was used to alter [Ca2+]o (1 to 5 mM),add agonists (ACh, histamine) and Gd3+ (100 mM to 1 mM), or addthe polycations ECP (10 mg/ml), PLA (300 mM), or spermine (1 mM).During experimentation requiring different [Ca2+]o, these changes weremade ~30 min before experiment (but after dye loading to ensure noconfounding effects of Ca2+o on CaSR or on the loading per se). Wherestated, cells were incubated with calcilytics (NPS89636, NPS2143, orCalhex 231) for 20 min.
Phospho-Akt, p38MAPK, and phospho-ERK cell signaling. Hu-manASM cells isolated from two healthy subjects (n = 17 to 19 technicalrepeats) were passaged up to 10 times and plated for phosphorylationexperiments. Cells were exposed to 0.5 mM Ca2+o (control), 5 mM Ca
2+o,
or 5 mMCa2+o in the presence of NPS2143 (1 mM), and experiments werecarried out and as described previously (44).
Protein analysis. Standard SDS–polyacrylamide gel electropho-resis with 4 to 15% gels and polyvinylidene difluoride membraneswere used with protein detection using far-red (LI-COR Odyssey XL)or horseradish peroxidase–conjugated secondary antibodies. CaSRprotein expression was normalized to glyceraldehyde-3-phosphate de-hydrogenase (GAPDH).
Ex vivo studiesForce measurements in intralobular bronchi. Second- to third-
order intralobular bronchial rings (2 mm in length) were isolated fromthe left lobe, cleaned, and mounted in a wire myograph (610M, DMT)for measurement of isometric force as described previously (45) at apassive tension of 2 mN. For the nonpaired experiments (WT versusKO), the data were normalized to themeanmaximum forWT,whereasfor the paired experiments (control versus treatedwith spermine or high[Ca2+]o), each data point was normalized to the maximum of its owncontrol. To obtain the spermine concentration-response curve, bronchi
nceTranslationalMedicine.org 22 April 2015 Vol 7 Issue 284 284ra60 8
http://stm.sciencemag.org/
-
R E S EARCH ART I C L E
CORRECTED 27 APRIL 2015; SEE FULL TEXT by guest on June 5, 2021
http://stm.sciencem
ag.org/D
ownloaded from
were first precontracted with ACh to achieve about 50% of maximaltone, and then rising concentrations of spermine were added to thebath. The averaged data points of each set were fitted with sigmoidaldose-response curve, variable slope (ACh), or second-order polynomialcurve (spermine).
Precision-cut lung slices. Samples were prepared as previously de-scribed (46). Intralobular bronchi were identified under a lightmicroscope(Nikon Diaphot) and imaged during bronchoconstrictor stimula-tion. Bronchial lumen areas were measured with ImageJ. Tone wasestablished using 1 mM ACh, and the effects of polyamine spermine(300 mM) were determined in the absence and presence of calcilyticNPS89636 (300 nM).
Laser capture microdissection and qRT-PCR. Air-inflated lungsfrom control and MA-challenged cohort of mice were rapidly frozenunder ribonuclease-free conditions (47). Samples were cryosectioned,and total RNA was isolated as described previously (47). CaSR mRNAwas standardized against ribosomal protein S16 mRNA (DCt). Indi-vidual DCt values were standardized against themean DCt of the con-trol group (nonasthmatic humans and control mice, DDCt) on whichstatistical comparisons were performed. For graphical representa-tion, the mean fold difference ± SD between the groups was calcu-lated as 2−DDCt ± SD.
Immunofluorescence. Standard techniques were applied to cryo-sections of paraformaldehyde-fixed biopsies from human lung andvibratome-cut, paraformaldehyde postfixedmurine lung slices. A TCS-SP2 AOBS confocal laser-scanning microscope (Leica) was used forimage acquisition.
In vivo studiesMeasurements of airway resistance (RL). RL was measured by
flexiVent (SCIREQ) under pentobarbital anesthesia and pancuroniumparalysis using established techniques (47, 48). In select cases, animalswere prenebulized with the CaSR-positive (R568; 1 mM) and/or CaSR-negative (NPS2143; 1 mM) allosteric modulators (Tocris) 10min beforeMCh challenge.
MAmodel. C57/Bl6mice received daily intranasalmixture of 10 mgofOVA and extracts fromAlternaria,Aspergillus, andDermatophagoides(house dust mite) for 4 weeks (Greer Labs), each dose in 50 ml ofphosphate-buffered saline (PBS). Control mice received intranasal PBS.Animals were analyzed 24 hours after the last sensitization.
Whole-body plethysmography. Noninvasive barometric plethys-mography (Buxco Research Systems) was carried out in unrestrained,conscious mice as described previously (31). After establishment ofbaseline enhanced pause (Penh) (49), standard nebulized MCh chal-lenge was performed (0.1 to 100 mg/ml in saline; 3-min recordingper dose; PulmoStar nebulizer, Sunrise Medical), and Penh values werecalculated and expressed as percentage change (DPenh, %). Althoughthe physiological data provided by a Penh-based approach differ fromthose using the forced oscillation technique of the flexiVent system, thenoninvasive approach allowed for longitudinal measurements ofbaseline and chronic drug effects in the same animals (as below).
Polycation-induced AHR. Twenty-fourhours after baselinemeasure-ments of Penh with MCh challenge, mice were exposed to aerosolizedPLA (3mM),NPS89636 (3mM),PLA+NPS89636, or vehicle [0.3% (v/v)dimethyl sulfoxide (DMSO)] for 1hour, andMChchallengewas repeated.For experiments with PLA + NPS89636 or vehicle, mice were pretreatedfor 30minwithNPS89636 (or vehicle) and then cotreatedwithPLA.Micewere allowed to recover for 1 week between each set of experiments. Sep-
www.Scie
arately, naïve animals were exposed to nebulizedNPS89636, and 0, 4, and24 hours later, the blood was collected and analyzed for serum Ca2+.
OVA-induced AHR. MaleBalbCmicewere sensitized on days 0 and5 by intraperitoneal injection of 100 mg ofOVApermouse and 50mg ofaluminum hydroxide per mouse in PBS. Thirteen days after the finalinjection, Penh was recorded during MCh challenge. The next day,mice were challenged twice with 0.5% nebulizedOVA (in PBS, w/v) andnebulized NPS89636 (3 mM, or 0.03% DMSO vehicle) by inhalation,4 hours apart. Twenty-nine hours after the first OVA inhalation, Penhwas again recorded during MCh challenge.
BALF analysis. Bronchoalveolar lavage was performed after the ter-minal experiment, cells were isolated byCytoSpin centrifugation (ThermoScientific), and total and differential cell counts were performed afterLeishman’s staining. Enzyme-linked immunosorbent assay (R&D) andECP (Aviscera Bioscience Inc.)measurementswere performed accordingto the manufacturer’s instructions.
Materials and antibodiesNPS89636was a gift fromNPSPharmaceuticals Inc.NPS2143 andCalhex231 were purchased from Tocris. All other chemicals were purchasedfrom Sigma-Aldrich, unless otherwise stated. Primary antibodies usedwere as follows: anti-SM22a (Abcam); anti-CaSR (AnaSpec or Abcam);and anti–phospho-ERK, anti–phospho-Akt, and anti-p38 MAPK (CellSignaling). Secondary antibodies used were as follows: Alexa Fluor 488,Alexa Fluor 594, or Alexa Fluor 647 (Life Technologies). Nuclei werecounterstained using Hoechst. Omission of the primary antibodiesacted as negative control.
StatisticsStatistical significance was determined usingGraphPad Prism 6 software.Student’s two-sided, unpaired, or paired t test was used to compare agroup of two data sets; one- or two-way ANOVA with Bonferronipost hoc test, or nonparametric (Friedman) with Dunn post hoc test, asstated in the figure legends, was used to compare three ormore data sets.Where applicable, statistical comparisons were made between nonnor-malized data groups, but normalized data are presented in the figures.
SUPPLEMENTARY MATERIALS
www.sciencetranslationalmedicine.org/cgi/content/full/7/284/284ra60/DC1Materials and MethodsFig. S1. Negative controls and original Western blots for Fig. 1.Fig. S2. Polycations increase [Ca2+]i by acting on the human CaSR.Fig. S3. Calcilytics prevent CaSR activation in human asthmatic ASM.Fig. S4. Technical replicates of data presented in Fig. 2E and summarized in Fig. 2F.Fig. S5. Phenotypic characterization of the SM22aCaSR∆flox/∆flox mouse.Fig. S6. Validation of the MA asthma model.Fig. S7. CaSR expression in human eosinophils.Database S1. Source data for Figs. 1 to 5 and figs. S1 to S5 (provided as Excel file).Reference (50)
REFERENCES AND NOTES
1. W. W. Busse, The relationship of airway hyperresponsiveness and airway inflammation:Airway hyperresponsiveness in asthma: Its measurement and clinical significance. Chest138, 4S–10S (2010).
2. D. Y. Koller, G. Halmerbauer, T. Frischer, B. Roithner, Assessment of eosinophil granuleproteins in various body fluids: Is there a relation to clinical variables in childhood asthma?Clin. Exp. Allergy 29, 786–793 (1999).
nceTranslationalMedicine.org 22 April 2015 Vol 7 Issue 284 284ra60 9
http://stm.sciencemag.org/
-
R E S EARCH ART I C L E
CORRECTED 27 APRIL 2015; SEE FULL TEXT by guest on June 5, 2021
http://stm.sciencem
ag.org/D
ownloaded from
3. K. Lonnkvist, C. Hellman, J. Lundahl, G. Hallden, G. Hedlin, Eosinophil markers in blood, serum,and urine for monitoring the clinical course in childhood asthma: Impact of budesonidetreatment and withdrawal. J. Allergy Clin. Immunol. 107, 812–817 (2001).
4. M. Kurosawa, Y. Shimizu, H. Tsukagoshi, M. Ueki, Elevated levels of peripheral-blood, nat-urally occurring aliphatic polyamines in bronchial asthmatic patients with active symp-toms. Allergy 47, 638–643 (1992).
5. M. L. North, H. Grasemann, N. Khanna, M. D. Inman, G. M. Gauvreau, J. A. Scott, Increasedornithine-derived polyamines cause airway hyperresponsiveness in a mouse model ofasthma. Am. J. Respir. Cell Mol. Biol. 48, 694–702 (2013).
6. M. L. Bartoli, E. Bacci, S. Carnevali, S. Cianchetti, F. L. Dente, A. Di Franco, D. Giannini, M. Taccola,B. Vagaggini, P. L. Paggiaro, Clinical assessment of asthma severity partially corresponds tosputum eosinophilic airway inflammation. Respir. Med. 98, 184–193 (2004).
7. P. G. Gibson, K. L. Woolley, K. Carty, K. Murree-Allen, N. Saltos, Induced sputum eosinophilcationic protein (ECP) measurement in asthma and chronic obstructive airway disease(COAD). Clin. Exp. Allergy 28, 1081–1088 (1998).
8. S. Pegorier, L. A. Wagner, G. J. Gleich, M. Pretolani, Eosinophil-derived cationic proteinsactivate the synthesis of remodeling factors by airway epithelial cells. J. Immunol. 177,4861–4869 (2006).
9. A. J. Coyle, S. J. Ackerman, C. G. Irvin, Cationic proteins induce airway hyperresponsivenessdependent on charge interactions. Am. Rev. Respir. Dis. 147, 896–900 (1993).
10. T. Homma, J. H. Bates, C. G. Irvin, Airway hyperresponsiveness induced by cationic proteinsin vivo: Site of action. Am. J. Physiol. Lung Cell. Mol. Physiol. 289, L413–L418 (2005).
11. H. Meurs, H. Maarsingh, J. Zaagsma, Arginase and asthma: Novel insights into nitric oxidehomeostasis and airway hyperresponsiveness. Trends Pharmacol. Sci. 24, 450–455 (2003).
12. M. Zhang, T. Caragine, H. Wang, P. S. Cohen, G. Botchkina, K. Soda, M. Bianchi, P. Ulrich,A. Cerami, B. Sherry, K. J. Tracey, Spermine inhibits proinflammatory cytokine synthesis inhuman mononuclear cells: A counterregulatory mechanism that restrains the immune re-sponse. J. Exp. Med. 185, 1759–1768 (1997).
13. H. Jones, W. Paul, C. P. Page, A comparison of allergen and polycation induced cutaneousresponses in the rabbit. Br. J. Pharmacol. 133, 1181–1189 (2001).
14. E. M. Brown, G. Gamba, D. Riccardi, M. Lombardi, R. Butters, O. Kifor, A. Sun, M. A. Hediger,J. Lytton, S. C. Hebert, Cloning and characterization of an extracellular Ca2+-sensing recep-tor from bovine parathyroid. Nature 366, 575–580 (1993).
15. E. F. Nemeth, D. Shoback, Calcimimetic and calcilytic drugs for treating bone and mineral-related disorders. Best Pract. Res. Clin. Endocrinol. Metab. 27, 373–384 (2013).
16. D. Riccardi, P. J. Kemp, The calcium-sensing receptor beyond extracellular calcium ho-meostasis: Conception, development, adult physiology, and disease. Annu. Rev. Physiol.74, 271–297 (2012).
17. G. S. Lee, N. Subramanian, A. I. Kim, I. Aksentijevich, R. Goldbach-Mansky, D. B. Sacks, R. N. Germain,D. L. Kastner, J. J. Chae, The calcium-sensing receptor regulates the NLRP3 inflammasomethrough Ca2+ and cAMP. Nature 492, 123–127 (2012).
18. M. Rossol, M. Pierer, N. Raulien, D. Quandt, U. Meusch, K. Rothe, K. Schubert, T. Schoneberg,M. Schaefer, U. Krugel, S. Smajilovic, H. Brauner-Osborne, C. Baerwald, U. Wagner, Extra-cellular Ca2+ is a danger signal activating the NLRP3 inflammasome through G protein-coupled calcium sensing receptors. Nat. Commun. 3, 1329 (2012).
19. J. Paccou, C. Boudot, C. Renard, S. Liabeuf, S. Kamel, P. Fardellone, Z. Massy, M. Brazier,R. Mentaverri, Total calcium-sensing receptor expression in circulating monocytes is increasedin rheumatoid arthritis patients with severe coronary artery calcification. Arthritis Res. Ther. 16,412 (2014).
20. K. Mahn, O. O. Ojo, G. Chadwick, P. I. Aaronson, J. P. Ward, T. H. Lee, Ca2+ homeostasis and struc-tural and functional remodelling of airway smooth muscle in asthma. Thorax 65, 547–552 (2010).
21. T. Koopmans, V. Anaparti, I. Castro-Piedras, P. Yarova, N. Irechukwu, C. Nelson, J. Perez-Zoghbi,X. Tan, J. P. Ward, D. B. Wright, Ca2+ handling and sensitivity in airway smooth muscle: Emergingconcepts for mechanistic understanding and therapeutic targeting. Pulm. Pharmacol. Ther. 29,108–120 (2014).
22. U. Bachrach, Metabolism and function of spermine and related polyamines. Annu. Rev.Microbiol. 24, 109–134 (1970).
23. P. McCann, Inhibition of Polyamine Metabolism: Biological Significance and Basis for NewTherapies (Academic Press, Orlando, FL, 1987).
24. S. Motojima, E. Frigas, D. A. Loegering, G. J. Gleich, Toxicity of eosinophil cationic proteinsfor guinea pig tracheal epithelium in vitro. Am. Rev. Respir. Dis. 139, 801–805 (1989).
25. K. Mahn, S. J. Hirst, S. Ying, M. R. Holt, P. Lavender, O. O. Ojo, L. Siew, D. E. Simcock, C. G. McVicker,V. Kanabar, V. A. Snetkov, B. J. O’Connor, C. Karner, D. J. Cousins, P. Macedo, K. F. Chung,C. J. Corrigan, J. P. Ward, T. H. Lee, Diminished sarco/endoplasmic reticulum Ca2+ ATPase(SERCA) expression contributes to airway remodelling in bronchial asthma. Proc. Natl.Acad. Sci. U.S.A. 106, 10775–10780 (2009).
26. C. Page, M. Cazzola, Bifunctional drugs for the treatment of asthma and chronic obstruc-tive pulmonary disease. Eur. Respir. J. 44, 475–482 (2014).
27. J. K. Burgess, J. H. Lee, Q. Ge, E. E. Ramsay, M. H. Poniris, J. Parmentier, M. Roth, P. R. Johnson,N. H. Hunt, J. L. Black, A. J. Ammit, Dual ERK and phosphatidylinositol 3-kinase pathways controlairway smooth muscle proliferation: Differences in asthma. J. Cell. Physiol. 216, 673–679 (2008).
www.Scien
28. J. J. Lepore, L. Cheng, M. Min Lu, P. A. Mericko, E. E. Morrisey, M. S. Parmacek, High-efficiencysomatic mutagenesis in smooth muscle cells and cardiac myocytes in SM22a-Cre transgenicmice. Genesis 41, 179–184 (2005).
29. W. Chang, C. Tu, T.-H. Chen, D. Bikle, D. Shoback, The extracellular calcium-sensing recep-tor (CaSR) is a critical modulator of skeletal development. Sci. Signal. 1, ra1 (2008).
30. M. Lomask, Further exploration of the Penh parameter. Exp. Toxicol. Pathol. 57 (Suppl. 2),13–20 (2006).
31. S. Fernandez-Rodriguez, K. J. Broadley, W. R. Ford, E. J. Kidd, Increased muscarinic receptoractivity of airway smooth muscle isolated from a mouse model of allergic asthma. Pulm.Pharmacol. Ther. 23, 300–307 (2010).
32. I. T. Olszak, M. C. Poznansky, R. H. Evans, D. Olson, C. Kos, M. R. Pollak, E. M. Brown, D. T. Scadden,Extracellular calcium elicits a chemokinetic response from monocytes in vitro and in vivo. J. Clin.Invest. 105, 1299–1305 (2000).
33. A. D. Conigrave, D. T. Ward, Calcium-sensing receptor (CaSR): Pharmacological propertiesand signaling pathways. Best Pract. Res. Clin. Endocrinol. Metab. 27, 315–331 (2013).
34. M. E. Handlogten, N. Shiraishi, H. Awata, C. Huang, R. T. Miller, Extracellular Ca2+-sensingreceptor is a promiscuous divalent cation sensor that responds to lead. Am. J. Physiol.Renal Physiol. 279, F1083–F1091 (2000).
35. P. D. Ngo, R. J. MacLeod, V. Mukkada, R. Turki, G. T. Furuta, Epithelial calcium-sensing re-ceptor activation by eosinophil granule protein analog stimulates collagen matrix contrac-tion. Pediatr. Res. 73, 414–419 (2013).
36. S. L. Davies, C. E. Gibbons, T. Vizard, D. T. Ward, Ca2+-sensing receptor induces Rho kinase-mediated actin stress fiber assembly and altered cell morphology, but not in response toaromatic amino acids. Am. J. Physiol. Cell Physiol. 290, C1543–C1551 (2006).
37. F. Hoffmeyer, K. Sucker, C. Monse, H. Berresheim, B. Jettkant, N. Rosenkranz, T. Bruning, J. Bunger,Different patterns in changes of exhaled breath condensate pH and exhaled nitric oxide afterozone exposure. Adv. Exp. Med. Biol. 834, 39–47 (2015).
38. G. H. Wan, D. C. Yan, T. H. Tung, C. S. Tang, C. H. Liu, Seasonal changes in endotoxinexposure and its relationship to exhaled nitric oxide and exhaled breath condensate pHlevels in atopic and healthy children. PLOS One 8, e66785 (2013).
39. L. A. Fitzpatrick, C. E. Dabrowski, G. Cicconetti, D. N. Gordon, T. Fuerst, K. Engelke, H. K. Genant,Ronacaleret, a calcium-sensing receptor antagonist, increases trabecular but not cortical bonein postmenopausal women. J. Bone Miner. Res. 27, 255–262 (2012).
40. S. E. Wenzel, Asthma phenotypes: The evolution from clinical to molecular approaches.Nat. Med. 18, 716–725 (2012).
41. Y. S. Prakash, A. Iyanoye, B. Ay, C. B. Mantilla, C. M. Pabelick, Neurotrophin effects on in-tracellular Ca2+ and force in airway smooth muscle. Am. J. Physiol. Lung Cell. Mol. Physiol.291, L447–L456 (2006).
42. D. T. Ward, M. Z. Mughal, M. Ranieri, M. M. Dvorak-Ewell, G. Valenti, D. Riccardi, Molecularand clinical analysis of a neonatal severe hyperparathyroidism case caused by a stop mu-tation in the calcium-sensing receptor extracellular domain representing in effect a human‘knockout’. Eur. J. Endocrinol. 169, K1–K7 (2013).
43. D. W. McGraw, K. M. Fogel, S. Kong, A. A. Litonjua, E. G. Kranias, B. J. Aronow, S. B. Liggett,Transcriptional response to persistent b2-adrenergic receptor signaling reveals regulationof phospholamban, which alters airway contractility. Physiol. Genomics 27, 171–177 (2006).
44. W. D. McCormick, R. Atkinson-Dell, K. L. Campion, H. C. Mun, A. D. Conigrave, D. T. Ward,Increased receptor stimulation elicits differential calcium-sensing receptorT888 dephos-phorylation. J. Biol. Chem. 285, 14170–14177 (2010).
45. J. Q. Liu, D. Yang, R. J. Folz, A novel bronchial ring bioassay for the evaluation of small airwaysmooth muscle function in mice. Am. J. Physiol. Lung Cell. Mol. Physiol. 291, L281–L288 (2006).
46. M. J. Sanderson, Exploring lung physiology in health and disease with lung slices. Pulm.Pharmacol. Ther. 24, 452–465 (2011).
47. B. Aravamudan, S. K. VanOosten, L. W. Meuchel, P. Vohra, M. Thompson, G. C. Sieck, Y. S. Prakash,C. M. Pabelick, Caveolin-1 knockout mice exhibit airway hyperreactivity. Am. J. Physiol. Lung Cell.Mol. Physiol. 303, L669–L681 (2012).
48. K. H. Shalaby, L. G. Gold, T. F. Schuessler, J. G. Martin, A. Robichaud, Combined forcedoscillation and forced expiration measurements in mice for the assessment of airway hy-perresponsiveness. Respir. Res. 11, 82 (2010).
49. E. Hamelmann, J. Schwarze, K. Takeda, A. Oshiba, G. L. Larsen, C. G. Irvin, E. W. Gelfand,Noninvasive measurement of airway responsiveness in allergic mice using barometricplethysmography. Am. J. Respir. Crit. Care Med. 156, 766–775 (1997).
50. G. Hillas, K. Kostikas, K. Mantzouranis, V. Bessa, K. Kontogianni, G. Papadaki, S. Papiris, M. Alchanatis,S. Loukides, P. Bakakos, Exhaled nitric oxide and exhaled breath condensate pH as predictors ofsputum cell counts in optimally treated asthmatic smokers. Respirology 16, 811–818 (2011).
Acknowledgments: We acknowledge D. H. Edwards for access to wire myography equipment,D.Wright for his helpwith humanASM cells, D. Richards for the human eosinophil cytospins, andE. F. Nemeth for the gift of NPS89636 and helpful discussions. Funding: This workwas supported bygrants fromAsthmaUK (11/056, to C.J.C., J.P.T.W., D.R., and P.J.K.), the Cardiff Partnership Fund (toD.R., P.J.K., E.J.K., and W.R.F.), a Marie Curie Initial Training Network “Multifaceted CaSR” (to D.R. andP.J.K.), the Biotechnology and Biological Sciences Research Council (BB/D01591X to D.R. and P.J.K.),
ceTranslationalMedicine.org 22 April 2015 Vol 7 Issue 284 284ra60 10
http://stm.sciencemag.org/
-
R E S EARCH ART I C L E
CORRECTED 27 APRIL 2015; SEE FULL TEXT
and the U.S. NIH [HL056470, HL088029 (to Y.S.P.), and HL090595 (to C.M.P.)]. We also acknowledgesupport from the Department of Health via the National Institute for Health Research Comprehen-sive Biomedical Research Centre award to Guy’s & King’s College London and King’s College HospitalNHS Foundation Trust.Author contributions: P.L.Y., A.L.S., V.S., R.D.B., M.A.T., A.P.P.L., M.F., B.A., S.C.B.,M.S., T.D., S.Y., Z.C., K.R., M.E.B.K., and D.T.W. performed the experiments. W.C. generated the SM22aLoxP CaSR mice. Y.S.P., H.K., P.L.Y., P.J.K., and D.R. designed and analyzed the experiments and per-formed the statistical analyses. E.J.K., W.R.F., and K.J.B. developed the OVA-sensitized mouse asthmamodel. C.M.P. developed the MA mouse asthma model. C.J.C., J.P.T.W., P.J.K., Y.S.P., P.L.Y., and D.R.wrote the manuscript. Competing interests: D.R., P.J.K., C.J.C., and J.P.T.W. are co-inventors on apatent (WO2014049351) claiming the use of CaSR antagonists for the treatment of inflammatorylung disorders. The other authors declare that they have no competing interests.
www.Scien
Submitted 7 November 2014Accepted 24 February 2015Published 22 April 201510.1126/scitranslmed.aaa0282
Citation: P. L. Yarova, A. L. Stewart, V. Sathish, R. D. Britt Jr., M. A. Thompson, A. P. P. Lowe,M. Freeman, B. Aravamudan, H. Kita, S. C. Brennan, M. Schepelmann, T. Davies, S. Yung,Z. Cholisoh, E. J. Kidd, W. R. Ford, K. J. Broadley, K. Rietdorf, W. Chang, M. E. Bin Khayat,D. T. Ward, C. J. Corrigan, J. P. T. Ward, P. J. Kemp, C. M. Pabelick, Y. S. Prakash, D. Riccardi,Calcium-sensing receptor antagonists abrogate airway hyperresponsiveness and inflammationin allergic asthma. Sci. Transl. Med. 7, 284ra60 (2015).
ceTranslationalMedicine.org 22 April 2015 Vol 7 Issue 284 284ra60 11
by guest on June 5, 2021http://stm
.sciencemag.org/
Dow
nloaded from
http://stm.sciencemag.org/
-
inflammation in allergic asthmaCalcium-sensing receptor antagonists abrogate airway hyperresponsiveness and
Pabelick, Y. S. Prakash and Daniela RiccardiChang, Mohd E. Bin Khayat, Donald T. Ward, Christopher J. Corrigan, Jeremy P. T. Ward, Paul J. Kemp, Christina M. Davies, Sun Yung, Zakky Cholisoh, Emma J. Kidd, William R. Ford, Kenneth J. Broadley, Katja Rietdorf, WenhanP. Lowe, Michelle Freeman, Bharathi Aravamudan, Hirohito Kita, Sarah C. Brennan, Martin Schepelmann, Thomas Polina L. Yarova, Alecia L. Stewart, Venkatachalem Sathish, Rodney D. Britt , Jr., Michael A. Thompson, Alexander P.
DOI: 10.1126/scitranslmed.aaa0282, 284ra60284ra60.7Sci Transl Med
vivo, supporting clinical testing of these drugs for asthmatics.can prevent these effects both in vitro and in−−CaSR antagonists−−airway hyperreactivity. What's more, calcilytics
model of allergic asthma. Indeed, extracellular calcium and other asthma-associated activators of CaSR increased Asthmatic patients express higher levels of CaSR in their airways than do healthy individuals, as does a mouse
extracellular calcium can activate airway smooth muscle cells through the calcium-sensing receptor (CaSR). contribute to inflammation and airway hyperresponsiveness in allergic asthma. They show that elevated
. now show that extracellular calcium mayet alCalcium may help to build strong bones. However, Yarova Calcilytics may help asthmatics breathe easier
ARTICLE TOOLS http://stm.sciencemag.org/content/7/284/284ra60
MATERIALSSUPPLEMENTARY http://stm.sciencemag.org/content/suppl/2015/04/20/7.284.284ra60.DC1
CONTENTRELATED
http://stke.sciencemag.org/content/sigtrans/8/391/ra84.fullhttp://stke.sciencemag.org/content/sigtrans/8/405/ra122.fullhttp://stke.sciencemag.org/content/sigtrans/10/475/eaai8583.fullhttp://stm.sciencemag.org/content/scitransmed/7/307/307ra152.fullhttp://science.sciencemag.org/content/sci/349/6252/1106.fullhttp://science.sciencemag.org/content/sci/349/6252/1034.fullhttp://stm.sciencemag.org/content/scitransmed/7/301/301ra129.fullhttp://stm.sciencemag.org/content/scitransmed/7/301/301fs33.fullhttp://stm.sciencemag.org/content/scitransmed/7/288/288ed5.fullhttp://stke.sciencemag.org/content/sigtrans/8/374/ec112.abstracthttp://stke.sciencemag.org/content/sigtrans/3/143/re7.fullhttp://stm.sciencemag.org/content/scitransmed/5/174/174ra26.fullhttp://stm.sciencemag.org/content/scitransmed/6/256/256ra134.full
REFERENCES
http://stm.sciencemag.org/content/7/284/284ra60#BIBLThis article cites 49 articles, 8 of which you can access for free
PERMISSIONS http://www.sciencemag.org/help/reprints-and-permissions
Terms of ServiceUse of this article is subject to the
registered trademark of AAAS. is aScience Translational MedicineScience, 1200 New York Avenue NW, Washington, DC 20005. The title
(ISSN 1946-6242) is published by the American Association for the Advancement ofScience Translational Medicine
Copyright © 2015, American Association for the Advancement of Science
by guest on June 5, 2021http://stm
.sciencemag.org/
Dow
nloaded from
http://stm.sciencemag.org/content/7/284/284ra60http://stm.sciencemag.org/content/suppl/2015/04/20/7.284.284ra60.DC1http://stm.sciencemag.org/content/scitransmed/6/256/256ra134.fullhttp://stm.sciencemag.org/content/scitransmed/5/174/174ra26.fullhttp://stke.sciencemag.org/content/sigtrans/3/143/re7.fullhttp://stke.sciencemag.org/content/sigtrans/8/374/ec112.abstracthttp://stm.sciencemag.org/content/scitransmed/7/288/288ed5.fullhttp://stm.sciencemag.org/content/scitransmed/7/301/301fs33.fullhttp://stm.sciencemag.org/content/scitransmed/7/301/301ra129.fullhttp://science.sciencemag.org/content/sci/349/6252/1034.fullhttp://science.sciencemag.org/content/sci/349/6252/1106.fullhttp://stm.sciencemag.org/content/scitransmed/7/307/307ra152.fullhttp://stke.sciencemag.org/content/sigtrans/10/475/eaai8583.fullhttp://stke.sciencemag.org/content/sigtrans/8/405/ra122.fullhttp://stke.sciencemag.org/content/sigtrans/8/391/ra84.fullhttp://stm.sciencemag.org/content/7/284/284ra60#BIBLhttp://www.sciencemag.org/help/reprints-and-permissionshttp://www.sciencemag.org/about/terms-servicehttp://stm.sciencemag.org/
Related Documents