Birth defects after a history of subfertility: a registry-based case-control study in the Northern Netherlands M.E. Bos s1735187 EUROCAT Northern Netherlands, UMCG Supervisors: dr. H.E.K. de Walle dept GENETICS dr. A. Hoek dept OBGYN, dr. M.L. Haadsma dept GENETICS Research period: August 2012 – December 2012

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Birth defects after a history of subfertility:
a registry-based case-control study in the
Northern Netherlands
M.E. Bos s1735187
EUROCAT Northern Netherlands, UMCG
Supervisors: dr. H.E.K. de Walle dept GENETICS
dr. A. Hoek dept OBGYN, dr. M.L. Haadsma dept GENETICS
Research period: August 2012 – December 2012

1
1 Abstract
Background: In children conceived via assisted reproduction, an increased overall
risk for birth defects has been described in literature. In these newborn, a specific
increase has been reported for cardiovascular, musculoskeletal, urogenital and
gastrointestinal abnormalities. It remains uncertain, however, whether the rise in
occurrence of birth defects can be attributed to patient characteristics related to
subfertility, or to the treatment itself. The primary aim of the study is to evaluate
whether specific types of birth defects occur more often in offspring of subfertile
couples rather than in the offspring of fertile couples. The secondary aim is to
evaluate when birth defects are more likely to develop: after a history of subfertility
compared to the offspring of couples who received in vitro fertilization (IVF) or
intracytoplasmatic sperm injection (ICSI). The tertiary aim is to evaluate whether
prolonged time to pregnancy (TTP) in the group of subfertile couples shows a positive
correlation with regard to the prevalence of specific types of birth defects.
Methods: For performing this case-control study we used data from EUROCAT –
Northern Netherlands, a registry of birth defects. 4392 cases and 1456 (malformed)
controls were identified. These subjects were born between 1997 and 2010, and were
registered by EUROCAT. The cases were children and fetuses with major birth
defects of a non-genetic origin. Controls were defined as children and fetuses with a
chromosomal anomaly, a microdeletion or a monogenic anomaly. In the statistical
analysis, three groups of children and fetuses were compared: Sub-NC (n=296),
IVF/ICSI (n=174) and children and fetuses of fertile couples (n=5378).
Results: Compared with fertile women, Sub-NC women were at an increased risk of
having a child with a penoscrotal hypospadia (adjusted odds ratio [aOR]: 6.80; 95%
confidence interval [CI]: 2.35 – 19.63). Subfertile women conceiving via IVF/ICSI
were at an increased risk of having a child with a limb anomaly (aOR: 2.80; CI: 1.51 –
5.20), especially polydactyly (aOR: 5.26; CI: 2.47 – 11.20). Compared to fertile
women, the entire group of subfertile women (Sub-NC and IVF/ICSI) was at an
additional increased risk of having a child with an epispadia (aOR: 4.28; CI: 1.04 –
17.57) and cystic kidneys (aOR: 2.10; CI: 1.02 – 4.34). Surprisingly, Sub-NC women
showed a significant decreased risk for having a child with a congenital anomaly in
general, considering congenital anomalies occurring in all groups. Overall, a
significantly decreased risk of having a child with a congenital hip dysplasia was seen
in subfertile women, as was also described for the Sub-NC women alone.
Conclusions: In this study, Sub-NC women were at an increased risk of having a
child with specific major congenital anomalies, especially penoscrotal hypospadias.
The results of this study may be of great importance for public health, since
subfertility is a growing health issue since women are conceiving at older ages.
Keywords: assisted reproductive techniques, IVF, ICSI, congenital abnormalities,
history of subfertility
2
2 Preface
This paper is intended as the final report of the science project for the Master in
Medicine. The emphasis lies on whether there is a correlation between specific major
congenital anomalies and subfertility. After the study was conducted, which greatly
expanded my interest in this topic, I have the ambition to do more research within this
field.
The main objective of the science project is to improve different skills: scientific
writing, critical reading and perform statistical analyses. This research is based on the
analysis of data from fertile records of fourteen hospitals in the Dutch provinces
Friesland, Groningen and Drenthe. Performing this research improved my ability to
read and understand fertility- and gynaecology- records. Moreover, I became more
experienced in communicating with gynaecologists.
Performing this science project and writing this report have been made
possible with the help of my supervisors, Hermien de Walle, Annemieke Hoek and
Maaike Haadsma.
Marly Bos
18-01-2013
3
Contents
1 Abstract 1
2 Preface 2
3 Introduction 4
3.1 Congenital anomalies 4
3.2 Assisted reproductive technology 5
3.3 IVF and ICSI procedures 5
3.4 Perinatal risks and congenital anomalies associated with ART 6
3.5 The role of subfertility in increasing birth defects rates 7
3.6 The aim of the present study 8
4 Methods 9
4.1 EUROCAT 9
4.2 Study population 10
4.3 Definitions and recruitment 10
4.4 Methods 11
4.5 Statistical analysis 11
5 Results 13
5.1 General 13
5.2 Characteristics 14
5.3 Fertility status in two and three categories 15
5.4 Time to pregnancy 18
6 Discussion and Conclusion 20
6.1 Main results 20
6.2 Strengths and weaknesses 21
6.3 Potential underlying mechanisms 22
6.4 Further research 23
6.5 Public health implications 24
6.6 Conclusion 24
7 Acknowledgments 25
8 References 26
9 Nederlandse samenvatting (Dutch summary) 30
Appendix 32

4
3 Introduction
3.1 Congenital anomalies
The term congenital anomaly refers to a broad spectrum of defects in body structures.
Congenital anomalies can be divided into anomalies of a genetic nature or anomalies
of a non-genetic nature. Genetic anomalies include chromosomal disorders (e.g.,
Down syndrome); single gene (monogenic) disorders, including those that are
autosomal recessive (e.g., cystic fibrosis), automosal dominant (e.g., Marfan
syndrome), or X-linked (e.g., hemophilia); as well as multifactorial disorders which
result from the interaction of multiple genetic and environmental factors. The latter
include birth defects such as a cleft lip/palate, congenital heart disease, and neural
tube defects. Non-genetic etiologies include environmental factors. Examples of non-
genetic defects are maternal phenylketonuria (PKU) or diabetes, teratogens (e.g.,
alcohol consumption) and infections. An important cause of perinatal mortality are
congenital anomalies, where 6-12% of stillbirths are attributed to a congenital
anomaly(1).
Congenital anomalies can be classified into four different categories. They can
be subdivided according to their presumed pathogenesis into malformations,
deformations, disruptions and dysplasias. Malformations are caused by an intrinsically
abnormal developmental process which leads to defects of organs or certain body
parts. Generally, malformations already occur in the first eight weeks of gestation and
are the result of a defect in embryonic development. Common occurring
malformations are neural tube defects and congenital heart defects. Deformations,
however, are not caused by intrinsically abnormal development, but are rather
produced by abnormal mechanical forces which distort otherwise normal structures
and could develop at any time in gestation. Oligohydramnion, for instance, may lead
to a child being born with an abnormal foot position. Unlike malformations or
deformations, disruptions results from an extrinsic disturbance leading to a
morphologic anomaly to an organ or body part. Anomalies caused by extrinsic
disturbance are typically caused by adverse environmental factors such as teratogenic
drugs, compression or strangulation. Anomalies can also appear as the result of
abnormal organization or function of cells into tissues, called dysplasias. When cells
are not correctly organized, this may lead to abnormal growth, resulting, for instance,
in skeletal dysplasia(2).
While congenital anomalies can be classified by the suspected underlying
cause, they may also be subdivided according to severity; as are major or minor
anomalies. The difference between major- and minor anomalies is that the former
have medical and/or social implications and often require surgery to be corrected,
while the latter generally at most have a cosmetic impact. Though minor anomalies
may be associated with a disorder or disability, they generally do not impede leading a
normal life and rarely require surgical intervention. Between 1981 and 2009, 2.8% of
all pregnancies in the Netherlands were affected by a major congenital anomaly(3).
5
3.2 Assisted reproductive technology
An assisted reproductive technique (ART) which is well known to the general public
is in vitro fertilization (IVF). The first IVF-baby, Louise Brown, was born in 1978.
Subsequently, over three million IVF children were born(5) and in Europe alone up to
3.9% of all pregnancies are conceived via IVF(6). Another ART is intracytoplasmatic
sperm injection (ICSI)(7). Ten to twenty percent of couples are subfertile: which
means they have an active waiting time to pregnancy of over 12 months(4). A
considerable number of these subfertile couples request the use of an assisted
reproductive technology in order to conceive. One of the reasons for the increasing
amount of ART requests is the fact that women start trying to conceive at increased
age. Not only do older woman have diminished fecundity, they also have an increased
risk for gestational diabetes, placenta previa, breech presentation, operative vaginal
delivery, Caesarean section, postpartum haemorrhage, delivery before 32 weeks
gestation, birth weight below the 5th
centile and stillbirth(8).
In addition, a Swedish population-based study reports a higher risk of
pregnancy complications after ART itself, regardless of increased parental age(9).
While women who conceive via IVF generally show lower smoking rates in early
pregnancy and have higher level of education, the increased odds of pregnancy
complications nevertheless persist(10).
Previous research has shown that children born after ART have more perinatal
health problems compared to naturally conceived children. Prematurity and low birth
weight, for example, are seen more often in ART-children, as well as perinatal
mortality and neonatal intensive care committal(11,12).
ART is also associated with higher rates of birth defects in offspring, although
contributing mechanisms are still controversial. Nonetheless, it is conceivable that
ART-related procedures interfere with developmental processes. Factors which ought
to be taken into account are, for instance, bypassing the natural selection of gametes
and artificially maturing the ovum. Additionally, the early embryonic development
takes place in vitro and the embryo is transferred into an altered uterus as the result of
ovarian hyperstimulation. Besides ART-related procedures, subfertility itself should
also be considered as a contributing mechanism, rather than just the ART procedures
themselves.
In the next sections, the IVF and ICSI procedures will be reviewed first, followed by a
discussion of the results of pregnancies after ART and the history of subfertility.
3.3 IVF and ICSI procedures
IVF refers to a procedure designed to overcome infertility. This procedure aims at
achieving a pregnancy as a direct result of the intervention. First, the ovaries are
stimulated by a combination of fertility medication, followed by the aspiration of
multiple oocytes from ovarian follicles. The oocytes are, then, fertilized by sperm in
the laboratory (hence "in vitro", meaning “in glass” in Latin), after which one or more
embryos are transferred into the uterine cavity. These steps occur over about a two-
week interval, which is called an IVF cycle.

6
The number of embryo’s which are transferred into the uterus is positively
associated with pregnancy rates. On the other hand, transferring multiple embryos has
a positive correlation with twin pregnancies. Transferring the embryos is successful
most of the times, but the biggest problem of the IVF cycle is embryo-implantation.
Of the IVF procedures started only 25-30% lead to a pregnancy. Of these pregnancies
another 20-25% is lost in abortion or as extrauterine gravidity. In total, only 20-25%
of IVF cycles results in the delivery of a child. Most couples undergo more than one
cycle, and the cumulative success rate of three cycles is 50%(13,14).
In 1992, ICSI was for the first time successfully used in humans. This was the
next step in assisted reproductive techniques(15). The technique of ICSI depends on
bringing a single spermatozoa directly into the cytoplasma of an oocyte by injection.
This procedure is performed as part of an IVF cycle, and is particularly useful when
semen parameters are suboptimal or when fertilization rates after conventional IVF
treatment were low or nil. Next to bypassing the natural selection of the fertilizing
sperm, ICSI may appear as a traumatic event which could damage the egg by the
operative procedure. Nevertheless, fertilization is generally successful and is usually
followed by normal embryonic development(16).
When embryos of good quality remain that are not transferred to the uterus,
they can be cryopreserved for future use. Around 10-20% of embryos do not survive
the thawing process. The freezing and thawing process is thought to cause subtle
damage to the embryos. Systematic reviews of observational studies have found that
children born after transfer of frozen-thawed embryos have better perinatal outcomes
than those born after transfer of fresh embryos (i.e., lower rates of preterm birth, low
birth weight, growth restriction, perinatal mortality). Malformation rates are
comparable, while data on growth, childhood morbidity, and mental development
were limited though with few differences appeared between the groups(17,18). The
reason for the slightly higher number of healthy children born after cryopreservation
compared to children born after fresh transfer (in most studies) is not known. It may,
however be related to differences in endometrial receptivity between women
undergoing fresh versus cryopreserved embryo transfer (e.g., adverse effects of
ovarian stimulation in ‘fresh’ IVF cycles). Another hypothesis is that freezing and
thawing serves as a selection mechanism, since only the most viable embryo’s survive
this procedure.
3.4 Perinatal risks and congenital anomalies associated with ART
Over the years, assisted reproductive techniques have become widely accepted in
society. However, removing and handling gametes outside the body has always raised
concerns what the short- and long-term safety outcomes may be. For couples
considering ART request it is important to know the risks of ART techniques. Next to
that, society as a whole will benefit from the evaluation of perinatal and
neurodevelopmental risks associated with ART, since adverse outcomes would place
a heavy burden on the health care system. Negative short-term outcomes are
repeatedly described. Singletons born after ART are more often preterm and of low
birth weight rather than naturally conceived singletons(12,19). Among the former
7
group, there are higher numbers of perinatal mortality and they need to be admitted to
neonatal intensive care more often (11,12). The low birth weight may not only
indicate preterm birth but also a growth retarding effect. This effect was demonstrated
by Kallen et al., and they found that 5.1% of IVF singleton infants were small for
gestational age, whereas no more than 2.8% among all singleton infants delivered
were born with a low birth weight. This study also reported a doubled over-all
hospitalization rate for IVF children(20).
Additionally, another current discussion in the field concerns the safety
outcome of ART with regard to the prevalence of birth defects. In a meta-analysis,
Hansen et al. (2005) showed an 40% increased risk for having a child with birth
defects after conceiving via ART(21). Previous research by Hansen et al. in 2002
suggested already that children born after ART were at higher risk of having multiple
major birth defects, especially musculoskeletal defects(22).
A study by Reefhuis et al. found a relationship between ART and several
specific anomalies. They showed an increase in the occurrence of septal heart defects,
cleft lip (with or without cleft palate), esophageal atresia and anorectal atresia in
singletons born after ART(7). Another study confirmed the findings by Reefhuis et al.
reported a higher prevalence of neural tube defects(23). Davies et al. (2012) reported
a higher prevalence of cardiovascular, musculoskeletal, urogenital and gastro-
intestinal congenital anomalies, as well as cerebral palsy in children conceived after
ART(24). Multiple studies showed a correlation between ART and the VACTERL-
association, which stands for multiple associated defects: Vertebral defects, Anal
atresia, Cardiac defects, Tracheo-Esophageal fistula, Renal malformations and Limb
defects(7,23).
Hypospadia is the only congenital anomaly which shows a disparity between
IVF and ICSI in terms of occurrence: the risk increases slightly when ICSI is
compared to IVF. This discrepancy may, however, be the result of paternal subfertility
rather than the ICSI procedure per se(22,25-27).
Summarizing, there appears to be a relationship between ART and congenital
malformations. However, the underlying mechanisms remain unclear. Whether the
ART procedure itself is responsible for the higher risk, or the underlying subfertility,
is an issue which still needs to be addressed
3.5 The role of subfertility in increasing birth defects rates
When the health condition in children born after ART is studied, it is imperative to
know the difference between the effects of the treatment techniques and the
underlying subfertility. A premature birth after a history of subfertility is known to be
associated with an increased risk of perinatal death(28).
Evidence is accumulating indicating that spontaneous conception after a
history of subfertility and its determinants are involved in increasing birth defects,
rather than ART-related procedures. These results were to be expected, since
subfertile couples are generally older, and age is a factor which is typically associated
with a higher risk of birth defects in offspring. Nevertheless, after correction for
parental age, it is argued in multiple studies that a history of subfertility was still

8
associated with higher rates of birth defects. A role of the underlying subfertility in
increasing birth defect rates was suggested for the first time by Ghazi et al. They
reported higher rates of congenital anomalies in a subgroup of couples who had
experienced subfertility for at least four years(29). Zhu et al. confirmed that a history
of subfertility without assisted conception is associated significantly with birth defects
and they described a high hazard ratio (hazard ratio [HR]: 1.20; 95% confidence
interval [CI]: 1.07 to 1.35) for congenital anomalies in subfertile couples who
conceived naturally, compared to fertile couples. These associations did not disappear
after correction for maternal age, maternal BMI at conception, smoking, alcohol
and/or coffee consumption during pregnancy and the level of education(30).
Zhu et al. and Seggers et al. found that increased time to pregnancy (TTP) was
associated with a higher prevalence of birth defects(30,31). Another study reported
that the increasing odds for birth defects after ART disappeared after correction for
time to pregnancy(23).
3.6 The aim of the present study
An increase of several specific types of birth defects has been repeatedly described
after ART: cardiovascular defects, musculoskeletal defects, neural tube defects,
urogenital defects, gastrointestinal abnormalities, cleft lip/palate and cerebral palsy.
Whether a history of subfertility is also associated with specific types of birth defects
remains unclear. This information would be quite useful in counseling subfertile
couples and may be applied in (extended) prenatal screening.
Therefore, the primary aim of this case-control study was to examine whether
specific types of birth defects occur more often in offspring of subfertile couples
compared to offspring of fertile couples. The secondary aim was to evaluate whether
specific types of birth defects occur more (or less) often after a history of subfertility
compared to the offspring of couples who received IVF/ICSI. The tertiary aim was to
evaluate whether prolonged time to pregnancy in the group of subfertile couples
shows a positive association with the prevalence of specific types of birth defects.
9
4 Methods
4.1 EUROCAT
In order to accurately describe and analyze birth defects among couples using ART or
suffering from subfertility, a massive amount of data needs to be available for
improving the power of the research. The EUROCAT Northern Netherlands
(EUROCAT NNL) database proved indispensible in this research, and offered a
wealth of information. EUROCAT is a population-based birth defects registry and
since 1981 it registers children and fetuses suffering from congenital anomalies
diagnosed before or after birth, born in the provinces Groningen, Friesland or
Drenthe. In this database, however, no information is collected on non-malformed
infants. Approximately 18.500 births yearly are covered by the registration. Among
those births which are registered, all types of pregnancy outcomes are represented and
there is no discrimination for gestational age. Deliveries that are registered are divided
into five categories: live birth, live born but deceased, stillbirth, terminations of
pregnancy because of a fetal anomaly and miscarriage. For a fetus’ death to be
considered a stillbirth the gestation needs to be at least 24 weeks and the fetus needs
to have either died in utero or during birth. For miscarriages the upper age limit is 24
weeks, there is no weight limit.
Although EUROCAT provides ample date on major anomalies detected in
children, it has far less information to offer on minor anomalies, since it had been
decided only to include those anomalies under certain conditions according to the
EUROCAT Central Registry Guidelines(32). As to what exactly constitutes an
anomaly in infants, EUROCAT relies on the classification of the 9th
and 10th
revisions
of the WHO International Classification of Diseases (ICD). Births up to 2001 were
classified according the ICD-9 classification; from 2002 onward, the ICD-10
classification is used. Information is gathered in a number of ways. Anomalies can be
reported by different medical institutions or sometimes by the parents themselves. In
addition, EUROCAT has an active and systematic search for children and fetuses with
a congenital anomaly in hospital records. The upper age limit for children to be
included up is 10 years. Parents are to provide written informed consent for
registration; the participation rate is over 80%. Of those parents who agree with
registration, around 80% returned the EUROCAT questionnaire. In this questionnaire,
parents were asked to report characteristics such as parental age, height, pre-
pregnancy weight, chronic illnesses, education, smoking, alcohol consumption, the
use of medication, socioeconomic status and information on mode of conception.
Subsequently, information on the use of medication dispended up to approximately
three months before conception and during pregnancy, is collected via community
pharmacies. A telephone interview with the mother is scheduled once the pharmacies
reported on the medication which was dispensed, to verify whether the mother
actually has taken the medication and if she has taken any self-medication before
conceiving or during the pregnancy. In case the questionnaire was not fully
10
completed, the telephone interview granted the opportunity to fill in any missing
answers.
4.2 Study population
The subjects that were included in the study were born between 1997 and 2010 and
were defined as follows: children and fetuses with a major congenital anomaly.
Major congenital anomalies were divided into different diagnostic groups
according to the EUROCAT international guidelines(32). For example subjects with
congenital heart defects were divided into subgroups based on scientific
epidemiological insights(33).
In order to test the accuracy of conclusions drawn from the EUROCAT data, we
choose for a case-control design. Extensive literature research on the topic of
subfertility and birth defects, showed no evidence of subfertility causing chromosomal
anomalies, microdeletion anomalies or monogenic anomalies. Therefore children and
fetuses born between 1997 and 2010 with a chromosomal anomaly, a microdeletion or
a monogenic anomaly were selected to act as a control group. Additionally, in studies
on risk factors for congenital anomalies the use malformed controls is widely
accepted(34).
For each group of cases, a different control group was selected carefully, as it
would be counterproductive to the aim of the study to allow the controls to have the
same congenital anomaly as the cases to which they were compared. The selection
procedure thus entailed, for example, that a child suffering from a chromosomal
anomaly, such as trisomy 18, and also a neural tube defect was used as a control for
all subgroups of anomalies, except for the group affected by neural tube defects. An
overview of the number of controls used for each congenital anomaly can be found in
TABLE 1.
4.3 Definitions and recruitment
From the initial 7720 participants born between 1997 and 2010, 246 participants were
excluded as they were coded into the diagnostic group ‘other syndromes’.
In the EUROCAT questionnaire parents were asked whether they had
problems conceiving with regard to this specific pregnancy. If participants did not
answer the question or when they filled in ‘unknown’, they were excluded.
Participants who answered ‘no’ were included as confirmed fertile participants. When
the answer given was ‘yes’, they were asked to specify whether they eventually
conceived spontaneously or if they received treatment; IVF, ICSI, IUI, KID, hormonal
therapy or other therapy. In case IVF, ICSI or IUI was used, parents were asked to
specify whether donor semen and/or donor oocytes were used. As our research
focuses on subfertile participants who conceived naturally and via IVF/ICSI, all other
fertility therapies were excluded.
To objectify the problems in becoming pregnant, a fertility record search was
performed. Lists of the self-reported subfertile participants were sent to the
EUROCAT contact persons in 15 hospitals in the provinces Groningen, Friesland and
Drenthe. The contacts were requested to let us perform a search for fertility (or
11
gynaecology) records of the participants in question. Medical records provided
information on fertility status, information on IVF/ICSI treatment procedures, fertility
diagnosis and TTP in terms of years. TTP was defined as the time between the active
child wish of the couple and conception. In case of a miscarriage, TTP-onset had to be
reset and ended at conception of the child included in the present study. Participants
were confirmed to be subfertile when they had a fertility record in which at least an
orientating fertility research was reported and/or a TTP of at least one year. The
confirmed subfertile participants were included. FIGURE 1 shows the flowchart.
EUROCAT NNL obtained permission from the registered participants to
request for medical information for scientific purposes. EUROCAT NNL also
obtained permission from the ethics committee of the University Medical Center
Groningen to use their data for scientific purposes.
4.4 Methods
Essentially, the fertility status was divided into two categories in the analysis; fertile
versus subfertile. In case there were sufficient numbers, i.e. more than 3 exposed
cases per category, the fertility status was divided into three categories rather than
two; fertile versus subfertile, as well as naturally conceived (sub-NC) versus
IVF/ICSI.
The main focus lies on subfertile couples who conceived naturally,
Additionally, ‘IVF/ICSI’ was analyzed to see whether ART was associated with
specific congenital anomalies. Furthermore, an attempt was made to analyze a
possible association between TTP and specific congenital anomalies. To this end, TTP
was divided into TTP < 2 years and TTP ≥ 2 years.
4.5 Statistical analysis
Since the controls that were used are mainly comprised of chromosomal anomalies,
which are known to be overrepresented in women of increased age at conception,
maternal age at conception is used as a confounder, even in the ‘crude’ analysis. To
estimate the risk for congenital anomalies, the ‘crude’ odds ratios (ORs) were
calculated first by using a ‘multivariate’ logistic regression with only maternal age at
conception as confounder. In the model, the fertility status in two or three categories
was the main independent variable and the different subgroups of congenital
anomalies were the dependent variables. Confirmed fertile participants were used as
reference category in the fertility status analyses. In the TTP analyses TTP < 2 years
was used as reference category.
To explore the contribution of the potential confounders, multivariate logistic
regression to calculate adjusted ORs was used. Apart from maternal age at
conception, potential confounders included pregnancy outcome, infant sex, education
of the mother, smoking, folic acid use, body mass index (BMI), diabetes mellitus,
parity, number of children in this pregnancy and a history of another pregnancy
affected by congenital anomalies.
To allow the level of education of the mother in question to be taken into
consideration as a possible factor influencing the outcome of the pregnancy, the level

12
of education was subdivided into a number of categories. Subsequently, the maternal
level of education was noted as either low, middle or high. The definition for low
level of education was primary school, lower general secondary education and lower
vocational education. Middle level education was defined as higher general secondary
education and intermediate vocational education. Those mothers who had a higher
vocational education, university degree or studied at a further tertiary college were
grouped among those with a high level of education.
Certain habits, such as smoking, could have an impact on the odds of giving
birth to a child suffering from birth defects. The mothers, who were included in this
study, were divided into the groups smoking or non-smoking during pregnancy. When
a woman was placed in the smoking category, this implies either smoking during
pregnancy, the mother has smoked but stopped at the moment she knew she was
pregnant, smoked only at the end of pregnancy or smoked but the exact period in
which the mother has smoked is unknown. In contrast, to be placed in the non-
smoking category implies that the mother either smoked but stopped before she
became pregnant or was a non-smoker.
The BMI classification of the World Health Organization (WHO) was used:
underweight (BMI < 18.50 kg/m2), normal weight (BMI 18.50 – 24.99 kg/m
2) and
overweight (BMI > 25 kg/m2)(35).
For counteracting the problem of multiple comparisons in statistical analyses,
the Bonferroni correction could have been used. Since this study is an explorative
research it was decided to not correct for multiple testing. Not correcting for multiple
testing in explorative research is widely accepted(36).Therefore, a p-value of less than
0.05 and 95% confidence interval (CI) excluding 1.00 was considered to be
statistically significant. Statistical analyses were performed using IBM SPSS Statistics
20.
13
5 Results
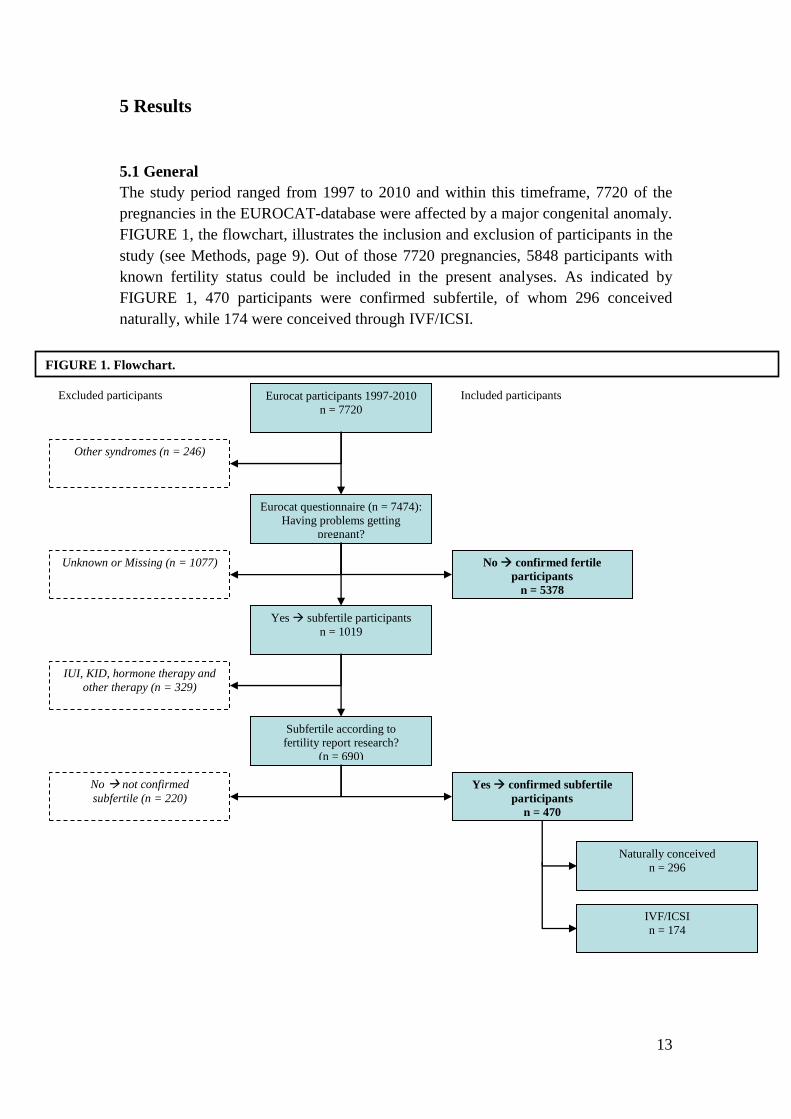
5.1 General
The study period ranged from 1997 to 2010 and within this timeframe, 7720 of the
pregnancies in the EUROCAT-database were affected by a major congenital anomaly.
FIGURE 1, the flowchart, illustrates the inclusion and exclusion of participants in the
study (see Methods, page 9). Out of those 7720 pregnancies, 5848 participants with
known fertility status could be included in the present analyses. As indicated by
FIGURE 1, 470 participants were confirmed subfertile, of whom 296 conceived
naturally, while 174 were conceived through IVF/ICSI.
Eurocat participants 1997-2010
n = 7720
Eurocat questionnaire (n = 7474):
Having problems getting
pregnant?
Other syndromes (n = 246)
Unknown or Missing (n = 1077) No confirmed fertile
participants
n = 5378
Yes subfertile participants
n = 1019
IUI, KID, hormone therapy and
other therapy (n = 329)
Subfertile according to
fertility report research?
(n = 690)
No not confirmed
subfertile (n = 220)
Yes confirmed subfertile
participants
n = 470
Naturally conceived
n = 296
IVF/ICSI
n = 174
Excluded participants Included participants
FIGURE 1. Flowchart.
14
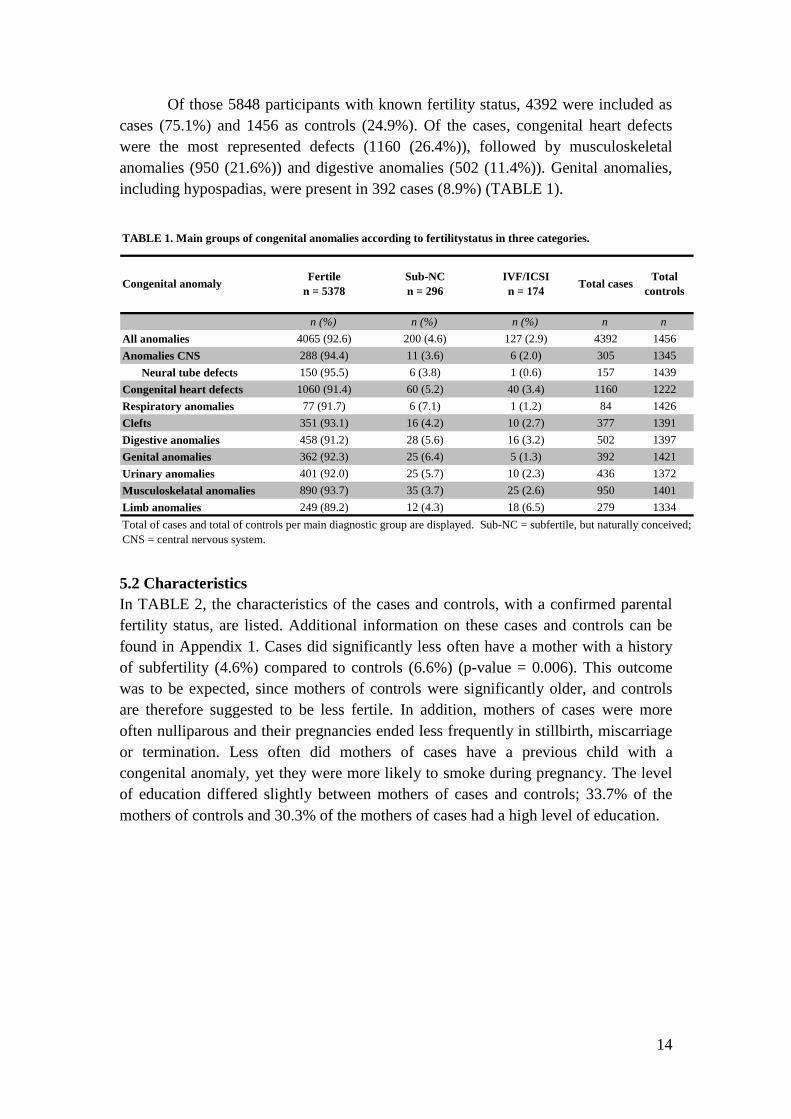
Of those 5848 participants with known fertility status, 4392 were included as
cases (75.1%) and 1456 as controls (24.9%). Of the cases, congenital heart defects
were the most represented defects (1160 (26.4%)), followed by musculoskeletal
anomalies (950 (21.6%)) and digestive anomalies (502 (11.4%)). Genital anomalies,
including hypospadias, were present in 392 cases (8.9%) (TABLE 1).
n (%) n (%) n (%) n n
All anomalies 4065 (92.6) 200 (4.6) 127 (2.9) 4392 1456
Anomalies CNS 288 (94.4) 11 (3.6) 6 (2.0) 305 1345
Neural tube defects 150 (95.5) 6 (3.8) 1 (0.6) 157 1439
Congenital heart defects 1060 (91.4) 60 (5.2) 40 (3.4) 1160 1222
Respiratory anomalies 77 (91.7) 6 (7.1) 1 (1.2) 84 1426
Clefts 351 (93.1) 16 (4.2) 10 (2.7) 377 1391
Digestive anomalies 458 (91.2) 28 (5.6) 16 (3.2) 502 1397
Genital anomalies 362 (92.3) 25 (6.4) 5 (1.3) 392 1421
Urinary anomalies 401 (92.0) 25 (5.7) 10 (2.3) 436 1372
Musculoskelatal anomalies 890 (93.7) 35 (3.7) 25 (2.6) 950 1401
Limb anomalies 249 (89.2) 12 (4.3) 18 (6.5) 279 1334
Total of cases and total of controls per main diagnostic group are displayed. Sub-NC = subfertile, but naturally conceived;
CNS = central nervous system.
TABLE 1. Main groups of congenital anomalies according to fertilitystatus in three categories.
Total casesTotal
controlsCongenital anomaly
Fertile
n = 5378
Sub-NC
n = 296
IVF/ICSI
n = 174
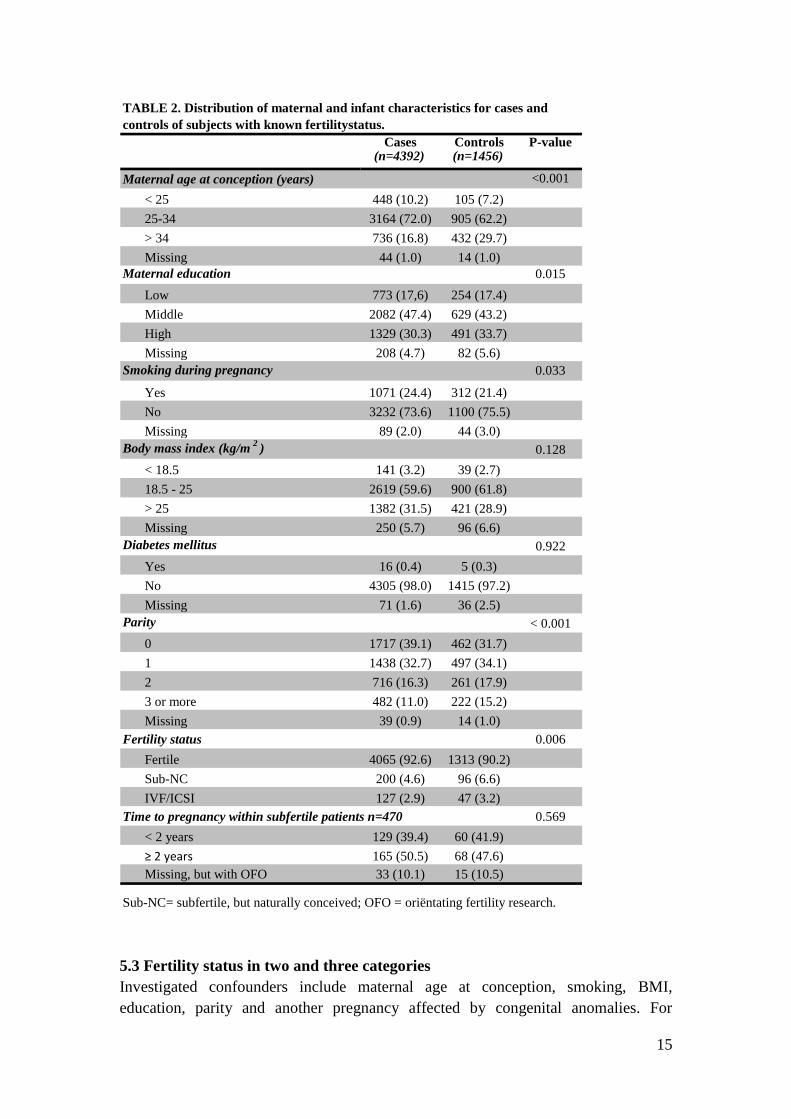
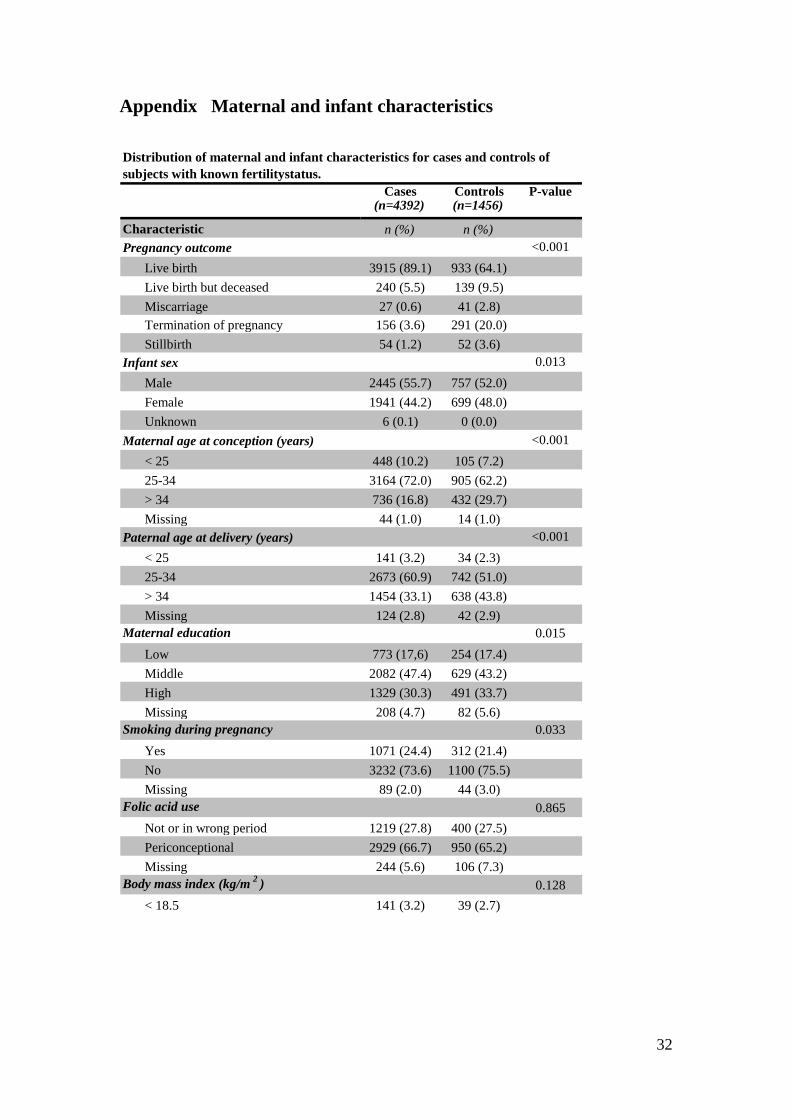
5.2 Characteristics
In TABLE 2, the characteristics of the cases and controls, with a confirmed parental
fertility status, are listed. Additional information on these cases and controls can be
found in Appendix 1. Cases did significantly less often have a mother with a history
of subfertility (4.6%) compared to controls (6.6%) (p-value = 0.006). This outcome
was to be expected, since mothers of controls were significantly older, and controls
are therefore suggested to be less fertile. In addition, mothers of cases were more
often nulliparous and their pregnancies ended less frequently in stillbirth, miscarriage
or termination. Less often did mothers of cases have a previous child with a
congenital anomaly, yet they were more likely to smoke during pregnancy. The level
of education differed slightly between mothers of cases and controls; 33.7% of the
mothers of controls and 30.3% of the mothers of cases had a high level of education.
15
Cases Controls P-value(n=4392) (n=1456)
<0.001
< 25 448 (10.2) 105 (7.2)
25-34 3164 (72.0) 905 (62.2)
> 34 736 (16.8) 432 (29.7)
Missing 44 (1.0) 14 (1.0)
Maternal education 0.015
Low 773 (17,6) 254 (17.4)
Middle 2082 (47.4) 629 (43.2)
High 1329 (30.3) 491 (33.7)
Missing 208 (4.7) 82 (5.6)
Smoking during pregnancy 0.033
Yes 1071 (24.4) 312 (21.4)
No 3232 (73.6) 1100 (75.5)
Missing 89 (2.0) 44 (3.0)
Body mass index (kg/m2
) 0.128
< 18.5 141 (3.2) 39 (2.7)
18.5 - 25 2619 (59.6) 900 (61.8)
> 25 1382 (31.5) 421 (28.9)
Missing 250 (5.7) 96 (6.6)
Diabetes mellitus 0.922
Yes 16 (0.4) 5 (0.3)
No 4305 (98.0) 1415 (97.2)
Missing 71 (1.6) 36 (2.5)
Parity < 0.001
0 1717 (39.1) 462 (31.7)
1 1438 (32.7) 497 (34.1)
2 716 (16.3) 261 (17.9)
3 or more 482 (11.0) 222 (15.2)
Missing 39 (0.9) 14 (1.0)
Fertility status 0.006
Fertile 4065 (92.6) 1313 (90.2)
Sub-NC 200 (4.6) 96 (6.6)
IVF/ICSI 127 (2.9) 47 (3.2)
0.569
< 2 years 129 (39.4) 60 (41.9)
≥ 2 years 165 (50.5) 68 (47.6)
Missing, but with OFO 33 (10.1) 15 (10.5)
Time to pregnancy within subfertile patients n=470
Sub-NC= subfertile, but naturally conceived; OFO = oriëntating fertility research.
TABLE 2. Distribution of maternal and infant characteristics for cases and
controls of subjects with known fertilitystatus.
Maternal age at conception (years)
5.3 Fertility status in two and three categories
Investigated confounders include maternal age at conception, smoking, BMI,
education, parity and another pregnancy affected by congenital anomalies. For
16
anomalies of the central nervous system (CNS), neural tube defects and congenital
heart defects an additional adjustment for maternal pre-gestational diabetes has been
done, since it is a known risk factor for these anomalies(37). Smoking, education,
parity, a previous pregnancy affected by congenital anomalies and diabetes were
considered as categorical variables and maternal age and BMI as continuous
variables. Other variables that we did investigate, but were found to have no
confounding effect included pregnancy outcome, infant sex, folic acid use and number
of children in this pregnancy.
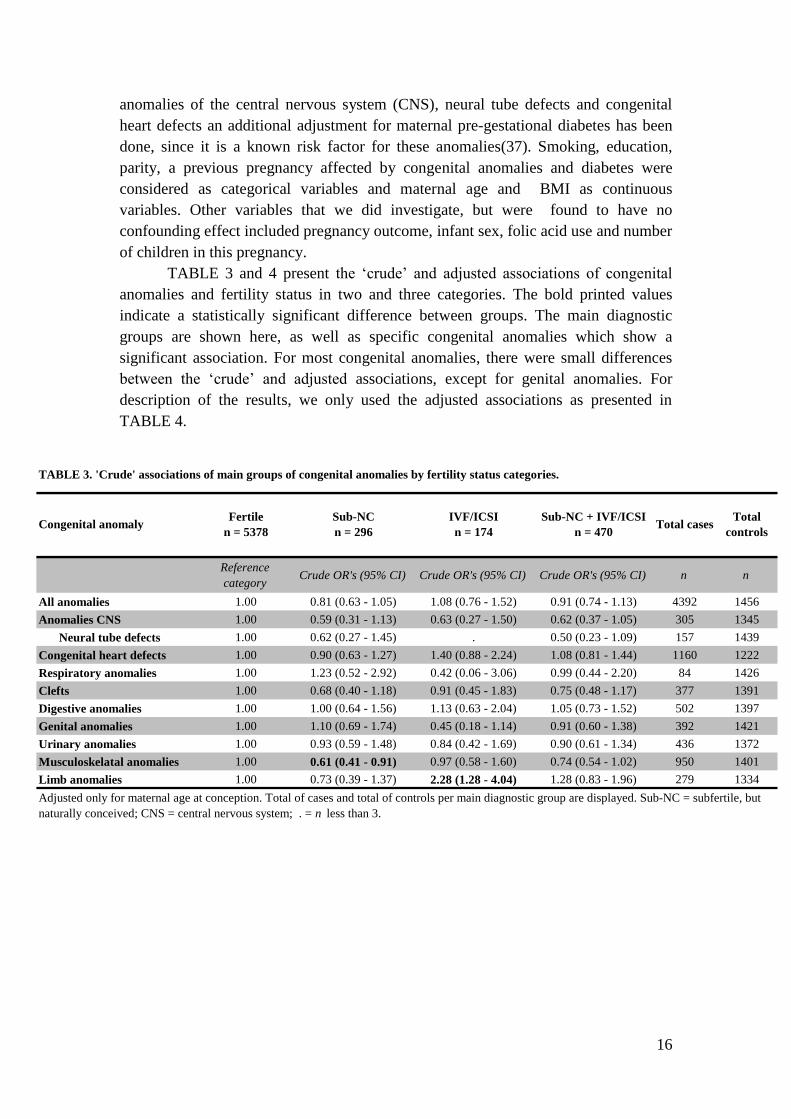
TABLE 3 and 4 present the ‘crude’ and adjusted associations of congenital
anomalies and fertility status in two and three categories. The bold printed values
indicate a statistically significant difference between groups. The main diagnostic
groups are shown here, as well as specific congenital anomalies which show a
significant association. For most congenital anomalies, there were small differences
between the ‘crude’ and adjusted associations, except for genital anomalies. For
description of the results, we only used the adjusted associations as presented in
TABLE 4.
Reference
categoryCrude OR's (95% CI) Crude OR's (95% CI) Crude OR's (95% CI) n n
All anomalies 1.00 0.81 (0.63 - 1.05) 1.08 (0.76 - 1.52) 0.91 (0.74 - 1.13) 4392 1456
Anomalies CNS 1.00 0.59 (0.31 - 1.13) 0.63 (0.27 - 1.50) 0.62 (0.37 - 1.05) 305 1345
Neural tube defects 1.00 0.62 (0.27 - 1.45) . 0.50 (0.23 - 1.09) 157 1439
Congenital heart defects 1.00 0.90 (0.63 - 1.27) 1.40 (0.88 - 2.24) 1.08 (0.81 - 1.44) 1160 1222
Respiratory anomalies 1.00 1.23 (0.52 - 2.92) 0.42 (0.06 - 3.06) 0.99 (0.44 - 2.20) 84 1426
Clefts 1.00 0.68 (0.40 - 1.18) 0.91 (0.45 - 1.83) 0.75 (0.48 - 1.17) 377 1391
Digestive anomalies 1.00 1.00 (0.64 - 1.56) 1.13 (0.63 - 2.04) 1.05 (0.73 - 1.52) 502 1397
Genital anomalies 1.00 1.10 (0.69 - 1.74) 0.45 (0.18 - 1.14) 0.91 (0.60 - 1.38) 392 1421
Urinary anomalies 1.00 0.93 (0.59 - 1.48) 0.84 (0.42 - 1.69) 0.90 (0.61 - 1.34) 436 1372
Musculoskelatal anomalies 1.00 0.61 (0.41 - 0.91) 0.97 (0.58 - 1.60) 0.74 (0.54 - 1.02) 950 1401
Limb anomalies 1.00 0.73 (0.39 - 1.37) 2.28 (1.28 - 4.04) 1.28 (0.83 - 1.96) 279 1334
Adjusted only for maternal age at conception. Total of cases and total of controls per main diagnostic group are displayed. Sub-NC = subfertile, but
naturally conceived; CNS = central nervous system; . = n less than 3.
Total casesTotal
controls
TABLE 3. 'Crude' associations of main groups of congenital anomalies by fertility status categories.
Sub-NC + IVF/ICSI
n = 470Congenital anomaly
Fertile
n = 5378
Sub-NC
n = 296
IVF/ICSI
n = 174
17
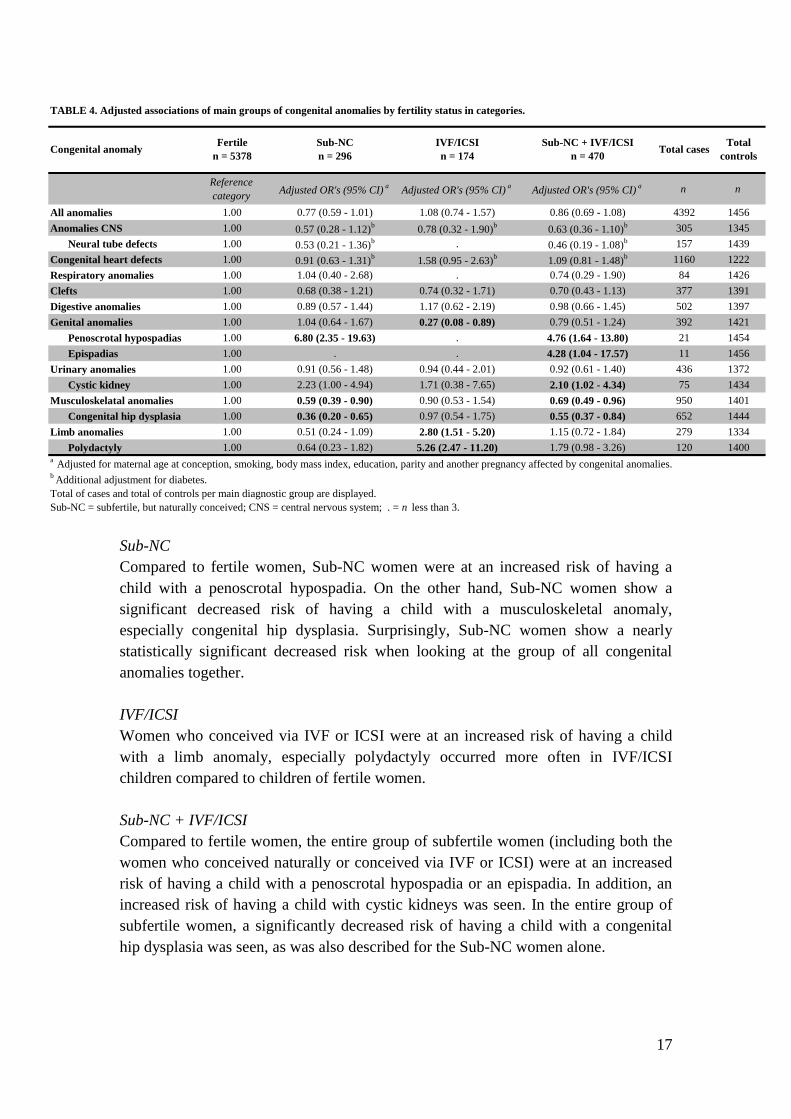
Sub-NC
Compared to fertile women, Sub-NC women were at an increased risk of having a
child with a penoscrotal hypospadia. On the other hand, Sub-NC women show a
significant decreased risk of having a child with a musculoskeletal anomaly,
especially congenital hip dysplasia. Surprisingly, Sub-NC women show a nearly
statistically significant decreased risk when looking at the group of all congenital
anomalies together.
IVF/ICSI
Women who conceived via IVF or ICSI were at an increased risk of having a child
with a limb anomaly, especially polydactyly occurred more often in IVF/ICSI
children compared to children of fertile women.
Sub-NC + IVF/ICSI
Compared to fertile women, the entire group of subfertile women (including both the
women who conceived naturally or conceived via IVF or ICSI) were at an increased
risk of having a child with a penoscrotal hypospadia or an epispadia. In addition, an
increased risk of having a child with cystic kidneys was seen. In the entire group of
subfertile women, a significantly decreased risk of having a child with a congenital
hip dysplasia was seen, as was also described for the Sub-NC women alone.
Reference
categoryAdjusted OR's (95% CI)
aAdjusted OR's (95% CI)
aAdjusted OR's (95% CI)
a n n
All anomalies 1.00 0.77 (0.59 - 1.01) 1.08 (0.74 - 1.57) 0.86 (0.69 - 1.08) 4392 1456
Anomalies CNS 1.00 0.57 (0.28 - 1.12)b
0.78 (0.32 - 1.90)b
0.63 (0.36 - 1.10)b 305 1345
Neural tube defects 1.00 0.53 (0.21 - 1.36)b . 0.46 (0.19 - 1.08)
b 157 1439
Congenital heart defects 1.00 0.91 (0.63 - 1.31)b
1.58 (0.95 - 2.63)b
1.09 (0.81 - 1.48)b 1160 1222
Respiratory anomalies 1.00 1.04 (0.40 - 2.68) . 0.74 (0.29 - 1.90) 84 1426
Clefts 1.00 0.68 (0.38 - 1.21) 0.74 (0.32 - 1.71) 0.70 (0.43 - 1.13) 377 1391
Digestive anomalies 1.00 0.89 (0.57 - 1.44) 1.17 (0.62 - 2.19) 0.98 (0.66 - 1.45) 502 1397
Genital anomalies 1.00 1.04 (0.64 - 1.67) 0.27 (0.08 - 0.89) 0.79 (0.51 - 1.24) 392 1421
Penoscrotal hypospadias 1.00 6.80 (2.35 - 19.63) . 4.76 (1.64 - 13.80) 21 1454
Epispadias 1.00 . . 4.28 (1.04 - 17.57) 11 1456
Urinary anomalies 1.00 0.91 (0.56 - 1.48) 0.94 (0.44 - 2.01) 0.92 (0.61 - 1.40) 436 1372
Cystic kidney 1.00 2.23 (1.00 - 4.94) 1.71 (0.38 - 7.65) 2.10 (1.02 - 4.34) 75 1434
Musculoskelatal anomalies 1.00 0.59 (0.39 - 0.90) 0.90 (0.53 - 1.54) 0.69 (0.49 - 0.96) 950 1401
Congenital hip dysplasia 1.00 0.36 (0.20 - 0.65) 0.97 (0.54 - 1.75) 0.55 (0.37 - 0.84) 652 1444
Limb anomalies 1.00 0.51 (0.24 - 1.09) 2.80 (1.51 - 5.20) 1.15 (0.72 - 1.84) 279 1334
Polydactyly 1.00 0.64 (0.23 - 1.82) 5.26 (2.47 - 11.20) 1.79 (0.98 - 3.26) 120 1400
TABLE 4. Adjusted associations of main groups of congenital anomalies by fertility status in categories.
Congenital anomalyFertile
n = 5378
Sub-NC
n = 296
IVF/ICSI
n = 174
a Adjusted for maternal age at conception, smoking, body mass index, education, parity and another pregnancy affected by congenital anomalies.
b Additional adjustment for diabetes.
Total of cases and total of controls per main diagnostic group are displayed.
Sub-NC = subfertile, but naturally conceived; CNS = central nervous system; . = n less than 3.
Sub-NC + IVF/ICSI
n = 470Total cases
Total
controls
18
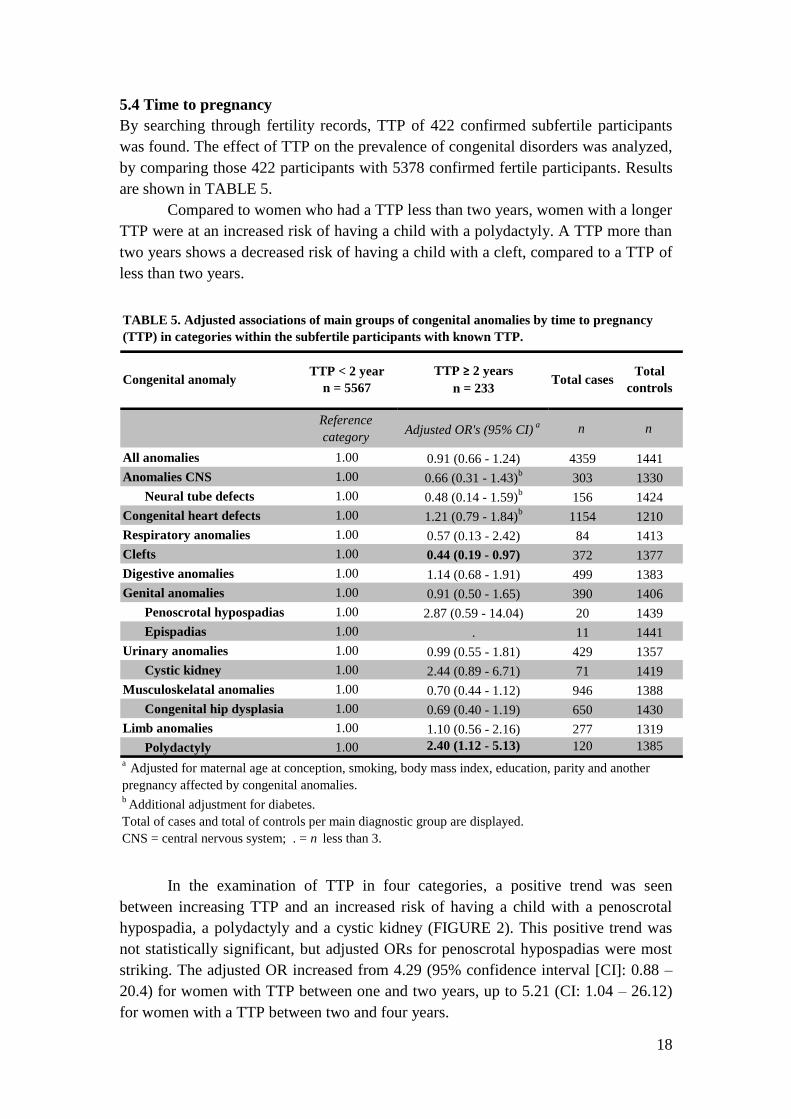
5.4 Time to pregnancy
By searching through fertility records, TTP of 422 confirmed subfertile participants
was found. The effect of TTP on the prevalence of congenital disorders was analyzed,
by comparing those 422 participants with 5378 confirmed fertile participants. Results
are shown in TABLE 5.
Compared to women who had a TTP less than two years, women with a longer
TTP were at an increased risk of having a child with a polydactyly. A TTP more than
two years shows a decreased risk of having a child with a cleft, compared to a TTP of
less than two years.
Reference
categoryAdjusted OR's (95% CI)
a n n
All anomalies 1.00 0.91 (0.66 - 1.24) 4359 1441
Anomalies CNS 1.00 0.66 (0.31 - 1.43)b
303 1330
Neural tube defects 1.00 0.48 (0.14 - 1.59)b
156 1424
Congenital heart defects 1.00 1.21 (0.79 - 1.84)b
1154 1210
Respiratory anomalies 1.00 0.57 (0.13 - 2.42) 84 1413
Clefts 1.00 0.44 (0.19 - 0.97) 372 1377
Digestive anomalies 1.00 1.14 (0.68 - 1.91) 499 1383
Genital anomalies 1.00 0.91 (0.50 - 1.65) 390 1406
Penoscrotal hypospadias 1.00 2.87 (0.59 - 14.04) 20 1439
Epispadias 1.00 . 11 1441
Urinary anomalies 1.00 0.99 (0.55 - 1.81) 429 1357
Cystic kidney 1.00 2.44 (0.89 - 6.71) 71 1419
Musculoskelatal anomalies 1.00 0.70 (0.44 - 1.12) 946 1388
Congenital hip dysplasia 1.00 0.69 (0.40 - 1.19) 650 1430
Limb anomalies 1.00 1.10 (0.56 - 2.16) 277 1319
Polydactyly 1.00 2.40 (1.12 - 5.13) 120 1385
a Adjusted for maternal age at conception, smoking, body mass index, education, parity and another
pregnancy affected by congenital anomalies. b
Additional adjustment for diabetes.
Total of cases and total of controls per main diagnostic group are displayed.
CNS = central nervous system; . = n less than 3.
Total casesTotal
controls
TABLE 5. Adjusted associations of main groups of congenital anomalies by time to pregnancy
(TTP) in categories within the subfertile participants with known TTP.
Congenital anomalyTTP < 2 year
n = 5567
TTP ≥ 2 years
n = 233
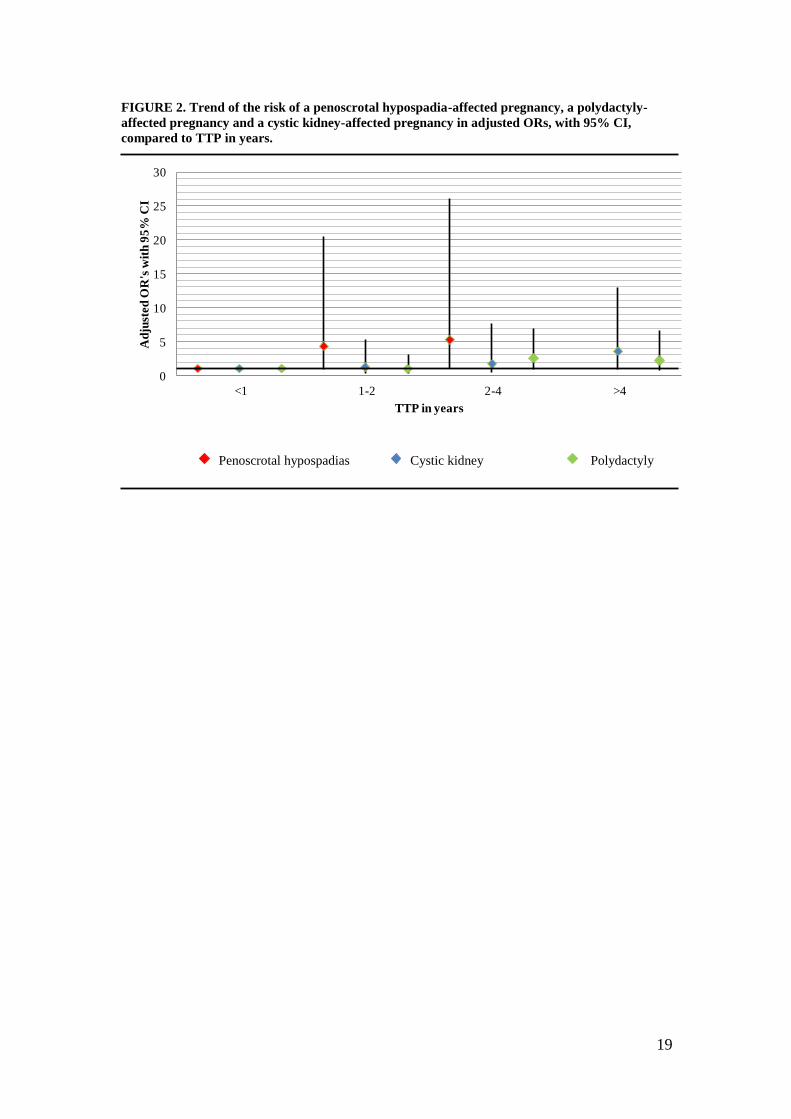
In the examination of TTP in four categories, a positive trend was seen
between increasing TTP and an increased risk of having a child with a penoscrotal
hypospadia, a polydactyly and a cystic kidney (FIGURE 2). This positive trend was
not statistically significant, but adjusted ORs for penoscrotal hypospadias were most
striking. The adjusted OR increased from 4.29 (95% confidence interval [CI]: 0.88 –
20.4) for women with TTP between one and two years, up to 5.21 (CI: 1.04 – 26.12)
for women with a TTP between two and four years.
19
FIGURE 2. Trend of the risk of a penoscrotal hypospadia-affected pregnancy, a polydactyly-
affected pregnancy and a cystic kidney-affected pregnancy in adjusted ORs, with 95% CI,
compared to TTP in years.
0
5
10
15
20
25
30
<1 1-2 2-4 >4
Ad
just
ed
OR
's w
ith
95
% C
I
TTP in years
Penoscrotal hypospadias Cystic kidney Polydactyly

20
6 Discussion
6.1 Main results
In this study, the question was addressed whether a history of subfertility, with or
without IVF/ICSI treatment, affects the risk of having a child with a specific
congenital anomaly. It was shown that subfertility is associated with an increased risk
of several congenital anomalies in naturally conceived offspring in subfertile women,
as well as in offspring conceived via IVF or ICSI. The most striking result was the
increased risk found in subfertile women who conceived naturally: they had a higher
risk of having a child with a penoscrotal hypospadia. Sub-NC women also were at
increased risk of having a child with an epispadia. In women who conceived via IVF
or ICSI we found an increased risk of having a child with a limb anomaly, especially
polydactyly occurred more often in this group. The total group of subfertile
participants (Sub-NC + IVF/ICSI) showed an increased risk of having a child with a
cystic kidney, compared to fertile women. We also found an association between
increased TTP (>2 years) and polydactyly. In addition, increased TTP showed a
positive trend for the risk of a pregnancy affected with a penoscrotal hypospadia, a
polydactyly, and a cystic kidney, but these trends were not statistically significant.
On the other hand, we found a decreased risk of having a child with a
congenital hip dysplasia in Sub-NC women. We also found a decreased risk of having
a child with a cleft in women with a TTP of more than two years, compared to women
with a TTP less than two years.
Comparison with the literature
Some of the results are in line with the literature, whereas others are not. First, in
accordance with Zhu et al., Ghazi et al. and Seggers et al., the present study showed
some evidence for an adverse effect of subfertility. That underlying subfertility played
a part in increasing birth defect rates was suggested by Ghazi et al. in a large Swedish
case-control study. They reported higher rates of congenital anomalies after a history
of subfertility of at least four years(29). Zhu et al. (2006) confirmed that a history of
subfertility without assisted conception is strongly associated with birth defects and
they described a high hazard ratio for congenital anomalies in subfertile couples who
conceived naturally, compared to fertile couples, in a large Danish national birth
cohort(30). Zhu et al. also described an increased prevalence of genital organ
malformations in babies born after ART compared with babies conceived naturally.
Others also repeatedly described that singletons born following IVF/ICSI have a
higher prevalence of congenital malformations, including hypospadias, compared to
singletons conceived naturally. Hypospadia is the only congenital anomaly which
consistently shows a different risk rate among different ART procedures in different
studies: the risk is slightly increased in children conceived via ICSI compared to IVF.
The authors of the studies suggested that this discrepancy could be the result of a
genetic link with paternal subfertility, rather than with the ICSI procedure per
21
se(22,25-27). Within the present study this comparison between IVF and ICSI was not
made, since numbers were too low. A higher risk for penoscrotal hypospadias in the
Sub-NC group was found, suggesting a role of the underlying subfertility instead of
the ART procedures.
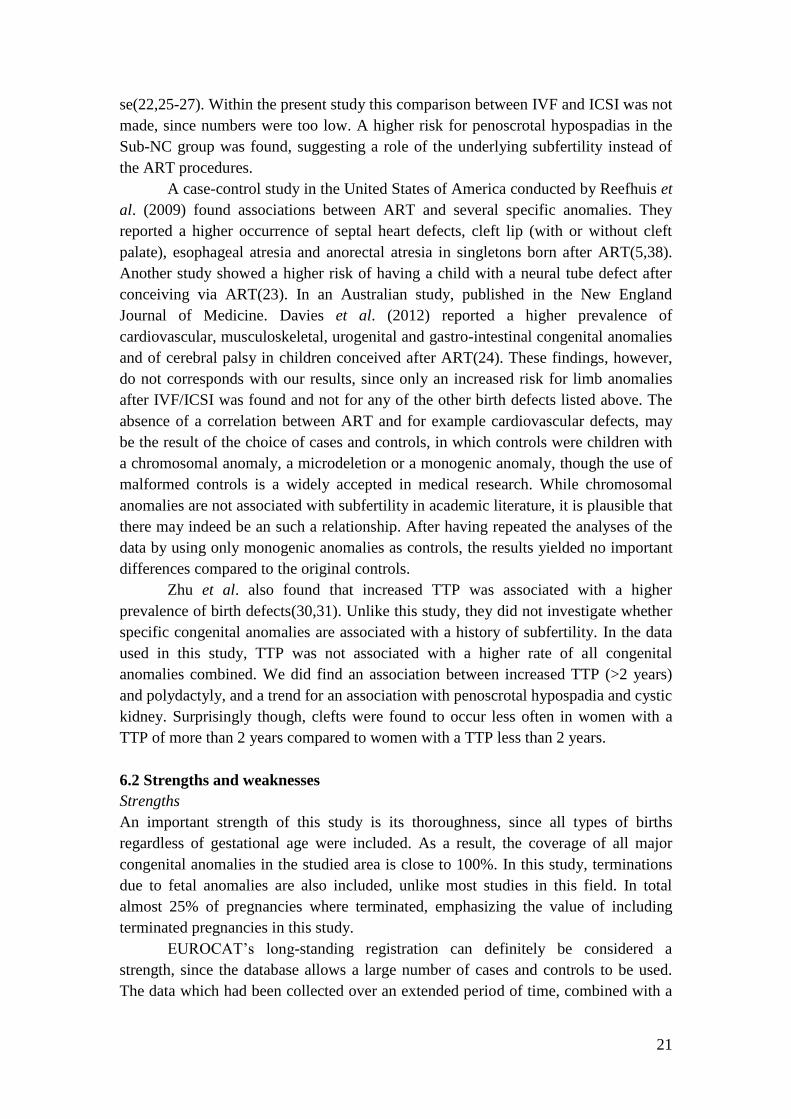
A case-control study in the United States of America conducted by Reefhuis et
al. (2009) found associations between ART and several specific anomalies. They
reported a higher occurrence of septal heart defects, cleft lip (with or without cleft
palate), esophageal atresia and anorectal atresia in singletons born after ART(5,38).
Another study showed a higher risk of having a child with a neural tube defect after
conceiving via ART(23). In an Australian study, published in the New England
Journal of Medicine. Davies et al. (2012) reported a higher prevalence of
cardiovascular, musculoskeletal, urogenital and gastro-intestinal congenital anomalies
and of cerebral palsy in children conceived after ART(24). These findings, however,
do not corresponds with our results, since only an increased risk for limb anomalies
after IVF/ICSI was found and not for any of the other birth defects listed above. The
absence of a correlation between ART and for example cardiovascular defects, may
be the result of the choice of cases and controls, in which controls were children with
a chromosomal anomaly, a microdeletion or a monogenic anomaly, though the use of
malformed controls is a widely accepted in medical research. While chromosomal
anomalies are not associated with subfertility in academic literature, it is plausible that
there may indeed be an such a relationship. After having repeated the analyses of the
data by using only monogenic anomalies as controls, the results yielded no important
differences compared to the original controls.
Zhu et al. also found that increased TTP was associated with a higher
prevalence of birth defects(30,31). Unlike this study, they did not investigate whether
specific congenital anomalies are associated with a history of subfertility. In the data
used in this study, TTP was not associated with a higher rate of all congenital
anomalies combined. We did find an association between increased TTP (>2 years)
and polydactyly, and a trend for an association with penoscrotal hypospadia and cystic
kidney. Surprisingly though, clefts were found to occur less often in women with a
TTP of more than 2 years compared to women with a TTP less than 2 years.
6.2 Strengths and weaknesses
Strengths
An important strength of this study is its thoroughness, since all types of births
regardless of gestational age were included. As a result, the coverage of all major
congenital anomalies in the studied area is close to 100%. In this study, terminations
due to fetal anomalies are also included, unlike most studies in this field. In total
almost 25% of pregnancies where terminated, emphasizing the value of including
terminated pregnancies in this study.
EUROCAT’s long-standing registration can definitely be considered a
strength, since the database allows a large number of cases and controls to be used.
The data which had been collected over an extended period of time, combined with a
22
parental questionnaire which is quite detailed, helped reveal a large collection of
variables which necessitated the adjustment of the analyses.
Likewise, another strength is the inclusion of children with congenital
anomalies up to the age of 10 years, since the vast majority of congenital anomalies is
detected before this age, meaning that the study covered most of the occurring
congenital anomalies.
The chance of differential recall of information on confounders between
mothers of malformed and non-malformed children is greatly reduced by selecting
malformed controls rather than seemingly healthy controls. Therefore, the use of
malformed controls can also be considered one of the strengths of this study.
Furthermore, this study is the first case-control study investigating whether
specific congenital anomalies are associated with a history of subfertility. Finally, we
were able to objectify fertility status by searching fertility records.
Weaknesses
A possible limitation is that data on fertility status and other determinants were
collected retrospectively, which means that recall bias may pose a problem, though of
the parental questionnaires 60% was returned before the child was aged two years.
The need to objectify the fertility status of participants by a fertility record search
resulted in loss of data, as participants with unconfirmed subfertility were excluded.
The loss of these data did reduce study power, but it is unlikely that a reduced data
input introduced bias. Parents who indicated that they did not have trouble conceiving
this pregnancy could however be subfertile according to our definition (TTP>1 year),
yet felt they conceived without a problem. These couples were included in the
analyses as ‘fertile couples’. Subfertile couples could subsequently be placed in the
‘fertile couples’ group. Due to this classification, there could have been an
underestimation of the effect of subfertility may have on the presence of congenital
anomalies occurring in offspring.
Finally, we only had relatively small numbers for the analysis on TTP, despite
the large size of the original study population. As a consequence, our study had
limited statistical power to evaluate an effect of increased TTP on specific congenital
abnormalities.
6.3 Potential underlying mechanisms
We found a large disparity between the characteristics of the mothers and infant of
both the cases and controls, particularly with regard to pregnancy outcomes, maternal
age, maternal education, parity, smoking and a history of pregnancies affected by a
congenital anomaly. An explanation of these differences in maternal characteristics is
the fact that prevalence of chromosomal anomalies, the largest number of our
controls, is higher in elderly women(39,40).
One matter in particular still remains unclear, which is the exact mechanism
behind subfertility leading to congenital anomalies, particularly hypospadias, in
fetuses. In academic literature an association between the use of diethylstilbestrol
(DES) in mothers and hypospadia in their offspring is described(41). Human exposure

23
to DES occurred through diverse sources, such as dietary ingestion from
supplemented cattle feed as well as medical treatment for certain conditions, including
breast and prostate cancers. From around 1940 to 1970, DES was given to pregnant
women in the mistaken belief it would reduce the risk of pregnancy complications and
miscarriages. DES use in mothers is known to affect fertility negatively in their
offspring. The association between DES use in mothers and fertility problems in DES-
daughters might be a clarifying mechanism for the possible association between
subfertile DES-daugthers and hypospadia in their sons.
The data show a decreased risk for the entire group consisting of all congenital
anomalies in women with a history of subfertility compared to fertile women.
Although the association is not statistically significant, these findings do, in fact,
contradict academic sources. A possible underlying mechanism explaining the
findings is the change of lifestyle in couples with subfertility problems. It can be
assumed that couples who are trying to conceive for a longer period are trying to
change their lifestyle, such as using folic acid. Another possible explanation for the
findings is the diversity in underlying causes of subfertility in our data. Examples of
underlying causes of subfertility in our data are sperm abnormalities (genetic quality
of the sperm, as well as its volume and motility), hormonal dysregulation,
endometriosis, uterine problems and subfertility with unknown cause. Since all
different causes were grouped together, it was impossible to specify which underlying
cause is responsible for a particular congenital anomaly. As such, there is no clear
insight into the relationship between subfertility and congenital anomalies .
6.4 Further research
More research is necessary to investigate the possible biological mechanisms
clarifying the association between subfertility and hypospadias and other congenital
anomalies. It will be important to determine which mechanisms may cause a higher
risk of having a child with a polydactyly after conceiving via IVF or ICSI.
To investigate whether there is a possible association between a history of
subfertility and the occurrence of chromosomal anomalies, microdeletion anomalies
or monogenic anomalies it is highly recommended to have this study repeated with
non-malformed controls. It will likewise be advisable to replicate this study with
larger numbers in the TTP>2 years category, since a positive but non-significant trend
was observed between increased TTP and a higher risk of a penoscrotal hypospadia-
affected pregnancy, a polydactyly-affected pregnancy and a cystic kidney-affected
pregnancy.
Another recommendation for further research is the possibility that DES use
in grandmothers could act as a mechanism, indicating an association between
subfertile DES-daughters and their offspring with a hypospadia.
Finally, it would be interesting to conduct further research into whether
anorectal malformations, especially VACTERL association, is due to ART procedures
or caused by the underlying subfertility instead(42).

24
6.5 Public health implications
Before this study was conducted, it was unclear whether a history of subfertility is
associated with specific types of birth defects. Only the risk for a penoscrotal
hypospadia appears to be higher in the Sub-NC group. This is a reassuring finding
which is of importance for correct counseling of subfertile couples and may be useful
for (extended) prenatal screening in the future.
6.6 Conclusion
From all the research that had been collected, this study appears to be the first to
examine associations between specific congenital anomalies and a history of
subfertility. Our study partly confirm the hypothesis that women with a history of
subfertility are at an increased risk of giving birth to a child with a specific major
congenital anomaly, namely a penoscrotal hypospadia. For identifying possible
mechanisms which cause the increased risk of hypospadias, further research is
recommended. The results of this study may be of importance for public health, since
subfertility is a growing health issue since women are conceiving at older ages.
25
7 Acknowledgments
In conducting my research, analyzing the data, drafting and finally writing this thesis,
I am greatly indebted to a number of people, for whom I would like to use this
opportunity to show them my deep gratitude.
I wish to thank Hermien de Walle, for her help in planning this research and
for her limitless support. Without her warm support, I doubt whether I would have
been able to finish this research and write my thesis. I would also like to thank
Annemieke Hoek and Maaike Haadsma for helping me to brainstorm on the contents
of this study. My thanks also go to Jorien Seggers for her contributions to the content
of the study, I also wish to thank her for helping me to collect the data. I am much
obliged to Nicole Siemensma, Lies ter Beek and Jorieke van Kammen, for their help
finding answers to some difficult questions, their advice in drafting a proper letter to
send to hospitals and for the classification of some cases. For enabling this research, I
am indebted to Marian Bakker, registry leader of EUROCAT Northern Netherlands
department. Finally, my special thanks go to the whole EUROCAT team for the warm
welcome.
Marly Bos
18-01-2013
26
8 References
(1) Flenady V, Middleton P, Smith GC, Duke W, Erwich JJ, Khong TY, et al. Stillbirths: the
way forward in high-income countries. Lancet 2011 May 14;377(9778):1703-1717.
(2) Up To Date Approach to congenital malformations. Available at:
http://www.uptodate.com/contents/approach-to-congenital-
malformations?source=search_result&search=congenital+anomalies&selectedTitle=1%7E15
0.
(3) Eurocat Northern Netherlands. Available at:
http://www.rug.nl/umcg/faculteit/disciplinegroepen/medischegenetica/eurocat/AlgemeneCijfe
rsTabel1tm4.pdf.
(4) Juul S, Karmaus W, Olsen J. Regional differences in waiting time to pregnancy:
pregnancy-based surveys from Denmark, France, Germany, Italy and Sweden. The European
Infertility and Subfecundity Study Group. Hum Reprod 1999 May;14(5):1250-1254.
(5) International Committee for Monitoring Assisted Reproductive Technology, Adamson
GD, de Mouzon J, Lancaster P, Nygren KG, Sullivan E, et al. World collaborative report on
in vitro fertilization, 2000. Fertil Steril 2006 Jun;85(6):1586-1622.
(6) Nyboe Andersen A, Goossens V, Bhattacharya S, Ferraretti AP, Kupka MS, de Mouzon J,
et al. Assisted reproductive technology and intrauterine inseminations in Europe, 2005: results
generated from European registers by ESHRE: ESHRE. The European IVF Monitoring
Programme (EIM), for the European Society of Human Reproduction and Embryology
(ESHRE). Hum Reprod 2009 Jun;24(6):1267-1287.
(7) Reefhuis J, Honein MA, Schieve LA, Correa A, Hobbs CA, Rasmussen SA, et al. Assisted
reproductive technology and major structural birth defects in the United States. Hum Reprod
2009 Feb;24(2):360-366.
(8) Jolly M, Sebire N, Harris J, Robinson S, Regan L. The risks associated with pregnancy in
women aged 35 years or older. Hum Reprod 2000 Nov;15(11):2433-2437.
(9) Nygren KG, Finnstrom O, Kallen B, Olausson PO. Population-based Swedish studies of
outcomes after in vitro fertilisation. Acta Obstet Gynecol Scand 2007;86(7):774-782.
(10) Kallen B, Finnstrom O, Nygren KG, Otterblad Olausson P. In vitro fertilization in
Sweden: maternal characteristics. Acta Obstet Gynecol Scand 2005 Dec;84(12):1185-1191.
(11) Helmerhorst FM, Perquin DA, Donker D, Keirse MJ. Perinatal outcome of singletons
and twins after assisted conception: a systematic review of controlled studies. BMJ 2004 Jan
31;328(7434):261.
(12) Jackson RA, Gibson KA, Wu YW, Croughan MS. Perinatal outcomes in singletons
following in vitro fertilization: a meta-analysis. Obstet Gynecol 2004 Mar;103(3):551-563.

27
(13) Up To Date In vitro fertilization. Available at: http://www.uptodate.com.proxy-
ub.rug.nl/contents/in-vitro-
fertilization?source=search_result&search=IVF+and+ICSI&selectedTitle=2~150.
(14) Heineman MJ, Evers JLH, Massuger LFAG, Steegers EAP. Vruchtbaarheidsstoornissen.
Obstetrie en Gynaecologie: Elversier Gezondheidszorg; 2007. p. 647-682.
(15) Palermo G, Joris H, Devroey P, Van Steirteghem AC. Pregnancies after intracytoplasmic
injection of single spermatozoon into an oocyte. Lancet 1992 Jul 4;340(8810):17-18.
(16) Lanzendorf SE, Maloney MK, Veeck LL, Slusser J, Hodgen GD, Rosenwaks Z. A
preclinical evaluation of pronuclear formation by microinjection of human spermatozoa into
human oocytes. Fertil Steril 1988 May;49(5):835-842.
(17) Wennerholm UB, Soderstrom-Anttila V, Bergh C, Aittomaki K, Hazekamp J, Nygren
KG, et al. Children born after cryopreservation of embryos or oocytes: a systematic review of
outcome data. Hum Reprod 2009 Sep;24(9):2158-2172.
(18) Maheshwari A, Pandey S, Shetty A, Hamilton M, Bhattacharya S. Obstetric and perinatal
outcomes in singleton pregnancies resulting from the transfer of frozen thawed versus fresh
embryos generated through in vitro fertilization treatment: a systematic review and meta-
analysis. Fertil Steril 2012 Aug;98(2):368-77.e1-9.
(19) Schieve LA, Meikle SF, Ferre C, Peterson HB, Jeng G, Wilcox LS. Low and very low
birth weight in infants conceived with use of assisted reproductive technology. N Engl J Med
2002 Mar 7;346(10):731-737.
(20) Kallen B, Finnstrom O, Nygren KG, Olausson PO. In vitro fertilization in Sweden: child
morbidity including cancer risk. Fertil Steril 2005 Sep;84(3):605-610.
(21) Hansen M, Bower C, Milne E, de Klerk N, Kurinczuk JJ. Assisted reproductive
technologies and the risk of birth defects--a systematic review. Hum Reprod 2005
Feb;20(2):328-338.
(22) Hansen M, Kurinczuk JJ, Bower C, Webb S. The risk of major birth defects after
intracytoplasmic sperm injection and in vitro fertilization. N Engl J Med 2002 Mar
7;346(10):725-730.
(23) Kallen B, Finnstrom O, Nygren KG, Olausson PO. In vitro fertilization (IVF) in Sweden:
risk for congenital malformations after different IVF methods. Birth Defects Res A Clin Mol
Teratol 2005 Mar;73(3):162-169.
(24) Davies MJ, Moore VM, Willson KJ, Van Essen P, Priest K, Scott H, et al. Reproductive
technologies and the risk of birth defects. N Engl J Med 2012 May 10;366(19):1803-1813.
(25) Ericson A, Kallen B. Congenital malformations in infants born after IVF: a population-
based study. Hum Reprod 2001 Mar;16(3):504-509.
28
(26) Silver RI, Rodriguez R, Chang TS, Gearhart JP. In vitro fertilization is associated with an
increased risk of hypospadias. J Urol 1999 Jun;161(6):1954-1957.
(27) Wennerholm UB, Bergh C, Hamberger L, Lundin K, Nilsson L, Wikland M, et al.
Incidence of congenital malformations in children born after ICSI. Hum Reprod 2000
Apr;15(4):944-948.
(28) Draper ES, Kurinczuk JJ, Abrams KR, Clarke M. Assessment of separate contributions
to perinatal mortality of infertility history and treatment: a case-control analysis. Lancet 1999
May 22;353(9166):1746-1749.
(29) Ghazi HA, Spielberger C, Kallen B. Delivery outcome after infertility--a registry study.
Fertil Steril 1991 Apr;55(4):726-732.
(30) Zhu JL, Basso O, Obel C, Bille C, Olsen J. Infertility, infertility treatment, and
congenital malformations: Danish national birth cohort. BMJ 2006 Sep 30;333(7570):679.
(31) Seggers J, Haadsma ML, Bos AF, Heineman MJ, Keating P, Middelburg KJ, et al.
Dysmorphic features in 2-year-old IVF/ICSI offspring. Early Hum Dev 2012 Oct;88(10):823-
829.
(32) Eurocat Central Registry guidelines. Available at: http://www.eurocat-netwerk.eu/.
(33) Botto LD, Lin AE, Riehle-Colarusso T, Malik S, Correa A, National Birth Defects
Prevention Study. Seeking causes: Classifying and evaluating congenital heart defects in
etiologic studies. Birth Defects Res A Clin Mol Teratol 2007 Oct;79(10):714-727.
(34) Jentink J, Loane MA, Dolk H, Barisic I, Garne E, Morris JK, et al. Valproic acid
monotherapy in pregnancy and major congenital malformations. N Engl J Med 2010 Jun
10;362(23):2185-2193.
(35) WHO BMI. Available at: http://apps.who.int/bmi/index.jsp?introPage=intro_3.html.
(36) Streiner DL, Norman GR. Correction for multiple testing: is there a resolution? Chest
2011 Jul;140(1):16-18.
(37) Garne E, Loane M, Dolk H, Barisic I, Addor MC, Arriola L, et al. Spectrum of
congenital anomalies in pregnancies with pregestational diabetes. Birth Defects Res A Clin
Mol Teratol 2012 Mar;94(3):134-140.
(38) Reefhuis J, Honein MA, Schieve LA, Rasmussen SA, National Birth Defects Prevention
Study. Use of clomiphene citrate and birth defects, National Birth Defects Prevention Study,
1997-2005. Hum Reprod 2011 Feb;26(2):451-457.
(39) Hook EB. Rates of chromosome abnormalities at different maternal ages. Obstet Gynecol
1981 Sep;58(3):282-285.
29
(40) Up To Date Effect of advanced age on fertility and pregnancy in women. Available at:
http://www.uptodate.com/contents/effect-of-advanced-age-on-fertility-and-pregnancy-in-
women?source=search_result&search=Effect+of+advanced+age+on+fertility+and+pregnancy
+in+women+47&selectedTitle=1%7E150.
(41) Klip H, Verloop J, van Gool JD, Koster ME, Burger CW, van Leeuwen FE, et al.
Hypospadias in sons of women exposed to diethylstilbestrol in utero: a cohort study. Lancet
2002 Mar 30;359(9312):1102-1107.
(42) Zwink N, Jenetzky E, Schmiedeke E, Schmidt D, Marzheuser S, Grasshoff-Derr S, et al.
Assisted reproductive techniques and the risk of anorectal malformations: a German case-
control study. Orphanet J Rare Dis 2012 Sep 15;7(1):65.
30
9 Nederlandse samenvatting
Inleiding: In de literatuur is een toegenomen risico op het voorkomen van aangeboren
afwijkingen bij in vitro fertilisatie (IVF)- en intracytoplasmatische sperma injectie
(ICSI)- kinderen beschreven. Specifiek worden een toename van cardiovasculaire,
musculoskeletale, urogenitale en gastrointestinale afwijkingen gezien. Het is nog niet
bekend of deze toegenomen risico’s kunnen worden verklaard door patiënt
karakteristieken gerelateerd aan subfertiliteit, of aan de behandelingstechnieken op
zichzelf. Het primaire doel van de studie was om te evalueren of specifieke
aangeboren afwijkingen vaker voorkomen bij de kinderen van subfertiele paren, die
natuurlijk zwanger werden (Sub-NC) in vergelijking met de kinderen van fertiele
paren. Het secundaire doel was het evalueren of specifieke aangeboren afwijkingen
vaker (of minder vaak) voorkomen na natuurlijke conceptie bij subfertiliteit in
vergelijking met kinderen van paren die middels IVF/ICSI zwanger zijn geworden.
Het tertiaire doel was om te kijken of de ‘time to pregnancy’ (TTP) bij subfertiele
paren een positieve associatie laat zien met het voorkomen van specifieke aangeboren
afwijkingen.
Methode: 4392 cases en 1456 (aangedane) controles tussen 1997 en 2010 geboren,
waarvan informatie over de fertiliteitstatus van de moeder bekend was, werden uit de
EUROCAT registratie geïncludeerd. Cases waren kinderen en foetussen met major
aangeboren afwijkingen met een niet-genetische oorzaak. Controles waren
gedefinieerd als kinderen en foetussen met chromosomale afwijking, een microdeletie
of een monogene afwijking. Multivariate logistische regressie met de vergelijking
tussen drie groepen van kinderen en foetussen vond plaats: Sub-NC (n=296),
IVF/ICSI (n=174) en kinderen en foetussen van fertiele paren (n=5378). Mogelijke
confounders waren leeftijd van de moeder bij de conceptie, roken tijdens de
zwangerschap, ‘body mass index’ voor de zwangerschap, opleidingsniveau van de
moeder, pariteit, ander kind met een aangeboren afwijking en maternale diabetes.
Resultaten: We vonden een hoger risico voor Sub-NC vrouwen in vergelijking met
fertiele vrouwen op het krijgen van een kind met een penoscrotale hypospadie
(gecorrigeerde odds ratio [aOR]: 6.80; 95% confidence interval [CI]: 2.35 – 19.63).
Subfertiele vrouwen die zwanger werden middels IVF/ICSI hebben een verhoogd
risico op het krijgen van een kind met een afwijking aan de ledematen (aOR: 2.80; CI:
1.51 – 5.20), in het bijzonder polydactylie (aOR: 5.26; CI: 2.47 – 11.20). In
vergelijking met fertiele vrouwen, heeft de totale groep van subfertiele vrouwen (Sub-
NC en IVF/ICSI) een verhoogd risico op het krijgen van een kind met een epispadie
(aOR: 4.28; CI: 1.04 – 17.57) en cysteuze nieren (aOR: 2.10; CI: 1.02 – 4.34).
Verrassend genoeg is er een bijna significante afname van de totale groep van
aangeboren afwijkingen te zien bij de Sub-NC vrouwen in vergelijking met fertiele
vrouwen. Aanvullend is er in de totale groep van subfertiele vrouwen een significant
lager risico op het krijgen van een kind met een congenitale heupdysplasie in

31
vergelijking met de fertiele vrouwen, zoals tevens te zien is bij groep Sub-NC
vrouwen alleen.
Conclusie: Deze studie heeft laten zien dat subfertiele vrouwen, die vervolgens wel
op de natuurlijke manier zwanger werden, een verhoogd risico hebben op het krijgen
van een kind met specifieke aangeboren afwijkingen, in het bijzonder penoscrotale
hypospadie. Gezien het feit dat subfertiliteit een groeiend probleem is, aangezien
vrouwen op steeds latere leeftijd zwanger proberen te raken, zijn onze bevindingen
van belang voor de volksgezondheid.
32
Appendix Maternal and infant characteristics
Cases Controls P-value(n=4392) (n=1456)
Characteristic n (%) n (%)
Pregnancy outcome <0.001
Live birth 3915 (89.1) 933 (64.1)
Live birth but deceased 240 (5.5) 139 (9.5)
Miscarriage 27 (0.6) 41 (2.8)
Termination of pregnancy 156 (3.6) 291 (20.0)
Stillbirth 54 (1.2) 52 (3.6)
0.013
Male 2445 (55.7) 757 (52.0)
Female 1941 (44.2) 699 (48.0)
Unknown 6 (0.1) 0 (0.0)
<0.001
< 25 448 (10.2) 105 (7.2)
25-34 3164 (72.0) 905 (62.2)
> 34 736 (16.8) 432 (29.7)
Missing 44 (1.0) 14 (1.0)
Paternal age at delivery (years) <0.001
< 25 141 (3.2) 34 (2.3)
25-34 2673 (60.9) 742 (51.0)
> 34 1454 (33.1) 638 (43.8)
Missing 124 (2.8) 42 (2.9)
Maternal education 0.015
Low 773 (17,6) 254 (17.4)
Middle 2082 (47.4) 629 (43.2)
High 1329 (30.3) 491 (33.7)
Missing 208 (4.7) 82 (5.6)
Smoking during pregnancy 0.033
Yes 1071 (24.4) 312 (21.4)
No 3232 (73.6) 1100 (75.5)
Missing 89 (2.0) 44 (3.0)
Folic acid use 0.865
Not or in wrong period 1219 (27.8) 400 (27.5)
Periconceptional 2929 (66.7) 950 (65.2)
Missing 244 (5.6) 106 (7.3)
Body mass index (kg/m2
) 0.128
< 18.5 141 (3.2) 39 (2.7)
Infant sex
Maternal age at conception (years)
Distribution of maternal and infant characteristics for cases and controls of
subjects with known fertilitystatus.
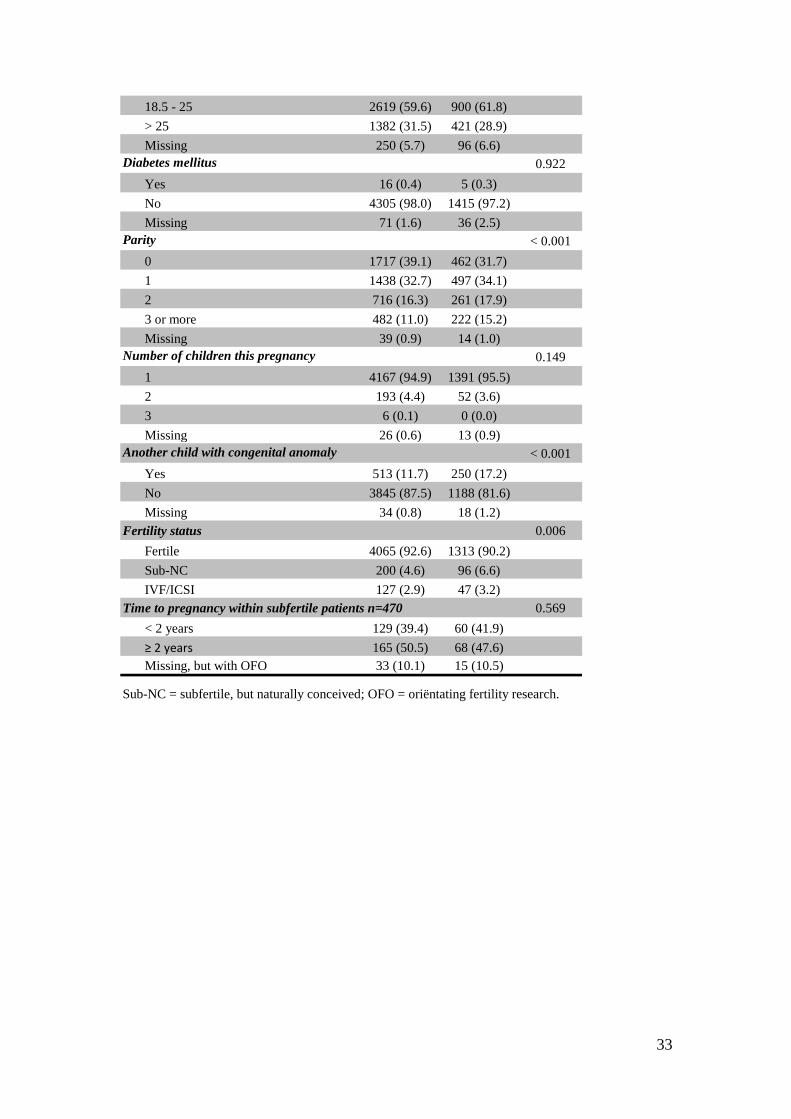
33
18.5 - 25 2619 (59.6) 900 (61.8)
> 25 1382 (31.5) 421 (28.9)
Missing 250 (5.7) 96 (6.6)
Diabetes mellitus 0.922
Yes 16 (0.4) 5 (0.3)
No 4305 (98.0) 1415 (97.2)
Missing 71 (1.6) 36 (2.5)
Parity < 0.001
0 1717 (39.1) 462 (31.7)
1 1438 (32.7) 497 (34.1)
2 716 (16.3) 261 (17.9)
3 or more 482 (11.0) 222 (15.2)
Missing 39 (0.9) 14 (1.0)
Number of children this pregnancy 0.149
1 4167 (94.9) 1391 (95.5)
2 193 (4.4) 52 (3.6)
3 6 (0.1) 0 (0.0)
Missing 26 (0.6) 13 (0.9)
Another child with congenital anomaly < 0.001
Yes 513 (11.7) 250 (17.2)
No 3845 (87.5) 1188 (81.6)
Missing 34 (0.8) 18 (1.2)
Fertility status 0.006
Fertile 4065 (92.6) 1313 (90.2)
Sub-NC 200 (4.6) 96 (6.6)
IVF/ICSI 127 (2.9) 47 (3.2)
0.569
< 2 years 129 (39.4) 60 (41.9)
≥ 2 years 165 (50.5) 68 (47.6)
Missing, but with OFO 33 (10.1) 15 (10.5)
Time to pregnancy within subfertile patients n=470
Sub-NC = subfertile, but naturally conceived; OFO = oriëntating fertility research.
Related Documents











