Indian J Dent Adv 2012; 4(2) 850 Bimaxillary Protrusion - Management With Sliding Mechanics Amit Prakash 1 , Arundhati P. Tandur 2 , Sonali Rai 3 ABSTRACT: The straight wire appliance has supreme control and finishing potential. This case report will evaluate the management of bimaxillary protrusion in adult patient with extraction of premolars. Clinical and cephalometric evaluation revealed Class I Skeletal pattern, Class I dental pattern, bimaxillary protrusion, high mandibular plane angle, increased lower anterior facial height, protruded upper and lower lips, decreased overjet and overbite. The goal of treatment was to use light forces and to provide maximum space for the retraction of anterior teeth. The case was successfully managed by extraction of all first Premolars and fixed appliance therapy using MBT mechanics. Post-treatment changes were good and stable. Key words: Bimaxillary protrusion, MBT mechanics, Malocclusion CASE REPORT doi: ........................... 1 Senior lecturer 2 Professor 3 Private practitioner Department of Orthodontics and Dentofacial Orthopedics Rishi-raj Dental College and Hospital, Bhopal Article Info: Received: April 10, 2012; Review Completed: May, 12, 2012; Accepted: June 7, 2012 Published Online: August, 2012 (www. nacd. in) © NAD, 2012 - All rights reserved Email for correspondence: [email protected] [email protected] Quick Response Code Introduction Class I bimaxillary protrusion is frequent type of malocclusion encountered in India. Its management frequently involves four premolar extractions. These cases were earlier managed to reasonable extent using edgewise appliance 1,2 and later with Begg’s appliance. 3 This case report illustrates An adult male patient having angles Class I dental with bimaxillary protrusion on class I skeletal base treated with extraction of all the first premolars using 022 MBT (McLaughlin Bennett Trevisi) mechanics 4 Case -Report This 16-year-old patient presented with a Class I bimaxillary protrusion malocclusion with a significant anteroposterior skeletal discrepancy, and a high angle between the maxillary and mandibular planes. The patient requested treatment to improve his dental appearance. He had no relevant medical history. Extra oral examination revealed convex profile, high mandibular plane angle, increased lower anterior facial height, protruded lips. Intraoral examination revealed Angles Class I molar and canine relation, generalized anterior spacing in upper arch. Lower midline shifted to left side by 1 mm, good oral hygiene, healthy soft tissue, U- shaped maxillary and mandibular arches, decreased overjet and overbite, unerupted 3 rd molars (Fig. 1). To achieve an ideal result, a treatment plan using MBT appliance was planned and a treatment based on orthodontic compensation and extraction of all upper and lower first premolars was implemented. INDIAN JOURNAL OF DENTAL ADVANCEMENTS Journal homepage: www. nacd. in

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Indian J Dent Adv 2012; 4(2) 850
Bimaxillary Protrusion - ManagementWith Sliding Mechanics
Amit Prakash1, Arundhati P. Tandur2, Sonali Rai3
ABSTRACT:
The straight wire appliance has supreme control and finishing
potential. This case report will evaluate the management of
bimaxillary protrusion in adult patient with extraction of
premolars. Clinical and cephalometric evaluation revealed Class
I Skeletal pattern, Class I dental pattern, bimaxillary
protrusion, high mandibular plane angle, increased lower
anterior facial height, protruded upper and lower lips, decreased
overjet and overbite. The goal of treatment was to use light forces
and to provide maximum space for the retraction of anterior
teeth. The case was successfully managed by extraction of all
first Premolars and fixed appliance therapy using MBT
mechanics. Post-treatment changes were good and stable.
Key words: Bimaxillary protrusion, MBT mechanics,
Malocclusion
C A S E R E P O R T
doi: ...........................
1Senior lecturer2Professor3Private practitioner
Department of Orthodontics and DentofacialOrthopedicsRishi-raj Dental College and Hospital, Bhopal
Article Info:
Received: April 10, 2012;Review Completed: May, 12, 2012;Accepted: June 7, 2012Published Online: August, 2012 (www. nacd. in)© NAD, 2012 - All rights reserved
Email for correspondence:[email protected]@gmail.com
Quick Response Code
IntroductionClass I bimaxillary protrusion is frequent type of malocclusion encountered in India. Its managementfrequently involves four premolar extractions. These cases were earlier managed to reasonable extent usingedgewise appliance1,2 and later with Begg’s appliance.3 This case report illustrates An adult male patienthaving angles Class I dental with bimaxillary protrusion on class I skeletal base treated with extraction ofall the first premolars using 022 MBT (McLaughlin Bennett Trevisi) mechanics4
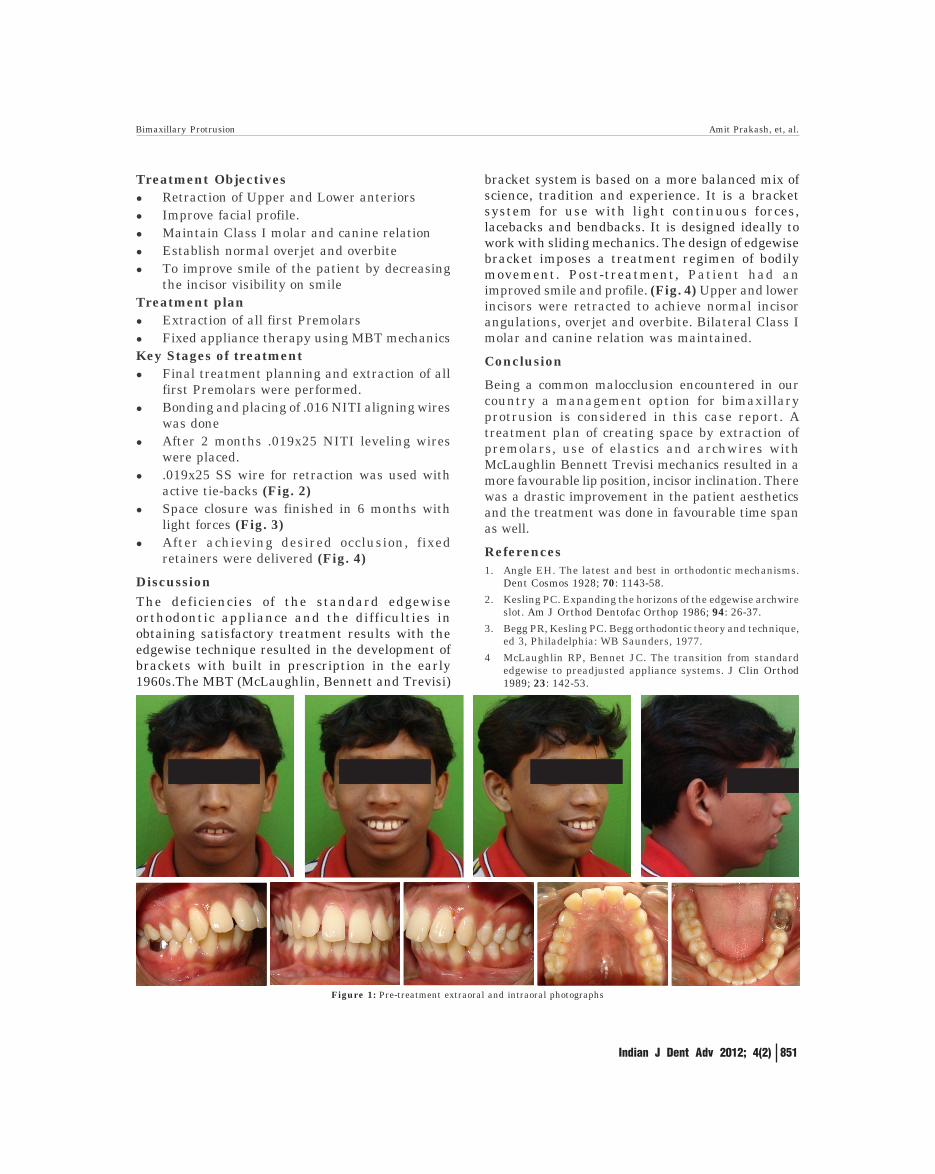
Case -ReportThis 16-year-old patient presented with a Class I bimaxillary protrusion malocclusion with a significantanteroposterior skeletal discrepancy, and a high angle between the maxillary and mandibular planes. Thepatient requested treatment to improve his dental appearance. He had no relevant medical history. Extraoral examination revealed convex profile, high mandibular plane angle, increased lower anterior facial height,protruded lips. Intraoral examination revealed Angles Class I molar and canine relation, generalized anteriorspacing in upper arch. Lower midline shifted to left side by 1 mm, good oral hygiene, healthy soft tissue, U-shaped maxillary and mandibular arches, decreased overjet and overbite, unerupted 3rd molars (Fig. 1). Toachieve an ideal result, a treatment plan using MBT appliance was planned and a treatment based onorthodontic compensation and extraction of all upper and lower first premolars was implemented.
INDIAN JOURNAL OF DENTAL ADVANCEMENTS
Jour nal homepage: www. nacd. in
Indian J Dent Adv 2012; 4(2) 851
Treatment Objectives� Retraction of Upper and Lower anteriors� Improve facial profile.� Maintain Class I molar and canine relation� Establish normal overjet and overbite� To improve smile of the patient by decreasing
the incisor visibility on smileTreatment plan� Extraction of all first Premolars� Fixed appliance therapy using MBT mechanicsKey Stages of treatment� Final treatment planning and extraction of all
first Premolars were performed.� Bonding and placing of .016 NITI aligning wires
was done� After 2 months .019x25 NITI leveling wires
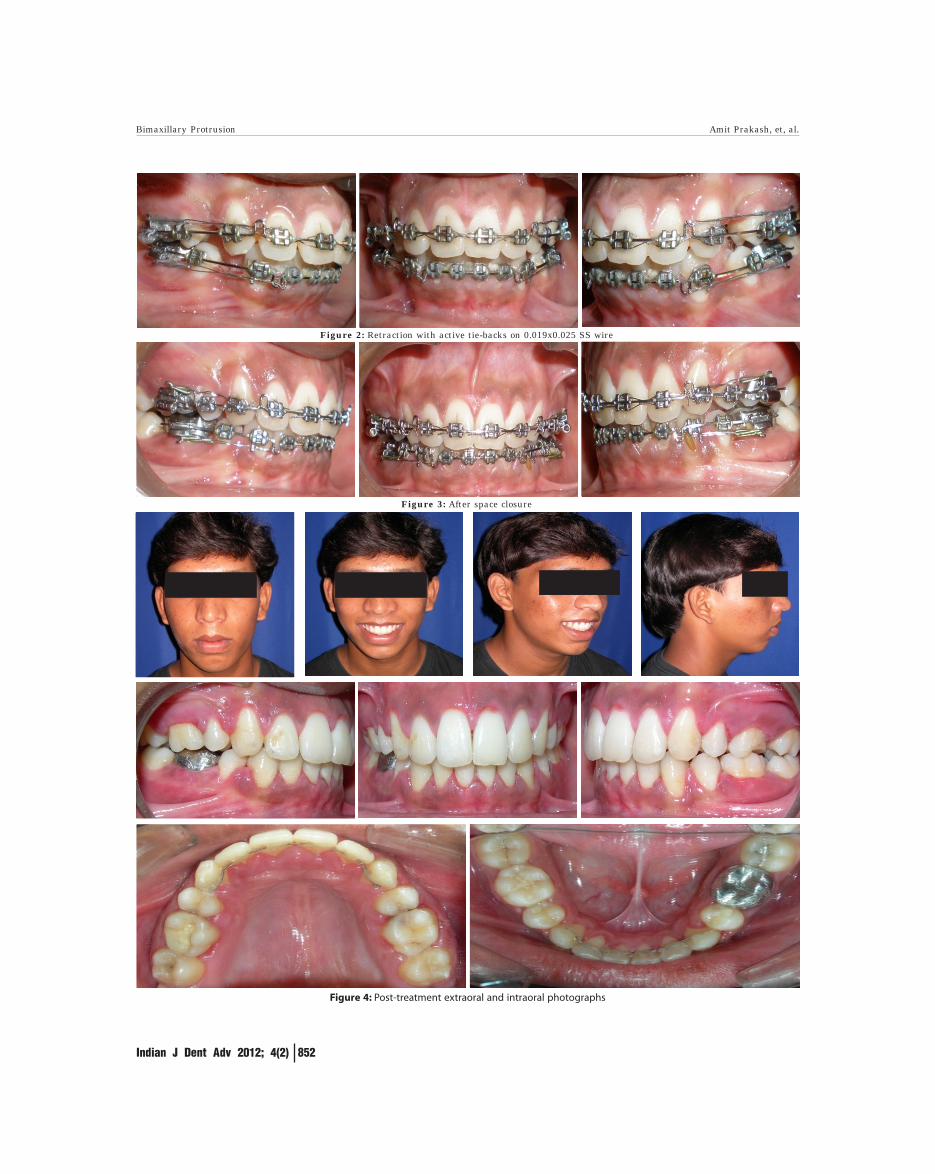
were placed.� .019x25 SS wire for retraction was used with
active tie-backs (Fig. 2)� Space closure was finished in 6 months with
light forces (Fig. 3)� After achieving desired occlusion, fixed
retainers were delivered (Fig. 4)
DiscussionThe deficiencies of the standard edgewiseorthodontic appliance and the difficulties inobtaining satisfactory treatment results with theedgewise technique resulted in the development ofbrackets with built in prescription in the early1960s.The MBT (McLaughlin, Bennett and Trevisi)
bracket system is based on a more balanced mix ofscience, tradition and experience. It is a bracketsystem for use with light continuous forces,lacebacks and bendbacks. It is designed ideally towork with sliding mechanics. The design of edgewisebracket imposes a treatment regimen of bodilymovement. Post-treatment, Patient had animproved smile and profile. (Fig. 4) Upper and lowerincisors were retracted to achieve normal incisorangulations, overjet and overbite. Bilateral Class Imolar and canine relation was maintained.
Conclusion
Being a common malocclusion encountered in ourcountry a management option for bimaxillaryprotrusion is considered in this case report. Atreatment plan of creating space by extraction ofpremolars, use of elastics and archwires withMcLaughlin Bennett Trevisi mechanics resulted in amore favourable lip position, incisor inclination. Therewas a drastic improvement in the patient aestheticsand the treatment was done in favourable time spanas well.
References1. Angle EH. The latest and best in orthodontic mechanisms.
Dent Cosmos 1928; 70: 1143-58.
2. Kesling PC. Expanding the horizons of the edgewise archwireslot. Am J Orthod Dentofac Orthop 1986; 94: 26-37.
3. Begg PR, Kesling PC. Begg orthodontic theory and technique,ed 3, Philadelphia: WB Saunders, 1977.
4 McLaughlin RP, Bennet JC. The transition from standardedgewise to preadjusted appliance systems. J Clin Orthod1989; 23: 142-53.
Figure 1: Pre-treatment extraoral and intraoral photographs
Bimaxillary Protrusion Amit Prakash, et, al.
Indian J Dent Adv 2012; 4(2) 852
Figure 2: Retraction with active tie-backs on 0.019x0.025 SS wire
Figure 3: After space closure
Figure 4: Post-treatment extraoral and intraoral photographs
Bimaxillary Protrusion Amit Prakash, et, al.
Related Documents











