Atorvastatin Prior to Percutaneous Coronary Intervention Following Myocardial Infarction Nina Hull, PharmD. PGY1 Pharmacy Resident Methodist Hospital, San Antonio, TX Division of Pharmacotherapy, The University of Texas at Austin College of Pharmacy Pharmacotherapy Education and Research Center University of Texas Health Science Center at San Antonio March 21, 2014 Learning Objectives . 1.) Discuss epidemiology and pathophysiology of acute coronary syndromes 2.) Identify the different treatment options for acute coronary syndromes 3.) Review the uses of atorvastatin and its role in patients with myocardial infarction 4.) Discuss primary literature describing atorvastatin use in patients undergoing percutaneous coronary intervention 5.) Summarize findings to make treatment recommendations for myocardial infarction patients

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Atorvastatin Prior to Percutaneous Coronary Intervention Following
Myocardial Infarction
Nina Hull, PharmD. PGY1 Pharmacy Resident
Methodist Hospital, San Antonio, TX Division of Pharmacotherapy, The University of Texas at Austin College of Pharmacy
Pharmacotherapy Education and Research Center University of Texas Health Science Center at San Antonio
March 21, 2014
Learning Objectives .
1.) Discuss epidemiology and pathophysiology of acute coronary syndromes
2.) Identify the different treatment options for acute coronary syndromes
3.) Review the uses of atorvastatin and its role in patients with myocardial infarction
4.) Discuss primary literature describing atorvastatin use in patients undergoing percutaneous
coronary intervention
5.) Summarize findings to make treatment recommendations for myocardial infarction patients
N. Hull 2
ACUTE CORONARY SYNDROMES
I. Acute Coronary Syndrome Background1-10
A. Acute coronary syndromes (ACS) occur from an imbalance between myocardial oxygen
demand and supply, resulting in acute myocardial ischemia B. Epidemiology
i. The American Heart Association reports 1.4 million annual hospitalizations for ACS in the United States
ii. Approximately 15% of people who experience a myocardial infarction (MI) will die from it
iii. However, an analysis from Centers for Medicare and Medicaid Services showed that between 1995 and 2006, the 30-day mortality rate attributed to MI decreased
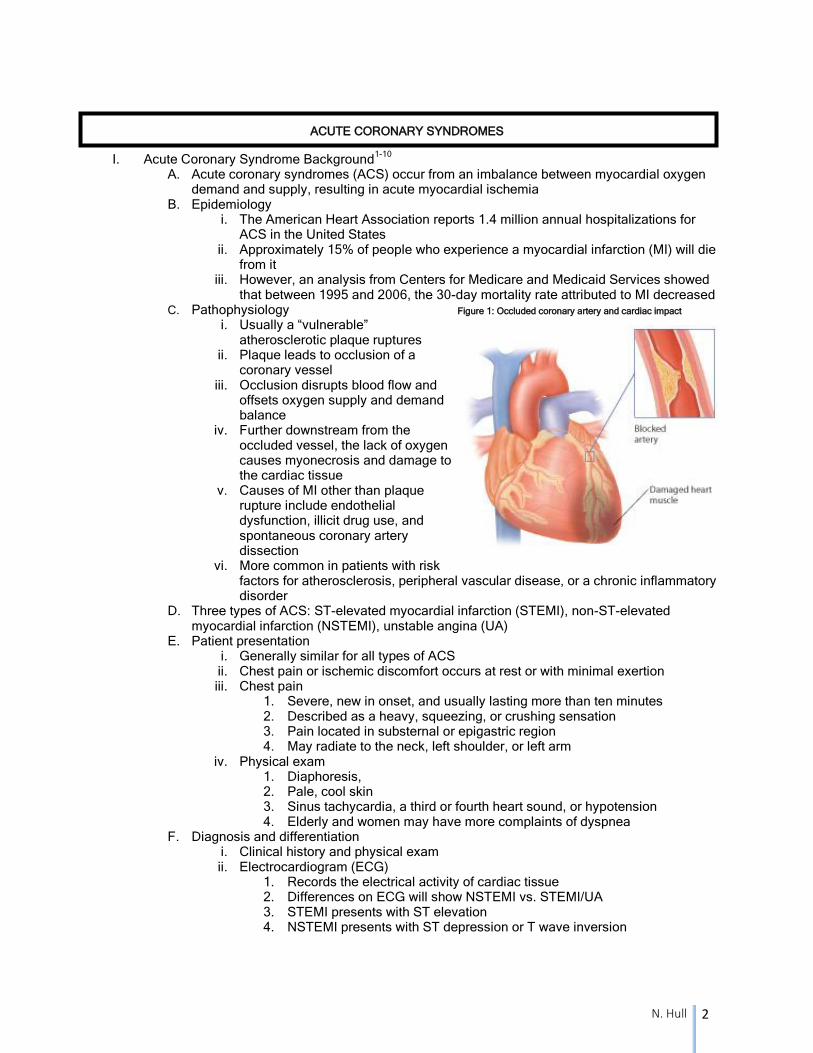
C. Pathophysiology Figure 1: Occluded coronary artery and cardiac impact i. Usually a “vulnerable”
atherosclerotic plaque ruptures ii. Plaque leads to occlusion of a
coronary vessel iii. Occlusion disrupts blood flow and
offsets oxygen supply and demand balance
iv. Further downstream from the occluded vessel, the lack of oxygen causes myonecrosis and damage to the cardiac tissue
v. Causes of MI other than plaque rupture include endothelial dysfunction, illicit drug use, and spontaneous coronary artery dissection
vi. More common in patients with risk factors for atherosclerosis, peripheral vascular disease, or a chronic inflammatory disorder
D. Three types of ACS: ST-elevated myocardial infarction (STEMI), non-ST-elevated myocardial infarction (NSTEMI), unstable angina (UA)
E. Patient presentation i. Generally similar for all types of ACS ii. Chest pain or ischemic discomfort occurs at rest or with minimal exertion iii. Chest pain
1. Severe, new in onset, and usually lasting more than ten minutes 2. Described as a heavy, squeezing, or crushing sensation 3. Pain located in substernal or epigastric region 4. May radiate to the neck, left shoulder, or left arm
iv. Physical exam 1. Diaphoresis, 2. Pale, cool skin 3. Sinus tachycardia, a third or fourth heart sound, or hypotension 4. Elderly and women may have more complaints of dyspnea
F. Diagnosis and differentiation i. Clinical history and physical exam ii. Electrocardiogram (ECG)
1. Records the electrical activity of cardiac tissue 2. Differences on ECG will show NSTEMI vs. STEMI/UA 3. STEMI presents with ST elevation 4. NSTEMI presents with ST depression or T wave inversion
N. Hull 3
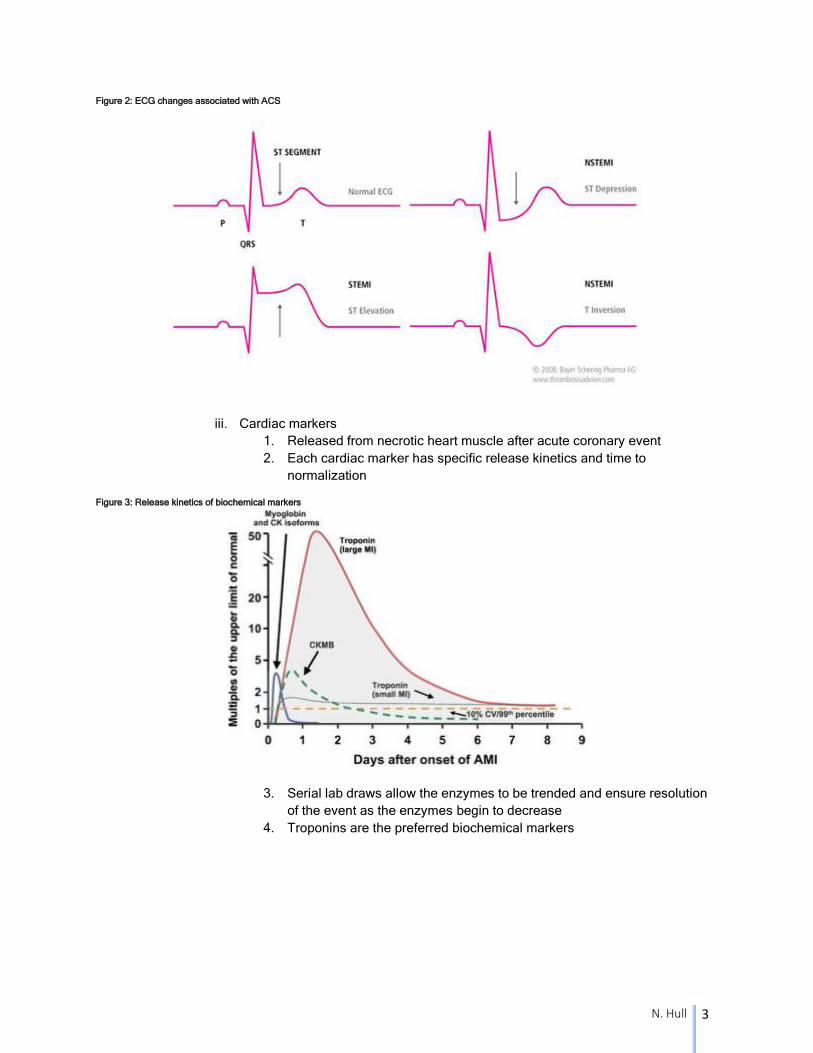
Figure 2: ECG changes associated with ACS
iii. Cardiac markers
1. Released from necrotic heart muscle after acute coronary event
2. Each cardiac marker has specific release kinetics and time to
normalization
Figure 3: Release kinetics of biochemical markers
3. Serial lab draws allow the enzymes to be trended and ensure resolution
of the event as the enzymes begin to decrease
4. Troponins are the preferred biochemical markers
N. Hull 4
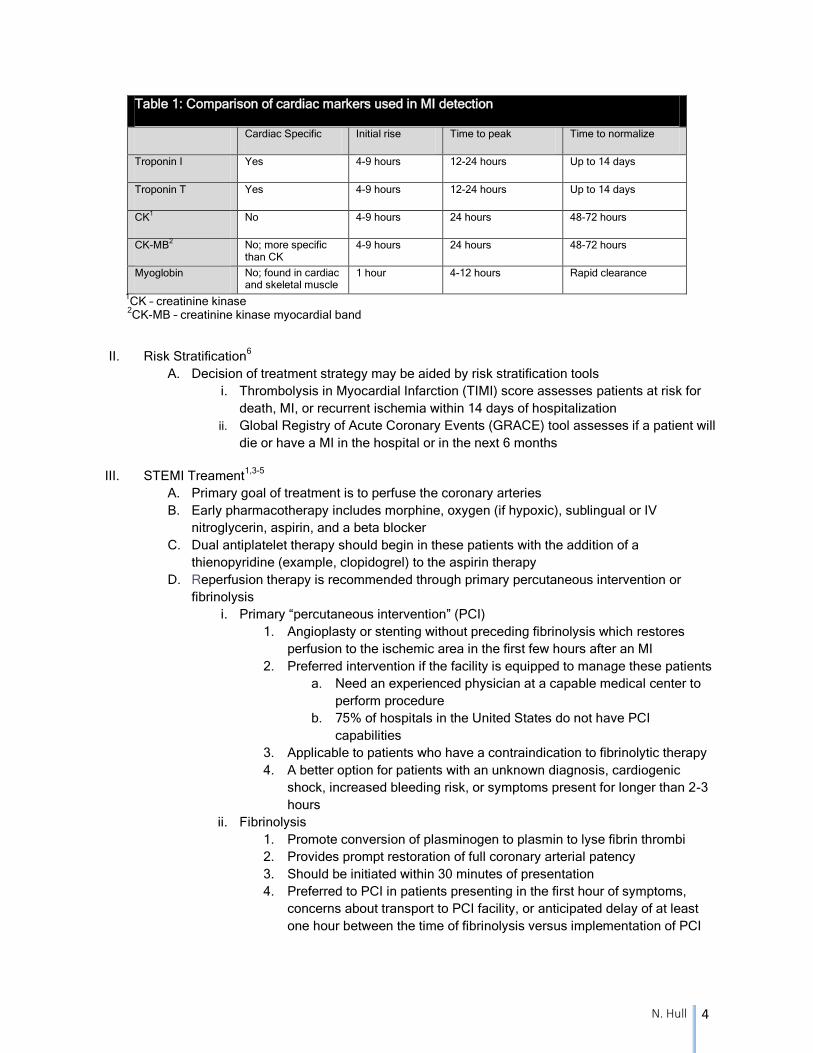
Table 1: Comparison of cardiac markers used in MI detection
Cardiac Specific Initial rise Time to peak Time to normalize
Troponin I Yes 4-9 hours 12-24 hours Up to 14 days
Troponin T Yes 4-9 hours 12-24 hours Up to 14 days
CK1
No 4-9 hours 24 hours 48-72 hours
CK-MB2
No; more specific than CK
4-9 hours 24 hours 48-72 hours
Myoglobin No; found in cardiac and skeletal muscle
1 hour 4-12 hours Rapid clearance
1CK – creatinine kinase
2CK-MB – creatinine kinase myocardial band
II. Risk Stratification6
A. Decision of treatment strategy may be aided by risk stratification tools
i. Thrombolysis in Myocardial Infarction (TIMI) score assesses patients at risk for
death, MI, or recurrent ischemia within 14 days of hospitalization
ii. Global Registry of Acute Coronary Events (GRACE) tool assesses if a patient will
die or have a MI in the hospital or in the next 6 months
III. STEMI Treament1,3-5
A. Primary goal of treatment is to perfuse the coronary arteries
B. Early pharmacotherapy includes morphine, oxygen (if hypoxic), sublingual or IV
nitroglycerin, aspirin, and a beta blocker
C. Dual antiplatelet therapy should begin in these patients with the addition of a
thienopyridine (example, clopidogrel) to the aspirin therapy
D. Reperfusion therapy is recommended through primary percutaneous intervention or
fibrinolysis
i. Primary “percutaneous intervention” (PCI)
1. Angioplasty or stenting without preceding fibrinolysis which restores
perfusion to the ischemic area in the first few hours after an MI
2. Preferred intervention if the facility is equipped to manage these patients
a. Need an experienced physician at a capable medical center to
perform procedure
b. 75% of hospitals in the United States do not have PCI
capabilities
3. Applicable to patients who have a contraindication to fibrinolytic therapy
4. A better option for patients with an unknown diagnosis, cardiogenic
shock, increased bleeding risk, or symptoms present for longer than 2-3
hours
ii. Fibrinolysis
1. Promote conversion of plasminogen to plasmin to lyse fibrin thrombi
2. Provides prompt restoration of full coronary arterial patency
3. Should be initiated within 30 minutes of presentation
4. Preferred to PCI in patients presenting in the first hour of symptoms,
concerns about transport to PCI facility, or anticipated delay of at least
one hour between the time of fibrinolysis versus implementation of PCI
N. Hull 5
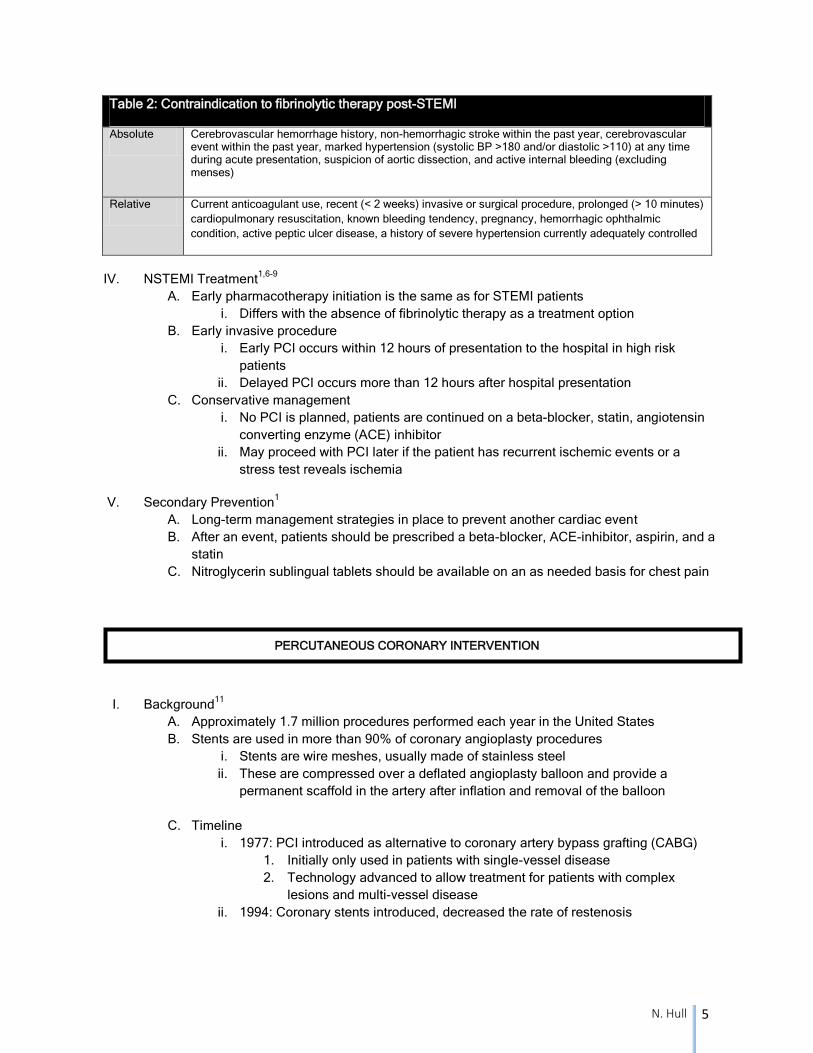
Table 2: Contraindication to fibrinolytic therapy post-STEMI
Absolute Cerebrovascular hemorrhage history, non-hemorrhagic stroke within the past year, cerebrovascular event within the past year, marked hypertension (systolic BP >180 and/or diastolic >110) at any time during acute presentation, suspicion of aortic dissection, and active internal bleeding (excluding menses)
Relative Current anticoagulant use, recent (< 2 weeks) invasive or surgical procedure, prolonged (> 10 minutes)
cardiopulmonary resuscitation, known bleeding tendency, pregnancy, hemorrhagic ophthalmic
condition, active peptic ulcer disease, a history of severe hypertension currently adequately controlled
IV. NSTEMI Treatment1,6-9
A. Early pharmacotherapy initiation is the same as for STEMI patients
i. Differs with the absence of fibrinolytic therapy as a treatment option
B. Early invasive procedure
i. Early PCI occurs within 12 hours of presentation to the hospital in high risk
patients
ii. Delayed PCI occurs more than 12 hours after hospital presentation
C. Conservative management
i. No PCI is planned, patients are continued on a beta-blocker, statin, angiotensin
converting enzyme (ACE) inhibitor
ii. May proceed with PCI later if the patient has recurrent ischemic events or a
stress test reveals ischemia
V. Secondary Prevention1
A. Long-term management strategies in place to prevent another cardiac event
B. After an event, patients should be prescribed a beta-blocker, ACE-inhibitor, aspirin, and a
statin
C. Nitroglycerin sublingual tablets should be available on an as needed basis for chest pain
PERCUTANEOUS CORONARY INTERVENTION
I. Background11
A. Approximately 1.7 million procedures performed each year in the United States
B. Stents are used in more than 90% of coronary angioplasty procedures
i. Stents are wire meshes, usually made of stainless steel
ii. These are compressed over a deflated angioplasty balloon and provide a
permanent scaffold in the artery after inflation and removal of the balloon
C. Timeline
i. 1977: PCI introduced as alternative to coronary artery bypass grafting (CABG)
1. Initially only used in patients with single-vessel disease
2. Technology advanced to allow treatment for patients with complex
lesions and multi-vessel disease
ii. 1994: Coronary stents introduced, decreased the rate of restenosis
N. Hull 6
iii. 2003: Drug-eluting stents introduced, further decreased restenosis
1. Polymer coating over the metal stent releases anti-proliferative drugs
directly into the plaque over one to three months after implantation
2. First generation devices were coated with sirolimus or paclitaxel
3. Second-generation stents used everolimus, biolimus, and zotarolimus
II. Procedure11,12
A. Medications
i. Patients are loaded with aspirin 325 mg and clopidogrel 300-600 mg before the
procedure
ii. During the procedure, anticoagulation is administered with heparin, low molecular
weight heparin, or bivalirudin
iii. A glycoprotein IIb/IIIa inhibitor may also be given for STEMI, high-risk acute
coronary syndrome, or those with a large thrombus in the coronary artery
B. Arterial access obtained, most commonly through the femoral artery or radial artery; a
sheath and preformed guidewire are inserted
i. The guidewire serves as a “rail” over which angioplasty balloon and stent are
advanced to enlarge the narrowed segment of a coronary artery
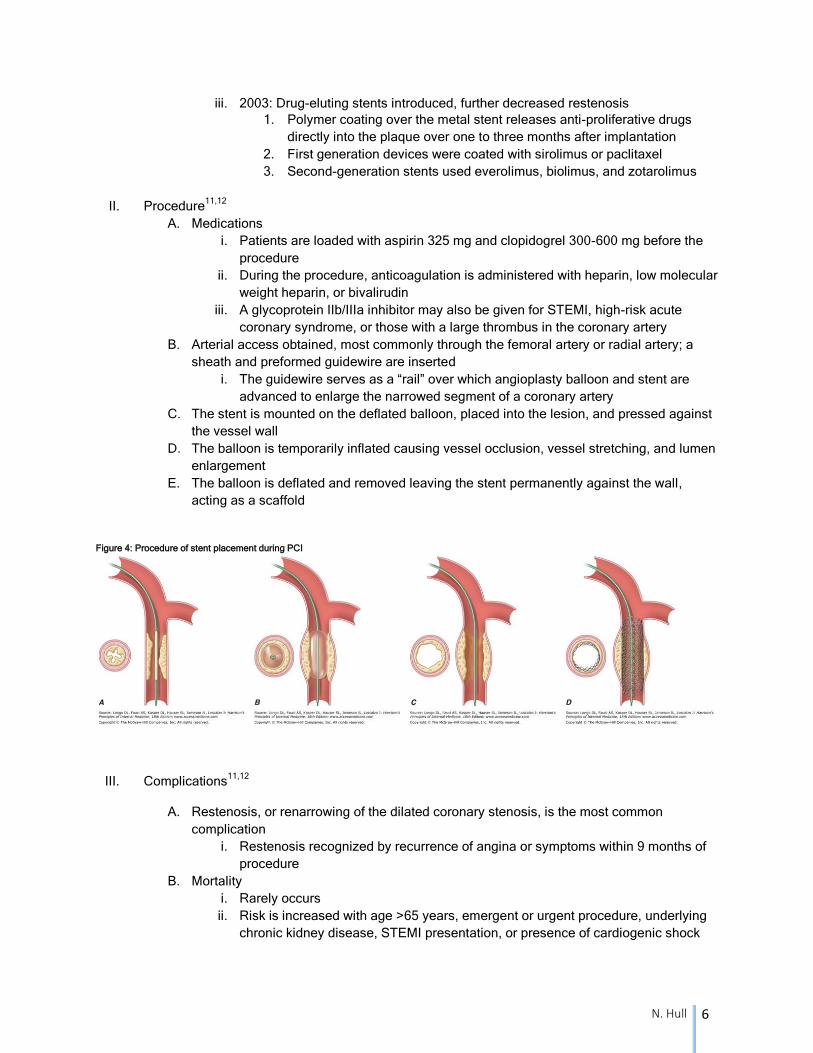
C. The stent is mounted on the deflated balloon, placed into the lesion, and pressed against
the vessel wall
D. The balloon is temporarily inflated causing vessel occlusion, vessel stretching, and lumen
enlargement
E. The balloon is deflated and removed leaving the stent permanently against the wall,
acting as a scaffold
Figure 4: Procedure of stent placement during PCI
III. Complications11,12
A. Restenosis, or renarrowing of the dilated coronary stenosis, is the most common
complication
i. Restenosis recognized by recurrence of angina or symptoms within 9 months of
procedure
B. Mortality
i. Rarely occurs
ii. Risk is increased with age >65 years, emergent or urgent procedure, underlying
chronic kidney disease, STEMI presentation, or presence of cardiogenic shock
N. Hull 7
C. Myocardial infarction
i. MI during PCI, or periprocedural MI (pMI), can occur for multiple reasons,
including acute occluding thrombus, severe coronary dissection , embolization of
thrombus or atherosclerotic material, or closure of a side branch vessel at the site
of angioplasty
ii. Noted in 5-40% of patients undergoing PCI, depending on the criteria used
iii. Most MIs are small and only detected by rise in CPK or troponin after procedure
1. Historically, only those with enzyme elevations three times the upper limit
of normal were associated with less favorable long-term outcomes and
determined to be significant
2. Cardiac biomarker testing has become more sensitive, so many enzyme
elevations may not be significant
3. However, cardiac imaging has shown that even small biomarker
elevations result in myonecrosis
4. Large pMI has shown to increase mortality; the risk is debated in relation
to small or medium pMI
5. The newest definition from ESC/ACC/AHA/WHF task force says a pMI
requires a troponin elevation of more than five times the 99th
percentile of
normal with supporting clinical, angiographic, or imaging evidence of
ischemia post-procedure
iv. Reducing incidence of pMI is an area of research to provide better outcomes for
these patients
v. Biomarker elevation is a target of interest with attempts to improve mortality with
dual antiplatelet therapy and antiplatelet loads, glycoprotein IIb/IIIa inhibitor
additions
vi. More than one-third of patients who experience a STEMI and are scheduled for
PCI have impaired myocardial tissue perfusion and an unfavorable outcome
1. Periprocedural care needs to be optimized to prevent further
complications in post MI patients
2. One area of research includes the use of HMG-CoA reductase inhibitors
prior to PCI
ATORVASTATIN
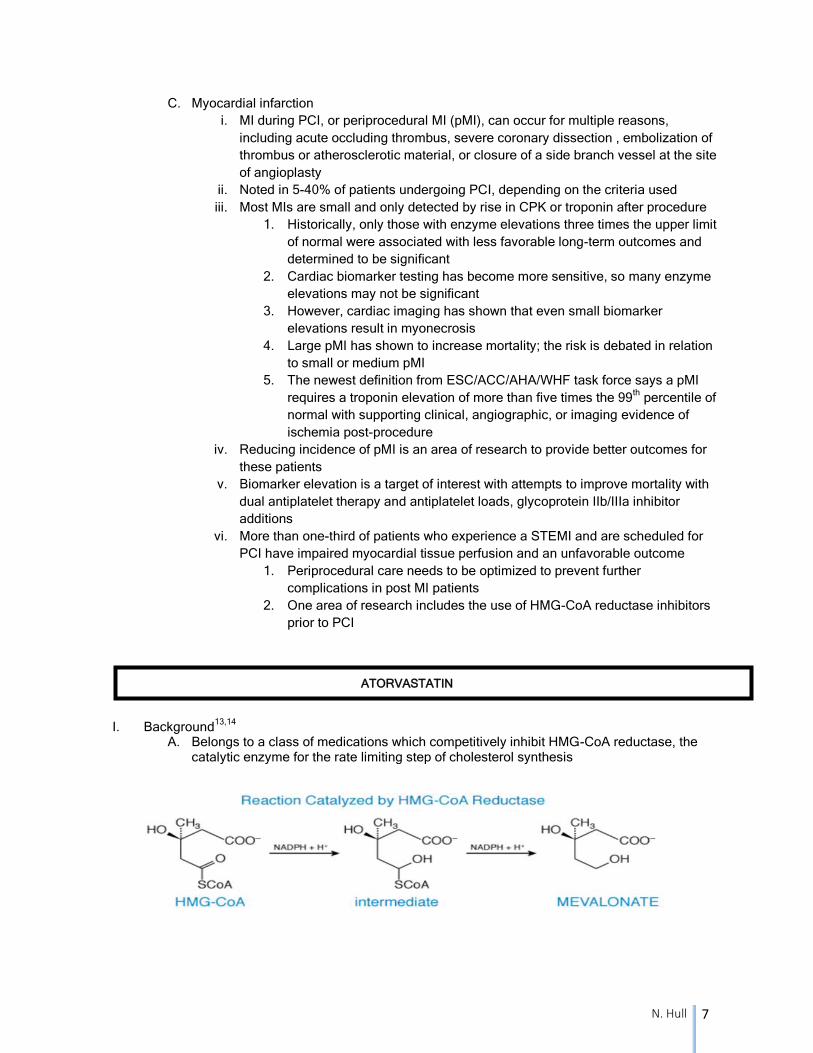
I. Background13,14
A. Belongs to a class of medications which competitively inhibit HMG-CoA reductase, the
catalytic enzyme for the rate limiting step of cholesterol synthesis
N. Hull 8
B. Class of medications also known as statins, based on the prototype mevastatin,
discovered in 1971
C. Currently, seven different statin agents available on the United States market
D. Main target is low density lipoprotein cholesterol in patients with dyslipidemia
II. Uses14
A. Adjunct to diet to reduce elevated total cholesterol, LDL cholesterol and increase HDL
cholesterol in adults with primary hyperlipidemia or mixed dyslipidemia
B. Adjunct to diet to reduce the risk of myocardial infarction, stroke, revascularization
procedures, and angina in patients with coronary heart disease, or without coronary heart
disease with risk factors
C. Primary and secondary prevention of cardiovascular disease
III. Dosing14
A. Ranges from 10 mg to 80 mg daily, with a typical starting dose of 10 to 20 mg
B. May be given at any time of the day without regard to food
IV. Adverse events14
A. Contraindicated in patients with active liver disease, pregnancy, and lactating mothers
B. Skeletal muscle effects, such as myopathy or rhabdomyolysis may occur
i. Risk is increased with coadministration of drugs that increase the levels of
atorvastatin
ii. May also occur in patients with baseline renal impairment, hypothyroidism, or age
over 65
C. Elevated hepatic transaminases
i. Check liver function tests at baseline and as necessary
ii. Tests results usually return to baseline after discontinuation of the statin agent
D. Drug interactions with CYP34A inhibitors or inducers
VI. Additional effects of statins16
A. Evidence suggests multiple other effects of statin beyond lipid lowering which include
i. Improvement of endothelial dysfunction
ii. Increased nitric oxide bioavailability
iii. Antioxidant properties
iv. Inhibition of inflammatory responses
v. Stabilization of atherosclerotic plaques
B. The mechanism may occur from the same interruption to the mevalonate pathway, which
causes a downstream inhibition of isoprenoid intermediates
i. The intermediates serve as post-translational modifiers of intracellular proteins
involved in inflammatory processes
LITERATURE REVIEW
I. Background A. Statins have shown benefit for coronary artery disease with long-term therapy and have
indications for risk reduction in patients with high cholesterol B. Observational studies in patients with acute MI suggested statin initiation within 24 hours
was associated with a significantly lower occurrence of early complications, a reduced infarct size, and better in-hospital survival
N. Hull 9
C. Observational animal and human studies noted a possible place for statin initiation prior to PCI in patients
D. Initial “Atorvastatin for Reduction of Myocardial Damage during Angioplasty” (ARMYDA) trial in 2004 was a randomized study showing the clinical benefit of pretreatment with statins in patients undergoing PCI
i. Included statin naïve, stable angina patients undergoing non-emergent PCI ii. High dose atorvastatin initiated one week prior to the procedure iii. Atorvastatin significantly reduced the risk of pMI in patients with stable angina
E. Newer studies have been published to investigate the use of statin loading doses in patients undergoing PCI after an acute coronary event
II. Clinical considerations
A. Is a statin load appropriate for patients undergoing PCI after an acute coronary event? B. When should therapy be initiated? C. What dose or doses should be used?
N. Hull 10
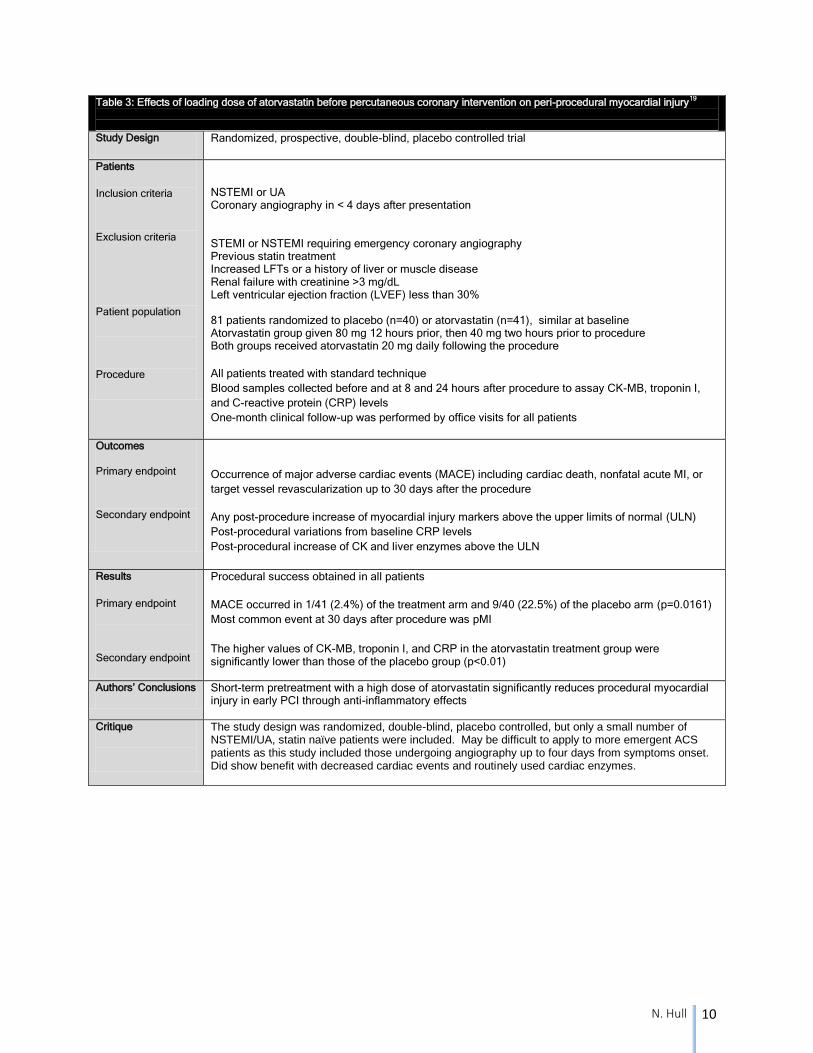
Table 3: Effects of loading dose of atorvastatin before percutaneous coronary intervention on peri-procedural myocardial injury19
Study Design Randomized, prospective, double-blind, placebo controlled trial
Patients
Inclusion criteria
Exclusion criteria
Patient population
Procedure
NSTEMI or UA Coronary angiography in < 4 days after presentation STEMI or NSTEMI requiring emergency coronary angiography Previous statin treatment Increased LFTs or a history of liver or muscle disease Renal failure with creatinine >3 mg/dL Left ventricular ejection fraction (LVEF) less than 30%
81 patients randomized to placebo (n=40) or atorvastatin (n=41), similar at baseline Atorvastatin group given 80 mg 12 hours prior, then 40 mg two hours prior to procedure Both groups received atorvastatin 20 mg daily following the procedure
All patients treated with standard technique
Blood samples collected before and at 8 and 24 hours after procedure to assay CK-MB, troponin I,
and C-reactive protein (CRP) levels
One-month clinical follow-up was performed by office visits for all patients
Outcomes
Primary endpoint
Secondary endpoint
Occurrence of major adverse cardiac events (MACE) including cardiac death, nonfatal acute MI, or
target vessel revascularization up to 30 days after the procedure
Any post-procedure increase of myocardial injury markers above the upper limits of normal (ULN)
Post-procedural variations from baseline CRP levels
Post-procedural increase of CK and liver enzymes above the ULN
Results
Primary endpoint
Secondary endpoint
Procedural success obtained in all patients
MACE occurred in 1/41 (2.4%) of the treatment arm and 9/40 (22.5%) of the placebo arm (p=0.0161)
Most common event at 30 days after procedure was pMI
The higher values of CK-MB, troponin I, and CRP in the atorvastatin treatment group were significantly lower than those of the placebo group (p<0.01)
Authors’ Conclusions Short-term pretreatment with a high dose of atorvastatin significantly reduces procedural myocardial injury in early PCI through anti-inflammatory effects
Critique
The study design was randomized, double-blind, placebo controlled, but only a small number of NSTEMI/UA, statin naïve patients were included. May be difficult to apply to more emergent ACS patients as this study included those undergoing angiography up to four days from symptoms onset. Did show benefit with decreased cardiac events and routinely used cardiac enzymes.
N. Hull 11
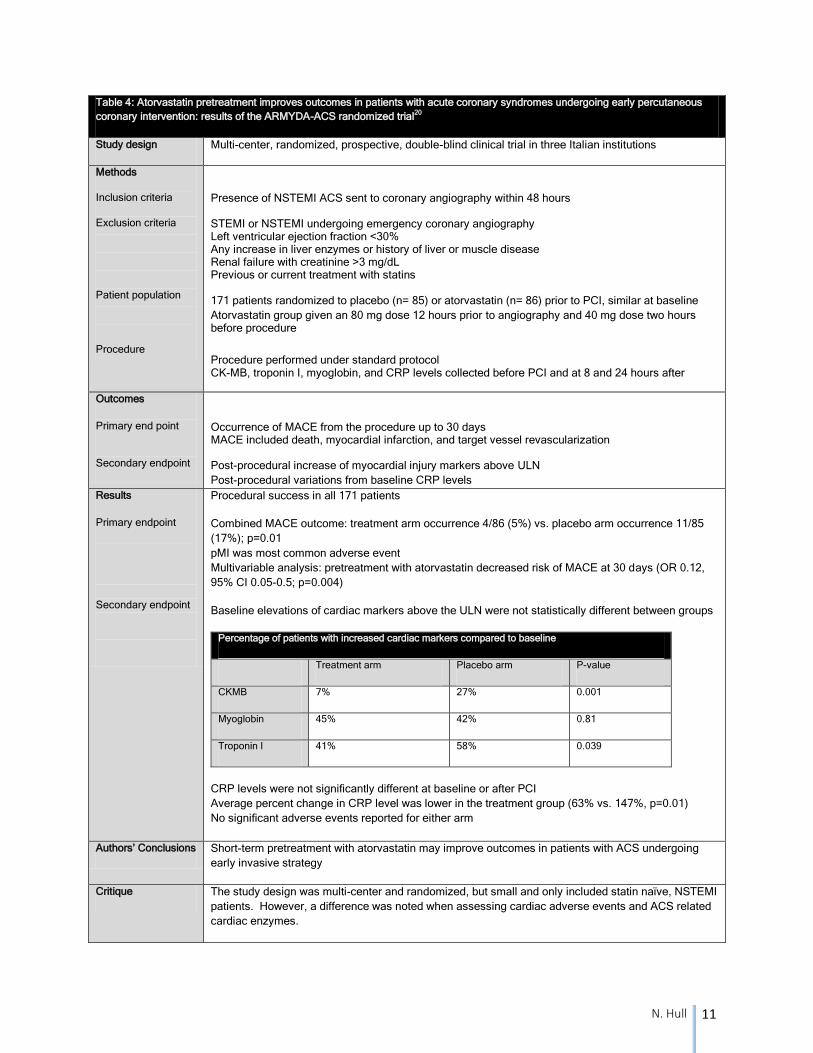
Table 4: Atorvastatin pretreatment improves outcomes in patients with acute coronary syndromes undergoing early percutaneous
coronary intervention: results of the ARMYDA-ACS randomized trial20
Study design Multi-center, randomized, prospective, double-blind clinical trial in three Italian institutions
Methods
Inclusion criteria
Exclusion criteria
Patient population
Procedure
Presence of NSTEMI ACS sent to coronary angiography within 48 hours STEMI or NSTEMI undergoing emergency coronary angiography Left ventricular ejection fraction <30% Any increase in liver enzymes or history of liver or muscle disease Renal failure with creatinine >3 mg/dL Previous or current treatment with statins 171 patients randomized to placebo (n= 85) or atorvastatin (n= 86) prior to PCI, similar at baseline
Atorvastatin group given an 80 mg dose 12 hours prior to angiography and 40 mg dose two hours before procedure
Procedure performed under standard protocol CK-MB, troponin I, myoglobin, and CRP levels collected before PCI and at 8 and 24 hours after
Outcomes
Primary end point
Secondary endpoint
Occurrence of MACE from the procedure up to 30 days MACE included death, myocardial infarction, and target vessel revascularization Post-procedural increase of myocardial injury markers above ULN
Post-procedural variations from baseline CRP levels
Results
Primary endpoint
Secondary endpoint
Procedural success in all 171 patients
Combined MACE outcome: treatment arm occurrence 4/86 (5%) vs. placebo arm occurrence 11/85
(17%); p=0.01
pMI was most common adverse event
Multivariable analysis: pretreatment with atorvastatin decreased risk of MACE at 30 days (OR 0.12,
95% CI 0.05-0.5; p=0.004)
Baseline elevations of cardiac markers above the ULN were not statistically different between groups
Percentage of patients with increased cardiac markers compared to baseline
Treatment arm Placebo arm P-value
CKMB 7% 27% 0.001
Myoglobin 45% 42% 0.81
Troponin I 41% 58% 0.039
CRP levels were not significantly different at baseline or after PCI
Average percent change in CRP level was lower in the treatment group (63% vs. 147%, p=0.01)
No significant adverse events reported for either arm
Authors’ Conclusions Short-term pretreatment with atorvastatin may improve outcomes in patients with ACS undergoing
early invasive strategy
Critique The study design was multi-center and randomized, but small and only included statin naïve, NSTEMI
patients. However, a difference was noted when assessing cardiac adverse events and ACS related
cardiac enzymes.
N. Hull 12
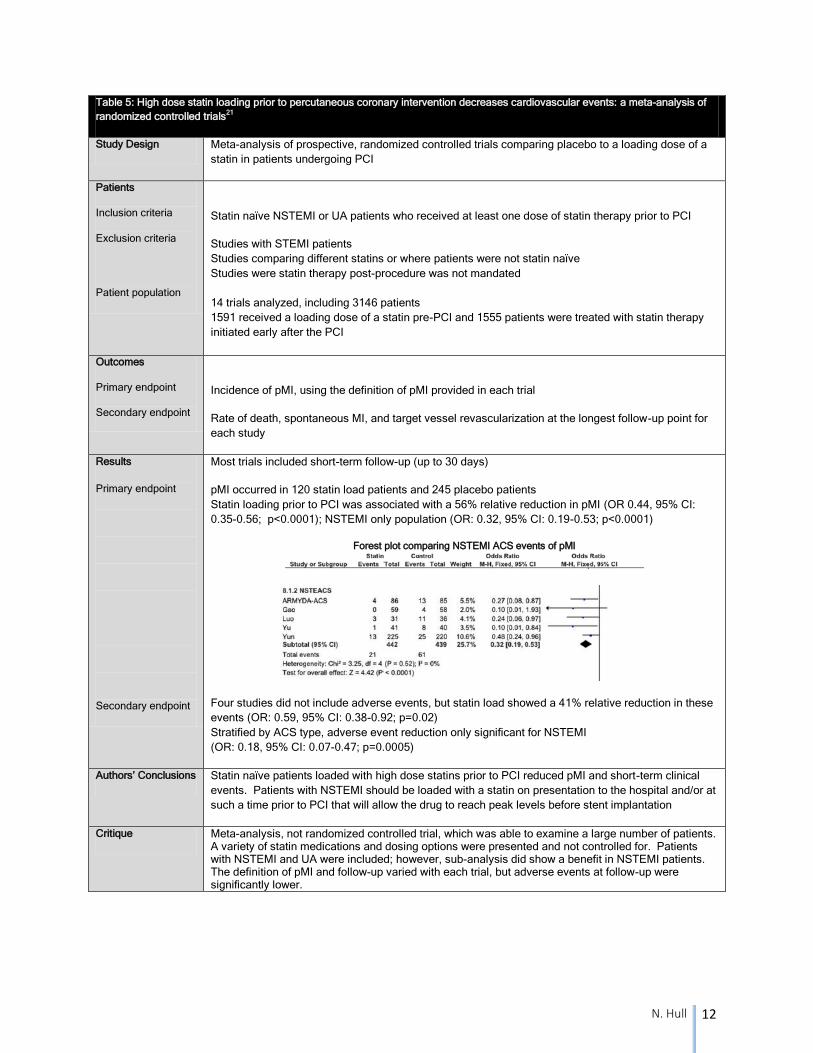
Table 5: High dose statin loading prior to percutaneous coronary intervention decreases cardiovascular events: a meta-analysis of
randomized controlled trials21
Study Design Meta-analysis of prospective, randomized controlled trials comparing placebo to a loading dose of a
statin in patients undergoing PCI
Patients
Inclusion criteria
Exclusion criteria
Patient population
Statin naïve NSTEMI or UA patients who received at least one dose of statin therapy prior to PCI
Studies with STEMI patients
Studies comparing different statins or where patients were not statin naïve
Studies were statin therapy post-procedure was not mandated
14 trials analyzed, including 3146 patients
1591 received a loading dose of a statin pre-PCI and 1555 patients were treated with statin therapy
initiated early after the PCI
Outcomes
Primary endpoint
Secondary endpoint
Incidence of pMI, using the definition of pMI provided in each trial
Rate of death, spontaneous MI, and target vessel revascularization at the longest follow-up point for
each study
Results
Primary endpoint
Secondary endpoint
Most trials included short-term follow-up (up to 30 days)
pMI occurred in 120 statin load patients and 245 placebo patients
Statin loading prior to PCI was associated with a 56% relative reduction in pMI (OR 0.44, 95% CI:
0.35-0.56; p<0.0001); NSTEMI only population (OR: 0.32, 95% CI: 0.19-0.53; p<0.0001)
Forest plot comparing NSTEMI ACS events of pMI
Four studies did not include adverse events, but statin load showed a 41% relative reduction in these
events (OR: 0.59, 95% CI: 0.38-0.92; p=0.02)
Stratified by ACS type, adverse event reduction only significant for NSTEMI
(OR: 0.18, 95% CI: 0.07-0.47; p=0.0005)
Authors’ Conclusions Statin naïve patients loaded with high dose statins prior to PCI reduced pMI and short-term clinical
events. Patients with NSTEMI should be loaded with a statin on presentation to the hospital and/or at
such a time prior to PCI that will allow the drug to reach peak levels before stent implantation
Critique Meta-analysis, not randomized controlled trial, which was able to examine a large number of patients. A variety of statin medications and dosing options were presented and not controlled for. Patients with NSTEMI and UA were included; however, sub-analysis did show a benefit in NSTEMI patients. The definition of pMI and follow-up varied with each trial, but adverse events at follow-up were significantly lower.
N. Hull 13
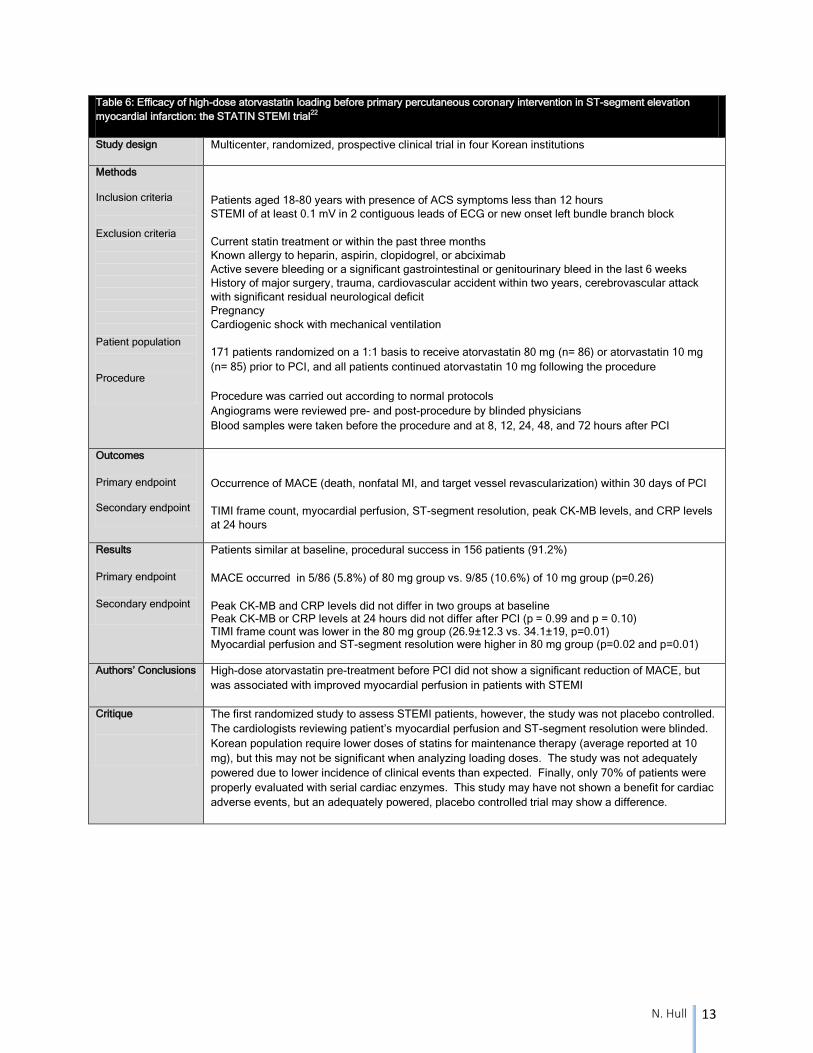
Table 6: Efficacy of high-dose atorvastatin loading before primary percutaneous coronary intervention in ST-segment elevation
myocardial infarction: the STATIN STEMI trial22
Study design Multicenter, randomized, prospective clinical trial in four Korean institutions
Methods
Inclusion criteria Exclusion criteria Patient population
Procedure
Patients aged 18-80 years with presence of ACS symptoms less than 12 hours
STEMI of at least 0.1 mV in 2 contiguous leads of ECG or new onset left bundle branch block
Current statin treatment or within the past three months
Known allergy to heparin, aspirin, clopidogrel, or abciximab
Active severe bleeding or a significant gastrointestinal or genitourinary bleed in the last 6 weeks
History of major surgery, trauma, cardiovascular accident within two years, cerebrovascular attack
with significant residual neurological deficit
Pregnancy
Cardiogenic shock with mechanical ventilation
171 patients randomized on a 1:1 basis to receive atorvastatin 80 mg (n= 86) or atorvastatin 10 mg
(n= 85) prior to PCI, and all patients continued atorvastatin 10 mg following the procedure
Procedure was carried out according to normal protocols
Angiograms were reviewed pre- and post-procedure by blinded physicians
Blood samples were taken before the procedure and at 8, 12, 24, 48, and 72 hours after PCI
Outcomes
Primary endpoint
Secondary endpoint
Occurrence of MACE (death, nonfatal MI, and target vessel revascularization) within 30 days of PCI
TIMI frame count, myocardial perfusion, ST-segment resolution, peak CK-MB levels, and CRP levels
at 24 hours
Results
Primary endpoint
Secondary endpoint
Patients similar at baseline, procedural success in 156 patients (91.2%)
MACE occurred in 5/86 (5.8%) of 80 mg group vs. 9/85 (10.6%) of 10 mg group (p=0.26)
Peak CK-MB and CRP levels did not differ in two groups at baseline Peak CK-MB or CRP levels at 24 hours did not differ after PCI (p = 0.99 and p = 0.10) TIMI frame count was lower in the 80 mg group (26.9±12.3 vs. 34.1±19, p=0.01) Myocardial perfusion and ST-segment resolution were higher in 80 mg group (p=0.02 and p=0.01)
Authors’ Conclusions High-dose atorvastatin pre-treatment before PCI did not show a significant reduction of MACE, but
was associated with improved myocardial perfusion in patients with STEMI
Critique
The first randomized study to assess STEMI patients, however, the study was not placebo controlled.
The cardiologists reviewing patient’s myocardial perfusion and ST-segment resolution were blinded.
Korean population require lower doses of statins for maintenance therapy (average reported at 10
mg), but this may not be significant when analyzing loading doses. The study was not adequately
powered due to lower incidence of clinical events than expected. Finally, only 70% of patients were
properly evaluated with serial cardiac enzymes. This study may have not shown a benefit for cardiac
adverse events, but an adequately powered, placebo controlled trial may show a difference.
N. Hull 14
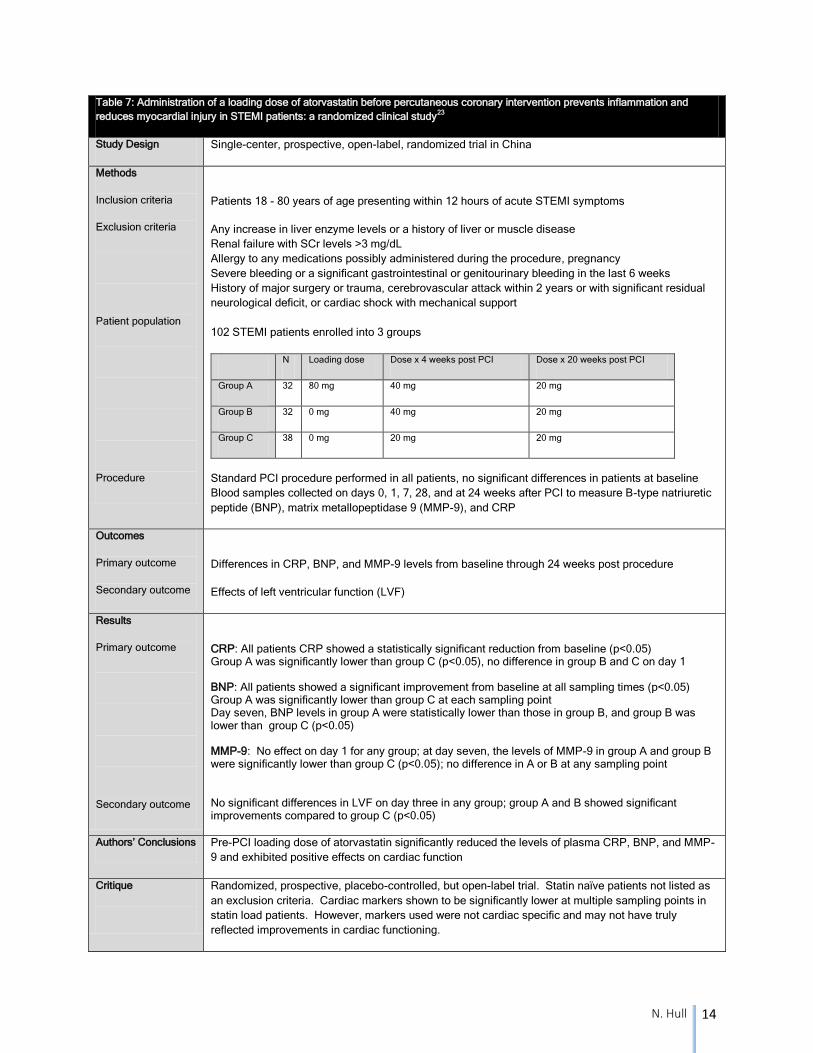
Table 7: Administration of a loading dose of atorvastatin before percutaneous coronary intervention prevents inflammation and
reduces myocardial injury in STEMI patients: a randomized clinical study23
Study Design Single-center, prospective, open-label, randomized trial in China
Methods
Inclusion criteria
Exclusion criteria
Patient population
Procedure
Patients 18 - 80 years of age presenting within 12 hours of acute STEMI symptoms
Any increase in liver enzyme levels or a history of liver or muscle disease
Renal failure with SCr levels >3 mg/dL
Allergy to any medications possibly administered during the procedure, pregnancy
Severe bleeding or a significant gastrointestinal or genitourinary bleeding in the last 6 weeks
History of major surgery or trauma, cerebrovascular attack within 2 years or with significant residual
neurological deficit, or cardiac shock with mechanical support
102 STEMI patients enrolled into 3 groups
N Loading dose Dose x 4 weeks post PCI Dose x 20 weeks post PCI
Group A 32 80 mg 40 mg 20 mg
Group B 32 0 mg 40 mg 20 mg
Group C 38 0 mg 20 mg 20 mg
Standard PCI procedure performed in all patients, no significant differences in patients at baseline
Blood samples collected on days 0, 1, 7, 28, and at 24 weeks after PCI to measure B-type natriuretic
peptide (BNP), matrix metallopeptidase 9 (MMP-9), and CRP
Outcomes
Primary outcome
Secondary outcome
Differences in CRP, BNP, and MMP-9 levels from baseline through 24 weeks post procedure
Effects of left ventricular function (LVF)
Results
Primary outcome
Secondary outcome
CRP: All patients CRP showed a statistically significant reduction from baseline (p<0.05) Group A was significantly lower than group C (p<0.05), no difference in group B and C on day 1 BNP: All patients showed a significant improvement from baseline at all sampling times (p<0.05) Group A was significantly lower than group C at each sampling point Day seven, BNP levels in group A were statistically lower than those in group B, and group B was lower than group C (p<0.05) MMP-9: No effect on day 1 for any group; at day seven, the levels of MMP-9 in group A and group B were significantly lower than group C (p<0.05); no difference in A or B at any sampling point
No significant differences in LVF on day three in any group; group A and B showed significant improvements compared to group C (p<0.05)
Authors’ Conclusions Pre-PCI loading dose of atorvastatin significantly reduced the levels of plasma CRP, BNP, and MMP-
9 and exhibited positive effects on cardiac function
Critique
Randomized, prospective, placebo-controlled, but open-label trial. Statin naïve patients not listed as
an exclusion criteria. Cardiac markers shown to be significantly lower at multiple sampling points in
statin load patients. However, markers used were not cardiac specific and may not have truly
reflected improvements in cardiac functioning.
N. Hull 15
I. Additional study24
A. ARMYDA-RECAPTURE trial reviewed patients currently taking a daily statin and
assessed if they benefited from re-loading with a statin medication
B. Multicenter, randomized, prospective, double-blind clinical trial performed in Italian
patients with NSTEMI on statin therapy for at least 30 days
C. Given atorvastatin 80 mg 12 hours before coronary angiography and 40 mg dose 2 hours
before the procedure
D. MACE noted in 7/192 of treatment arm (3.7%) versus 18/191 (9.4%) of the placebo
group, p=0.037
E. One of few studies to analyze patients on existing statin therapy
F. Of note, this is another study to reinforce the benefits of statin loading in NSTEMI ACS
patients undergoing PCI
CONCLUSION
I. Answering the clinical question
A. Is a statin load appropriate for patients undergoing PCI after an acute coronary event?
i. Based on the existing literature, administration of atorvastatin prior to a PCI in
both STEMI and NSTEMI patients should be highly considered
ii. Studies reviewed show beneficial outcomes in NSTEMI patients up to 30 days
after PCI
iii. The data available does not provide as clear of a picture to base
recommendations for STEMI treatment
iv. Although the role is not clearly defined for STEMI patients, no studies showed
significant adverse events
a) Thus, one should still consider utilization of atorvastatin prior to PCI in
the management of STEMI
B. When should therapy be initiated? What dose and dosing schedule is beneficial? i. Based on the evidence provided, 80 mg of atorvastatin should be administered
12 hours prior to PCI and an additional 40 mg dose given two hours prior
II. Recommendations A. NSTEMI patients
i. Non-emergent, early invasive strategy a) Load the patient with atorvastatin 80 mg 12 hours prior and an additional
40 mg two hours prior to PCI ii. Emergent, invasive strategy
a) Assess the time before intervention b) Consider giving one 80 mg dose if more than two hours between taking
medication and procedure iii. Conservative, medical management strategy
a) Continue high dose statin for secondary prevention b) If PCI scheduled for future date, load the patient with atorvastatin 80 mg
12 hours prior and an additional 40 mg two hours prior to PCI B. STEMI patients
i. Assess the time before intervention ii. Consider giving one 80 mg dose if more than two hours between taking
medication and procedure, even if the patient was treated with fibrinolytic therapy followed by PCI
N. Hull 16
REFERENCES
1) Spinler S and De Denus S. Chapter 18. Acute Coronary Syndromes. In: DiPiro JT, Talert RL, Yee GC, Matzke GR, Wells
GR, Wells BG, Posey LM, eds. Pharmacotherapy: A Pathophysiologic Approach. 8th ed. New York: McGraw-Hill; 2012.
2) Roger V, Go A, Lloyd-Jones D, et al. Heart disease and stroke statistics—2012 update: a report from the American Heart
Association. Circulation. 2012;125:e2-e220.
3) Antman E and Loscalzo J. Chapter 245. ST-segment elevation myocardial infarction. In: Longo D, Fauci A, Kasper D,
Hauser S, Jameson J, Loscalzo J, eds. Harrison’s Principles of Internal Medicine. 18th ed. New York: McGraw-Hill; 2012.
4) Trost J and Lange R. Treatment of acute coronary syndrome: Part 2: ST-segment elevation myocardial infarction. Crit
Care Med. 2012;40(6):1939-1945.
5) Gara P, Kushner F, Ascheim D, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial
infarction. Circulation. 2013;127:e362-e425.
6) Trost J and Lange R. Treatment of acute coronary syndrome: Part 1: Non-ST-segment acute coronary syndrome. Crit
Care Med. 2011;39(10):2346-2353.
7) Cannon C and Braunwald E. Chapter 244. Unstable angina and non-ST-segment elevation myocardial infarction. In:
Longo D, Fauci A, Kasper D, Hauser S, Jameson J, Loscalzo J, eds. Harrison’s Principles of Internal Medicine. 18th ed.
New York: McGraw-Hill; 2012.
8) Jneid H, Anderson J, Wright R, et al. 2012 ACCF/AHA focused update of the guideline for the management of patients
with unstable angina/non-ST elevation myocardial infarction. Circulation. 2012;126:875-910.
9) Libby P. Mechanisms of acute coronary syndromes and their implications for therapy. NEJM. 2013;368(21):2004-2013.
10) Lewandrowski K, Chen A, Januzzi J. Cardiac markers for myocardial infarction. Am J Clin Pathol. 2012;118(Suppl1):S93-
S99.
11) Faxon D and Bhatt D. Chapter 246. Percutaneous coronary interventions and other interventional procedures. In: Longo
D, Fauci A, Kasper D, Hauser S, Jameson J, Loscalzo J, eds. Harrison’s Principles of Internal Medicine. 18th ed. New
York: McGraw-Hill; 2012.
12) Lansky A and Stone G. Periprocedural myocardial infarction: prevalence, prognosis, and prevention. Circ Cardiovasc
Interv. 2010;3:602-610.
13) Leoncini M, Toso A, Maioli M, et al. Statin treatment before percutaneous coronary intervention. J Thorac Dis.
2013;5(3):335-342.
14) Talbert R. Chapter 28. Dyslipidemia. In: DiPiro JT, Talert RL, Yee GC, Matzke GR, Wells GR, Wells BG, Posey LM, eds.
Pharmacotherapy: A Pathophysiologic Approach. 8th ed. New York: McGraw-Hill; 2012.
15) Lipitor [package insert]. New York, NY: Parke-Davis Division of Pfizer Inc; 2014.
16) Davignon J. Beneficial cardiovascular pleiotropic effects of statins. Circulation. 2004;109:III-39-III-43.
17) Simona M, Giuseppe P, Cannon C, et al. Preprocedural statin therapy to prevent myocardial damage in percutaneous
coronary intervention. Crit Path Cardio. 2010;9(1):19-22.
18) Briguori C, Visconti G, Focaccio A, et al. Novel approaches for preventing or limiting events (Naples) II trial. JACC.
2009;54(23):2157-2163.
19) Yu X, Zhang H, Ren S, et al. Effects of loading dose of atorvastatin before percutaneous coronary intervention on
periprocedural myocardial injury. Coronary Artery Disease. 2001;22:87-91.
20) Giuseppe P, Vincenzo P, Giuseppe C, et al. Atorvastatin pretreatment improves outcomes in patients with acute coronary
syndromes undergoing early percutaneous coronary intervention: results of the ARMYDA-ACS randomized trial. JACC.
2007;49(12):1272-1278.
21) Benjo A, El-Hayek G, Messerli F, et al. High dose statin loading prior to percutaneous coronary intervention decreases
cardiovascular events: a meta-analysis of randomized controlled trials. Catheter Cardio Inte. 2013. DOI:
10.1002/ccd.25302.
22) Kim J, Kim J, Choi D, et al. Efficacy of high-dose atorvastatin loading before primary percutaneous coronary intervention
in ST-segment elevation myocardial infarction: The STATIN STEMI trial. J Am Coll Cardiol Intv 2010;3:332-339.
23) Liu H, Yang Y, Yang S, et al. Administration of a loading dose of atorvastatin before percutaneous coronary intervention
prevents inflammation and reduces myocardial injury in STEMI patients: a randomized clinical study. Clin Ther
2013;35:261-272.
24) Di Sciascio G, Patti G, Pasceri V, et al. Efficacy of atorvastatin reload in patients on chronic statin therapy undergoing
percutaneous coronary intervention. JACC. 2009;54(6):558-565.
N. Hull 17
APPENDIX
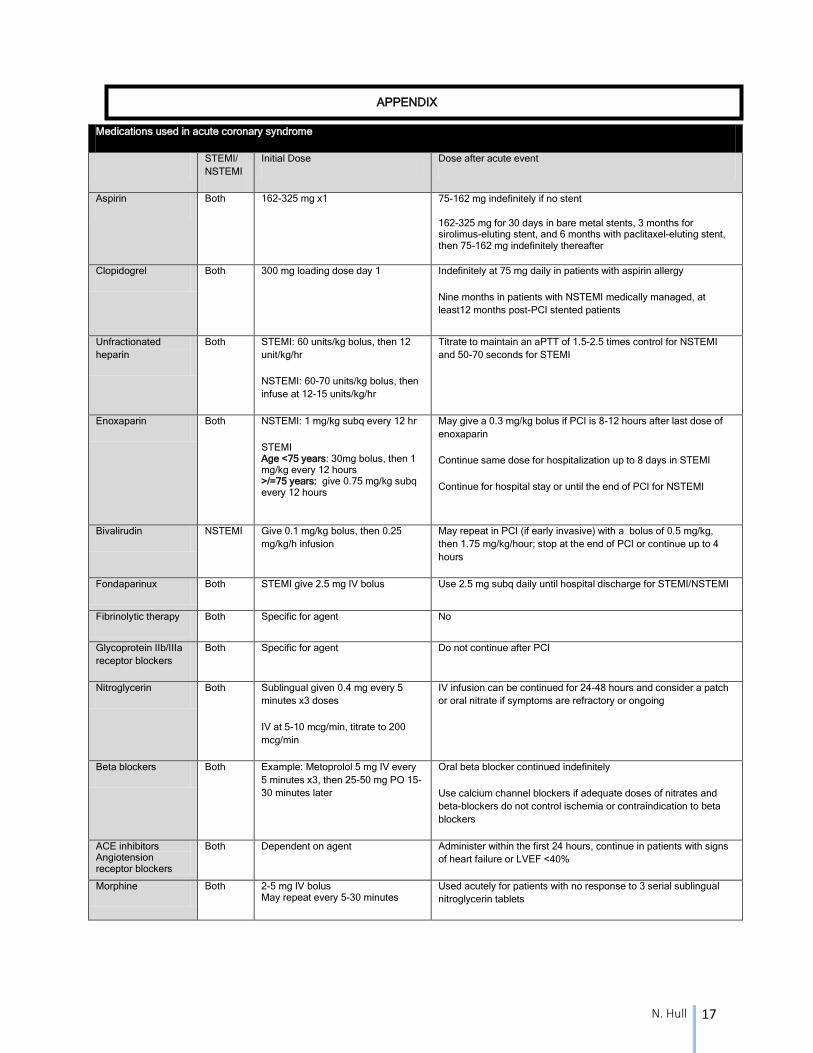
Medications used in acute coronary syndrome
STEMI/
NSTEMI
Initial Dose Dose after acute event
Aspirin Both 162-325 mg x1
75-162 mg indefinitely if no stent
162-325 mg for 30 days in bare metal stents, 3 months for sirolimus-eluting stent, and 6 months with paclitaxel-eluting stent, then 75-162 mg indefinitely thereafter
Clopidogrel Both 300 mg loading dose day 1 Indefinitely at 75 mg daily in patients with aspirin allergy
Nine months in patients with NSTEMI medically managed, at
least12 months post-PCI stented patients
Unfractionated
heparin
Both STEMI: 60 units/kg bolus, then 12
unit/kg/hr
NSTEMI: 60-70 units/kg bolus, then
infuse at 12-15 units/kg/hr
Titrate to maintain an aPTT of 1.5-2.5 times control for NSTEMI
and 50-70 seconds for STEMI
Enoxaparin Both NSTEMI: 1 mg/kg subq every 12 hr
STEMI Age <75 years: 30mg bolus, then 1 mg/kg every 12 hours >/=75 years: give 0.75 mg/kg subq every 12 hours
May give a 0.3 mg/kg bolus if PCI is 8-12 hours after last dose of
enoxaparin
Continue same dose for hospitalization up to 8 days in STEMI
Continue for hospital stay or until the end of PCI for NSTEMI
Bivalirudin NSTEMI Give 0.1 mg/kg bolus, then 0.25
mg/kg/h infusion
May repeat in PCI (if early invasive) with a bolus of 0.5 mg/kg,
then 1.75 mg/kg/hour; stop at the end of PCI or continue up to 4
hours
Fondaparinux Both STEMI give 2.5 mg IV bolus Use 2.5 mg subq daily until hospital discharge for STEMI/NSTEMI
Fibrinolytic therapy Both Specific for agent No
Glycoprotein IIb/IIIa
receptor blockers
Both Specific for agent Do not continue after PCI
Nitroglycerin Both Sublingual given 0.4 mg every 5
minutes x3 doses
IV at 5-10 mcg/min, titrate to 200
mcg/min
IV infusion can be continued for 24-48 hours and consider a patch
or oral nitrate if symptoms are refractory or ongoing
Beta blockers Both Example: Metoprolol 5 mg IV every
5 minutes x3, then 25-50 mg PO 15-
30 minutes later
Oral beta blocker continued indefinitely
Use calcium channel blockers if adequate doses of nitrates and
beta-blockers do not control ischemia or contraindication to beta
blockers
ACE inhibitors Angiotension receptor blockers
Both Dependent on agent Administer within the first 24 hours, continue in patients with signs
of heart failure or LVEF <40%
Morphine Both 2-5 mg IV bolus May repeat every 5-30 minutes
Used acutely for patients with no response to 3 serial sublingual
nitroglycerin tablets
Related Documents