-
7/27/2019 Antibioterapie Model Poole
1/60
Michael D. Poole, MD, PhD
-
7/27/2019 Antibioterapie Model Poole
2/60
-
7/27/2019 Antibioterapie Model Poole
3/60
-
7/27/2019 Antibioterapie Model Poole
4/60
Study design: What to payattention to
Pharmacodynamic/pharmacokinetic properties
Bacterial elimination studies (requires a culture
during or at end of therapy). Clinical studies can be (and commonly are)
manipulated to suggest bacteriologic efficacy whenit may not be there.
-
7/27/2019 Antibioterapie Model Poole
5/60
What about all the papers
and studies that suggestsomething different thanguideline recommendations?
There are different ways to performsinusitis trials
Clinical diagnosis, clinical endpointBacteriologic diagnosis, clinical endpoint
Bacteriologic diagnosis, bacteriologic endpoint
-
7/27/2019 Antibioterapie Model Poole
6/60
Sample Sizes in SinusitisComparing Antibiotic A with 90% killing rate with
Antibiotic B with a killing rate of
:*
Clinical Diagnosis
Clinical endpointBacteriologic
diagnosis,
Clinical endpoint
Bacteriologicdiagnosis,
Bacteriologic
endpoint50% 1,900 543 14660% 3,256 912 22970% 7,039 1925 43880% 26,958 7142 1403
Poole, MD, et al.
Abstr Amer Acad OtolaryngolAnn Meeting, 2002
*Based on an alpha = 0.05; beta 0.1; Non-bacterial,
non-resolving = 10%, non-bacterial, resolving (viral) = 40%,Spontaneous resolution of all bacterial cases = 50%
-
7/27/2019 Antibioterapie Model Poole
7/60
Minimum Inhibitory Concentration
(MIC)
64 32 16 8 4 2 1 0.5 0.25 Control(no antibiotic)
MIC
-
7/27/2019 Antibioterapie Model Poole
8/60
-
7/27/2019 Antibioterapie Model Poole
9/60
Penicillin-resistant S. pneumoniaeDefined
NCCLS document M100-S12. 2002.
penicillin-susceptible = MIC 2 g/mL
Penicillin-resistant S. pneumoniaeisdefined as penicillin MIC of >2 g/mL
-
7/27/2019 Antibioterapie Model Poole
10/60
20% R1219.9% R>1
11.9% R1% R
15.7%
15.1%
17.7%
12.6%9.6%
19.1%
18.5%
22.8% 22.5%
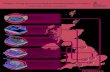
Regional S. pneumoniae Penicillin Resistance:TRUST 7 (2002-2003) Respiratory Season
Penicillin resistance defined as an MIC of 2 mg/ml
Data on file, Ortho-McNeil Pharmaceutical, Inc. In vitro activity does not necessarily correlate with clinical results.
National PenicillinResistance Rate = 17.3%
-
7/27/2019 Antibioterapie Model Poole
11/60
25.6%
25.2%
15.2%
32.5%
40.6% 31.7%
25.2%17.6%
31.9%
20% R1219.9% R>1
11.9% R1% R
Regional S. pneumoniae Azithromycin Resistance:TRUST 7 (2002-2003) Respiratory Season
Azithromycin resistance defined as an MIC of 2 mg/ml
Data on file, Ortho-McNeil Pharmaceutical, Inc. In vitro activity does not necessarily correlate with clinical results.
National AzithromycinResistance Rate = 27.5%
-
7/27/2019 Antibioterapie Model Poole
12/60
S. pneum on iaeAntibiogram: Sinus IsolatesTRUST 6 & 7 (2002-2003), N = 390
MIC90 MIC90Antimicrobial (mg/mL) Interp Cata % S % I % RLevofloxacin 1 S 99.2 0.0 0.8
Amox/clav 8 R 86.2 3.3 10.5
Cefuroxime 8 R 59.2 4.6 36.2
Erythromycin 16 R 58.7 0.0 41.3
Azithromycin >32 R 58.7 0.3 41.0
TMP-SMX >4 R 55.9 9.5 34.6
Penicillin 4 R 51.5 18.2 30.3
a: Interpretive category result of S, I, R based on MIC90 value (mg/ml).
Sahm et al. ICAAC2003, abstr C2-924. Data on file, Ortho-McNeil Pharmaceutical,
Inc.
In vitro activity does not necessarily correlate with clinical results.
-
7/27/2019 Antibioterapie Model Poole
13/60
3.1 2.9 2.7 2.1 2.8
169.7
8.2 7.4
12.7 15.3 14 12.2 10.7
1
0.8
3.2 6.82.5
6.37.3
14.5 19.7
12.34.8
1.64.1
9.9
10.1
11.3
7.7
10.4
11.2
0
5
10
15
20
2530
35
40
45
50
1985
1986
1987
1988-1989
1990-1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
Intermediate (MICs 0.12 to 1.0 g/mL)
Resistant (MICs 4.0 g/mL)Resistant (MICs = 2.0 g/mL)
Doern GV.Am J Med. 1995;99(suppl 6B):S3S7.
Jacobs MR, et al.Antimicrob Agents Chemother. 1999;43:19011908.
Jacobs MR, et al.ICAAC1999. Abstract C-61.Alexander Project 1999-2000. GlaxoSmithKline, data on file.
No
nsusceptibleis
olates(%)
Penicillin-nonsusceptibleS. pneumoniae:
U.S. Surveillance1985-2000
-
7/27/2019 Antibioterapie Model Poole
14/60
0
5
10
15
20
1992 1993 1994 1995 1996 1997 1998 1999 2000
MIC 2 g/mL
MIC 4 g/mL
MIC 8 g/mL
MIC 16 g/mL
Distribution of Penicillin MICs inS. pneumoniaeIs Changing:
U.S. 1992-2000
Data on file. Alexander Project. GlaxoSmithKline.
Year
P
ercentageofstrains
-
7/27/2019 Antibioterapie Model Poole
15/60
Amoxicillin in Middle Ear Fluid
Current NCCLS
amoxicillinbreakpoint for
S. pneumoniae
Adapted from Seikel K, et al.Pediatr Infect Dis J. 1997;16:710
711;Adapted from Harrison CJ, et al.Pediatr Infect Dis J. 1998;17:657658.
Time (h)
C
oncentration(g/m
L)
8
7
6
5
4
3
21
0
35 mg/kg (Seikel)45 mg/kg (Seikel)
0 1 2 3
30 mg/kg (Harrison)13 mg/kg (Harrison)
-
7/27/2019 Antibioterapie Model Poole
16/60
0
10
20
30
40
50
60
MIC (g/mL)0.0
15
0.0
3
0.0
6
0.1
2
0.2
50.5 1 2 4 8 1
6
>16
%o
fstrains
Amoxicillin/Clavulanate
Data on file. Alexander Project 2000..
M. catarrhalis
S. pneumoniae
H. infl uenzae
Shaded floor represents PK/PD breakpoint
-
7/27/2019 Antibioterapie Model Poole
17/60
There is no rational reason to use low/regular
doses of amoxicillin (or amox-clavulanate):Pediatrics 80-100 mg/kg, Adults 3-4 g/daily,divided BID
Higher doses (of either) will markedly reduce H.influenzaefailures) (15-25%) and some S.pneumoniaefailures (~5%). Hemophilusfailuresare related to the less than optimal intrinsic activity
of amoxicillin against beta-lactamase negative H.influenzae.
Hemophilus influenzaeis the most common failure
cause for amoxicillin-clavulanate.
-
7/27/2019 Antibioterapie Model Poole
18/60
-
7/27/2019 Antibioterapie Model Poole
19/60
Data from A lexander Proj ect 1999-2000, analyzed by Mic hael Jacob s
100 10094
98 100
77 83
Amox
(HD)
Ceftria
x
cefdinir
(QD)
Cefdinir
(BID)
Cefprozil
Cefuroxime
cefa
clor
Pen -Sn = 4,254
Proportion of Susceptible Pnc Isolates that areSusceptible to High Dose Amox, Ceftriaxone and Oral
Cephalosporins, (by Pk/Pd Breakpoints)
100 99
25
59
73
77
22
Amox
(HD)
Ceftria
x
cefdinir
(QD)
Cefdinir
(BID)
Cefprozil
Cefuroxime
cefa
clor
Pen -In = 905
87
78
0 0 0 0 0
Amox
(HD)
Ceftria
x
cefdinir
(QD)
Cefdinir
(BID)
Cefprozil
Cefuroxime
cefa
clor
Pen -Rn = 1,250
n = 6,409
-
7/27/2019 Antibioterapie Model Poole
20/60
There is no defensible role for cefprozil, loracarbef, and
cefaclor in ear and sinus infection.
NO oral cephalosporin has clinical activity against penicillinresistant S. pneumoniae.
Cefpodoxime (Vantin) is the most active of the oralcephalosporins, especially for amoxicillin or amox-clavulanate failures.
Cefdinir (Omnicef) is the best choice for 1st line therapy ofchildren, but is likely less effective than high-doseamoxicillin.
Ceftriaxone (Rocephin), given at usual IV/doses for 3-7days, is highly effective for the usual pathogens, includingmost ceftriaxone and penicillin resistantS. pneumoniae.
-
7/27/2019 Antibioterapie Model Poole
21/60
-
7/27/2019 Antibioterapie Model Poole
22/60
0
10
20
30
40
50
60
70
80
90
100
Pen-S Pen-I Pen-R
Erythromycin-resistant Clindamycin-resistant TMP/SMX-resistant
Penicillin-nonsusceptibleS. pneumoniaeis Frequently Cross-
resistant to Other Classes of Antibiotic*
Resistantisolate
s(%)
(n=2,756) (n=848) (n=589)
Hoban DJ, et al. Clin Inf Dis. 2000:32(suppl 2):S81-S93.
Pen-S, MIC 0.06 g/mL; Pen-I, MIC 0.12-1 g/mL; Pen-R, MIC 2 g/mL
* NCCLS breakpoints used
-
7/27/2019 Antibioterapie Model Poole
23/60
Distribution of macrolide MICs amongH. in fluenzae(Alexander study 1997-2000)
97% baseline
1% hyper-
susceptible
2% hyper-
resistant
Macrolide Susceptibility ofH. influenzae
-
7/27/2019 Antibioterapie Model Poole
24/60
Resistance Mechanisms
Strains Efflux RibosomalMutation
Hypersusceptible (-) (-)Baseline (+) (-)High level resistant (+) (+)
Conclusion: Macrolide and KetolideResistance in H. influenzae
Peric, Applebaum, et al. 2003
-
7/27/2019 Antibioterapie Model Poole
25/60
Telithromycin
0
10
20
30
40
50
6070
80
%o
fstrains
MIC (g/mL)
0
0.008
0.015
0.0 3
0.0 6
0.1 2
0.2 5
0.5 1 2 4 >
4
M. catarrhal is
S. pneumoniae
H. influenzae
Adapted from:Nagai K, et al.Antimicrob Agents Chemother. 2002;46:371377.Pankuch GA, et al.Antimicrob Agents Chemother. 1998;42:30323034.
Shaded floor represents PK/PD breakpointGreen represents susceptible range
-
7/27/2019 Antibioterapie Model Poole
26/60
Telithromycin (Ketek)
Technically, a ketolide, derived from clarithromycin
Has an additional binding ribosomal binding site onthe molecule, so it appears to be active against
most of the macrolide-resistant pneumococci.
Similar to the macrolides, the MICs to Hemophilusare high enough that the efficacy is poor to fair.
Some concerns about drug-drug interactions.
If all of the above are true, it is somewhat lesseffective than amoxicillin.
-
7/27/2019 Antibioterapie Model Poole
27/60
Macrolides and Ketolides have activity against H.influenzaethat is equal to or near that of placebo(ear and sinus disease) Macrolide resistant S.pneumoniaeare common.
They are significantly less effective than high doseamoxicillin for previously untreated patients;markedly less effective than quinolones and amox-
clavulanate for second line therapy. Telithromycin (Ketek) has somewhat better activity
than macrolides against S. pneumoniae.
-
7/27/2019 Antibioterapie Model Poole
28/60
R i l L fl i
-
7/27/2019 Antibioterapie Model Poole
29/60
1.0%
1.0%
0.9%
0.9%
0.9% 0.7%
0.9%1.7%
0.7%
20% R1219.9% R>111.9% R1% R
Regional S. pneumon iaeLevofloxacinResistance:
TRUST 7 (2002-2003) Respiratory Season
Levofloxacin resistance defined as an MIC of 8 mg/mLData on file, Ortho-McNeil Pharmaceutical, Inc. In vitro activity does not necessarily correlate with clinical results.
National LevofloxacinResistance Rate = 0.96%
-
7/27/2019 Antibioterapie Model Poole
30/60
Similar Susceptibilities of Newer FluoroquinolonesAgainst S. pneumon iae
Antimicrobial %S %I %R
Canadian Bact Surv Netwk, Low, et al AAC 2002;46:1295-1301
Levofloxacin 99.0 0.1 0.9
Gatifloxacin 99.1 0.1 0.8Moxifloxacin 99.1 0.5 0.4
TRUST 7, USA (2002-2003), Data on file, Ortho-McNeil Pharmaceutical, Inc.
Levofloxacin 99.0 0.0 1.0
Gatifloxacin 99.1 0.1 0.8
Moxifloxacin 99.1 0.5 0.4
Low et al (2000 data): N= 2,245; TRUST 7 (2002-2003): N = 4, 377
-
7/27/2019 Antibioterapie Model Poole
31/60
Levafloxacin (Levaquin), 750 mg
Significantly improves an already very good PK/PDprofile.
Has been tested in the setting of a 5 day course inpneumonia and sinusitis.
Will likely supplant 500 mg qd dosing.
-
7/27/2019 Antibioterapie Model Poole
32/60
Implications of AntimicrobialPotency on Resistanced
Bigger is better!
Dead bugs
dont
become
RESISTANT!
-
7/27/2019 Antibioterapie Model Poole
33/60
Levofloxacin (Levaquin), gatifloxacin (Tequin), and
moxifloxacin (Avelox) are very active agents forrespiratory tract infections.
They are roughly equal (within 1-2%) in clinical
efficacy. There are some differences in adverse effects and
safety profiles.
Safety and resistance issues make them, ingeneral, appropriate for second line therapy.
We will see more short course trials of sinusitiswith good microbiologic outcome.
A i i bi l f Rhi i i i
-
7/27/2019 Antibioterapie Model Poole
34/60
Antimicrobials for Rhinosinusitis
Respiratory Quinolones (92%)
HD Amoxicillin/clavulanate (91%)
Amoxicillin/clavulanate (87%)
HD Amoxicillin (83%)
Cefpodoxime proxetil (81%)Cefixime (80%)
Cefuroxime axetil (80%)
Cefdinir (78%)
TMP/SMX (77%)
Cefprozil (70%)
Macrolides (68%)
Placebo (60%)
More effective,
More antibiotic use
Less effective,
Less antibiotic use
Sinus and Allergy Health Partnership.Otolaryng ol Head Neck Surg) 2004
/ d d
-
7/27/2019 Antibioterapie Model Poole
35/60
2004 AAP/AAFP RecommendedAntibacterial Agents for Initial
Treatment for AOM
Antibacterial
agents in past
month if age < 2
years or daycare
At diagnosis Clinically defined treatment failure at
48-72 hours after treatment
Recommended Recommended
No High-dose
amoxicillin
High-dose
amoxicillin/
clavulanate
or cefdinir;
or cefpodoxime;
or cefuroxime;
or ceftriaxone
Yes High-dose
amoxicillin or
amoxicillin/
clavulanate
High-dose
amoxicillin/
clavulanate
or cefdinir;
or cefpodoxime;
or cefuroxime;
or ceftriaxone
Ob ti O ti A tibi ti
-
7/27/2019 Antibioterapie Model Poole
36/60
Observation Option vs. AntibioticTherapy
Age Certain Diagnosis Uncertain Diagnosis
< 6 months Antibacterial therapy Antibacterial therapy
6 months-2 yrs Antibacterial therapy Antibacterial therapyif severe illness
Observe if non-severe
2 years Antibacterial therapyif severe illness
Observe if non-severe
Observe
Proportion of AOM Episodes Culture Positive for
-
7/27/2019 Antibioterapie Model Poole
37/60
Kilpi T. Pediatr Infect Dis J. 2001;20:654-662.
0
5
10
15
20
25
30
35
40
1 2 3 4 5 >5
H. influenzae
S. pneumoniae
Culturepo
sitive(%)
Episodes of AOM
Proportion of AOM Episodes Culture-Positive forH. influenzaeor S. pneumoniae
(Finland, 1994-1997)
N = 203 144 98 71 34 35
-
7/27/2019 Antibioterapie Model Poole
38/60
AOM is currently the best bacterial respiratory
infection to study.
Conjugated pneumococcal vaccines have changedAOM somewhat.
Only a few drugs are very efficacious for AOM:high dose Amox-clav, ceftriaxone
H. influenzaeis now our most important AOM
pathogenespecially for ENT patients.Most antibiotic failures are not failures.
We have been mis-informed about antibiotic
effectiveness in AOM.
-
7/27/2019 Antibioterapie Model Poole
39/60
S-Pnc
Non-S-Pnc
Hi
Hi BL+placebo
*For amoxicillin only
84%
52%
%p
ersistence *
Bacter io logic
Failure Rates on
Day 4-6 inAOM: Double Tap
Studies
Dagan,personal communication
-
7/27/2019 Antibioterapie Model Poole
40/60
Reasons why primary careclinicians think antibiotics fail
when they do not.
Misinterpret intercurrent infections as
failuresOME after AOM is characterized as a failure
Cases of OME are diagnosed as AOM and arecalled failures.
Cli i l R f AOM Withi
-
7/27/2019 Antibioterapie Model Poole
41/60
Leibovitz E, et al. Pediatr Infect Dis J. 2003;22:209-216.
Relapses vs. new infections determined forS. pneumon iaeby
PFGE and serotyping, and forHaemop hi lus inf luenzaeby PFGE
and -lactamase production
0
20
40
6080
100
C
linicalrelapse
(%)
n= 39 n = 38 n = 21 n = 10
Bacteriologic relapsesNew infections
Days 1-7 Days 8-14 Days 15-21 Days 22-28
Clinical Recurrences of AOM Within28 d After EOT
EOT = end of therapy.
-
7/27/2019 Antibioterapie Model Poole
42/60
Reasons why primary careclinicians think antibiotics fail
when they do not.
Misinterpret intercurrent infections as
failuresOME after AOM is characterized as a failure
Cases of OME are diagnosed as AOM and arecalled failures.
-
7/27/2019 Antibioterapie Model Poole
43/60
-
7/27/2019 Antibioterapie Model Poole
44/60
Reasons why primary careclinicians think antibiotics fail
when they do not.
Misinterpret intercurrent infections as
failuresOME after AOM is characterized as a failure
Cases of OME are diagnosed as AOM and arecalled failures.
-
7/27/2019 Antibioterapie Model Poole
45/60
Pediatric Chronic Sinusitis
2.5 year old boy with an 18 month history ofchronic sinusitis. Major symptoms includecongestion, rhinorrhea, poor sleeping, relapsingcough. No history of systemic or lower respiratoryinfections. 4-5 bouts of AOM, resolving onantibiotics.
On antibiotics almost monthly. Has had culturesthat grew DRSP and H. influenzae at various times.
Tested neg. for CF. Attends a small (7-10 kids)daycare.
-
7/27/2019 Antibioterapie Model Poole
46/60
Pediatric Chronic Sinusitis, cont
Family sought allergy referral: Had skin testing:negative. Had PneumoVax and antibody responsetest that showed varying levels to differentserotypes.
Has had two prior CTs, one last month. Oneshowed pan-sinusitis (taken while sick), othershowed scattered ethmoid and maxillary mucosal
thickening. Exam: Normal general exam. TMs retracted
without fluid. Nose: moderate mocupurulentsecretions. No polyps. Oropharynx normal.
2004
-
7/27/2019 Antibioterapie Model Poole
47/60
2004For Problematic Pediatric Sinusitis or AOM
Augmentin ES600 (90 mg/kg/d, BID)
For Augmentin failures. Cefpodoxime (Vantin).Then culture.
Clindamycin + ceftibuten (Cedax) or TMP-SMX orcefixime (Suprax)
High dose Amoxicillin + ceftibuten (Cedax) or TMP-SMX
Ceftriaxone + .(observation, high dose amoxicillin,more ceftriaxone)
For allergic/intolerant : macrolides (mild cases).Consider rifampin (20 mg/kg/d) plus clindamycin orTMP-SMX for severe AOM.
-
7/27/2019 Antibioterapie Model Poole
48/60
-
7/27/2019 Antibioterapie Model Poole
49/60
The Psycho-neuroses ofChronic Pediatric Sinusitis
The child is usually no different than many otherchildren who have same clinical/radiographicfindings without the level of anxiety.
The family has generally been misinformed andmisled about a number of issues.
Re-education is time consuming.
Areas of Dis-informaton
-
7/27/2019 Antibioterapie Model Poole
50/60
Areas of Dis informaton
He/she has the same infection back again.
Wrong. Symptoms and presentation may be the same
The sinuses are blocked up.
A simplistic pro-surgical explanation that is generally
wrong.Nothing works for him/her.
Wrong
The CT abnormalities prove how serious it is.Wrong
It is all due to his/her allergies.
Wrong
Managing the child (and family) with
-
7/27/2019 Antibioterapie Model Poole
51/60
Managing the child (and family) withchronic sinusitis
Manage each episode individually (Do not use thesame shotgun poly-pharmacy for every episode.)
Prospectively, the number of infections in going tobe exaggerated over historical counts.
Have someone in the office with the time andpatience to talk the family down when the childbecomes ill not over-reacting.
Dont lower your antibiotic prescribing thresholdbecause of the past history.
Obtain cultures when therapy may not be working...
Patience
-
7/27/2019 Antibioterapie Model Poole
52/60
Causes & Treatment Strategies for
-
7/27/2019 Antibioterapie Model Poole
53/60
Causes & Treatment Strategies forChronic Rhinosinusitis
Adapted from Benninger, et al. Otolaryngol Head Neck Surg , 2003;129:S1-32.
CRS
Bacteria
Super-antigenOsteitis Allergy
Fungi
TreatEtiology-Antibiotics-Antifungals-MechanicaldebridementAttenuateInflammation-Steroids-Anti-IL-5-IL-4R-Anti-IgE-Immunotherapy-Anti-leukotrienes-Macrolides
IL-5, IL-4IL-8, IF-gGM-CSF
Bio-films
P i O i i
-
7/27/2019 Antibioterapie Model Poole
54/60
Post-operative OpportunisticBacterial Maxillary Sinusitis
What causes it?
What sinuses are involved?
Why is this something different than whatthey originally had?
Treatment?
-
7/27/2019 Antibioterapie Model Poole
55/60
Rising Incidence of CA-MRSA
-
7/27/2019 Antibioterapie Model Poole
56/60
Rising Incidence of CA-MRSA(Community Acquired Methicillin Resistant
Staph aureus)
Rapid increase in community acquired strains MOREVirulent. More transmissable.
Can be resistant to macrolides, clindamycin, quinolones,
sulfasalmost everything but vanco and rifampinWarningIf the strain tests resistant to erythromycin
(even if tested Suscept to clinda), resistance to clindamay be inducibleemerges during therapy
Most can be treated with drainage,TMP-SMX + rifampin,
Many are susceptible to clindamycin.
All are susceptible to Vancomycin
-
7/27/2019 Antibioterapie Model Poole
57/60
Although the risk is small, aminoglycosides should
not be used with non-intact TMs or used withappropriate consent.
From a microbiologic standpoint, there is no
significant clinical difference between ciprofloxacinand ofloxacin.
The presence of a potent steroid (dexamethasone)appears to have significant positive impact of
treatment of infections. Effect in surgery patientsis unknown.
A neutral pH drop (ofloxacin otic) may predispose
to yeast overgrowth.
Draining Ears: Resistant bugs
-
7/27/2019 Antibioterapie Model Poole
58/60
Draining Ears: Resistant bugs,Pseudomonas,
MRSA or Enterococcus
May have failed IVvancomycin!
Rx: Topical agents
Otic quinolones
Aminoglycosides
Forget susceptibilitytest results
Sudden Cardiac Death and Erythromycin
-
7/27/2019 Antibioterapie Model Poole
59/60
Sudden Cardiac Death and Erythromycin Looked at a cohort of Tennessee Medicaid patients:
1.2 million patient years, and 1476 cases of sudden
cardiac death
Patients on erythromycin had a 2 x rate of death.
Patients on erthromycin PLUS an strong inhibitor of
cytochrome P-450 had a 5.35 increase in rate. Nitro-imidazole antifungal agents, diltiazem, verapamil,
and troleandomycin
Presumptive mechanism of increased risk inprolongation of Q-T interval and subsequentarrythmias.
No increase with amoxicillin or prior erythromycin
Ray, WA et al. NEJM. 2004; 351 1089
-
7/27/2019 Antibioterapie Model Poole
60/60
Probable Implications
Large drug usage database analysis, whencombined with outcome data is a very potent new
tool.
This is probably the tip of the iceberg concerningcombinations of drugs that alter Q-T interval or arecompetitively metabolized.
With regard to antimicrobials, will likely increaseconcerns about erythromycin, clarithromycin, ?telithromycin, and the flouroquinolones (esp.moxifloxacin)