Annals i>f Oiiilogy, Rhinology & Ijiryngology 114( IO(:777-785. © 2(J0fi Annuls Publlshiitg Company. All rights reserved. Angular Vestibulo-ocular Reflex Gains Correlate With Vertigo Control After Intratympanic Gentamicin Treatment for Meniere's Disease Frank R. Lin, MD; Americo A. Migliaccio, PhD; Thomas Haslwanter, PhD; Lloyd B. Minor, MD; John P. Carey, MD Objectives: The objective of our study was to determine whether angular vestibulo-ocular reflex (aVOR) gains correlated with vertigo control after intratympanic genlamicin treatment for Meniere's disease. Methods: We conducted a prospective study of 18 subjects with unilateral Meniere's disease treated with intralympanic gentamicin injection and followed all subjects for I year. We measured the gain of the aVOR elicited by rapid rotary head thrusts in each of the canal planes for each subject before and after treatment with intratympanic gentamicin by using magnetic search coils to record eye movements. Results: During the follow-up period. II subjects ("single-treatment group": 61%) had eontrol of their vertigo with a single gentamicin injection. The remaining 7 subjects ("multiple-treatment group"; 39%) experienced recurrent vertigo that required a second injection of gentamicin at a mean of 6 months after the first treatment. The 11 subjects in the single-treatment group had significantly greater reduction of labyrinthine function after the first treatment, as measured by change in ipsilateral horizontal canal gain, than did the 7 subjects with vertigo recurrence. Changes in caloric asymmetry did not correlate with vertigo control. Conclusions: Our results suggest that successful treatment of Meniere's disease is closely related to attenuation of semicircular canal function as measured by horizontal canal aVOR gains. Key Words: angular vestibulo-ocular reflex gain, intratympanic gentamicin, Meniere's disease. INTRODUCTION 4 days. Nineteen percent of the patients in their series Intratympanic injection of gentamicin is increas- required re-treatment for vertigo control at a mean ingly used to control vertigo that is refractory to medi- «f ^ months after the initial treatment. Harner et aP cal treatment in unilateral Meniere's disease. Since g^ve I intratympanic injection of gentamicm and Schuknechti first introduced intratympanic amino- found that 41% of thetr patients required additional glycosides as a treattnent for Meniere's disease in treatments. In all of these recent case series, it is un- 1956, myriad treatment regimens have been pro- '-•"ear why there is recurrence ot vertigo in some pa- posed. These regimens have varied in the drug con- ti^nt^ but not others, or what clinical signs could be ccntration, as well as in the number and frequency "^^d to predict the recurrence ot vertigo, of doses. There does not appear to be a consensus on The goal of our study was to identify the factors which regimen most effectively controls vertigo.- In that correlate witb successful control of vertigo in a titration-based protocol previously used at our insti- patients treated with 1 intratympanic injection of gen- tution.^ patients were given weekly injections of in- tamicin. We used magnetic search coil testing to mea- tratympanic gentamicin until they developed clinical sure the angular vestibulo-ocular reflex (aVOR) elic- signs of vestibuiar hypofunction. Of these patients, ited by rapid rotary head thrusts in the planes of the recurrence of vertigo occurred at 6 months or more semicircular canals in subjects tested before and after after treatment in 22%. Kaplan et aH treated their treatment. These measurements were then compared series of patients with 3 injections of gentamicin over between subjects who, during a 1 -year foUow-up pe- Hrom Ihe Department of Otolaryngology-Head and Neck Surgery. The Johns Hopkins University School of Medicine. Baltimore. Maryland (Lin, Migiiacuio. Minor, Carey), and ihe Deparlmenl of Neurology. University Hospital Zurich (Haslwanter). and the lnstiiule of Theoretical Physics. Hidgenossische Technische Hochschule (Haslwanter). Zurich, Switzerland. Supported by ihe Na- iional Institutes of Health (ROl DC05040, K23 DC00i')6). Presented in part at the Mid-Winter Meeting of the Assuciatitm for Research in Otolaryngology. Si Peiersburg, Florida. January 27- 31.2002. Correspondence: John P. Carey, MD. Dept of Otolaryngology-Head and Neck Surgery, Johns Hopkins OutpatienI Center. Room 6255. 601 N Caroline Si. Baltimore. MD 212S7-0910. 777

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Annals i>f Oiiilogy, Rhinology & Ijiryngology 114( IO(:777-785.© 2(J0fi Annuls Publlshiitg Company. All rights reserved.
Angular Vestibulo-ocular Reflex Gains Correlate With VertigoControl After Intratympanic Gentamicin Treatment for
Meniere's Disease
Frank R. Lin, MD; Americo A. Migliaccio, PhD; Thomas Haslwanter, PhD;Lloyd B. Minor, MD; John P. Carey, MD
Objectives: The objective of our study was to determine whether angular vestibulo-ocular reflex (aVOR) gains correlatedwith vertigo control after intratympanic genlamicin treatment for Meniere's disease.
Methods: We conducted a prospective study of 18 subjects with unilateral Meniere's disease treated with intralympanicgentamicin injection and followed all subjects for I year. We measured the gain of the aVOR elicited by rapid rotaryhead thrusts in each of the canal planes for each subject before and after treatment with intratympanic gentamicin byusing magnetic search coils to record eye movements.
Results: During the follow-up period. II subjects ("single-treatment group": 61%) had eontrol of their vertigo with asingle gentamicin injection. The remaining 7 subjects ("multiple-treatment group"; 39%) experienced recurrent vertigothat required a second injection of gentamicin at a mean of 6 months after the first treatment. The 11 subjects in thesingle-treatment group had significantly greater reduction of labyrinthine function after the first treatment, as measuredby change in ipsilateral horizontal canal gain, than did the 7 subjects with vertigo recurrence. Changes in caloric asymmetrydid not correlate with vertigo control.
Conclusions: Our results suggest that successful treatment of Meniere's disease is closely related to attenuation ofsemicircular canal function as measured by horizontal canal aVOR gains.
Key Words: angular vestibulo-ocular reflex gain, intratympanic gentamicin, Meniere's disease.
INTRODUCTION 4 days. Nineteen percent of the patients in their seriesIntratympanic injection of gentamicin is increas- required re-treatment for vertigo control at a mean
ingly used to control vertigo that is refractory to medi- «f ^ months after the initial treatment. Harner et aPcal treatment in unilateral Meniere's disease. Since g^ve I intratympanic injection of gentamicm andSchuknechti first introduced intratympanic amino- found that 41% of thetr patients required additionalglycosides as a treattnent for Meniere's disease in treatments. In all of these recent case series, it is un-1956, myriad treatment regimens have been pro- '-•"ear why there is recurrence ot vertigo in some pa-posed. These regimens have varied in the drug con- ti^nt^ but not others, or what clinical signs could beccntration, as well as in the number and frequency "^^d to predict the recurrence ot vertigo,of doses. There does not appear to be a consensus on The goal of our study was to identify the factorswhich regimen most effectively controls vertigo.- In that correlate witb successful control of vertigo ina titration-based protocol previously used at our insti- patients treated with 1 intratympanic injection of gen-tution.^ patients were given weekly injections of in- tamicin. We used magnetic search coil testing to mea-tratympanic gentamicin until they developed clinical sure the angular vestibulo-ocular reflex (aVOR) elic-signs of vestibuiar hypofunction. Of these patients, ited by rapid rotary head thrusts in the planes of therecurrence of vertigo occurred at 6 months or more semicircular canals in subjects tested before and afterafter treatment in 22%. Kaplan et aH treated their treatment. These measurements were then comparedseries of patients with 3 injections of gentamicin over between subjects who, during a 1 -year foUow-up pe-
Hrom Ihe Department of Otolaryngology-Head and Neck Surgery. The Johns Hopkins University School of Medicine. Baltimore.Maryland (Lin, Migiiacuio. Minor, Carey), and ihe Deparlmenl of Neurology. University Hospital Zurich (Haslwanter). and thelnstiiule of Theoretical Physics. Hidgenossische Technische Hochschule (Haslwanter). Zurich, Switzerland. Supported by ihe Na-iional Institutes of Health (ROl DC05040, K23 DC00i')6).Presented in part at the Mid-Winter Meeting of the Assuciatitm for Research in Otolaryngology. Si Peiersburg, Florida. January 27-31.2002.Correspondence: John P. Carey, MD. Dept of Otolaryngology-Head and Neck Surgery, Johns Hopkins OutpatienI Center. Room6255. 601 N Caroline Si. Baltimore. MD 212S7-0910.
777
778 Un et al. Angular Vestibulo-ocular Reflex Gain & Vertigo Control
riod, had control of their vertigo ("single-treatmentgroup") and those who required additional injectionsfor recurrent vertigo {"multiple-treatment group"").
The aVOR for any canal can be measured withmagnetic search coil recordings of eye and beadmovements during rapid head thrusts in tbe plane ofthe canal being tested. Normal subjects are able tomaintain visual fixation on an object during rapidhead thrusts and hence have gain values (ratio of eyevelocity to head velocity) close to 1.0.̂ Asymmetriesin the aVOR evoked by high-frequency, higb-accel-eration head movements occur after loss of vestibuiarfunction in one ear. The gain of the aVOR evokedby rapid head movements exciting the canal on theside of the lesion is lower than that evoked by rota-tions exciting the coplanar canal on the intact side.^Patients with surgical unilateral vestibuiar destructionhave markedly reduced gain values (0.2 to 0.3) whenhead thrusts are directed toward any of tbe ipsilateralcanals.^ Carey et al̂ demonstrated that a single intra-tympanic injection of gentamicin in patients with Me-niere"s disease was often sufficient to reduce gainsfor ipsilateral canals to values in the range of 0.35 to0.45. The patients with surgical unilateral vestibuiardestruction in the same study showed aVOR gains ofonly 0.2 to 0.3. These results suggest that a single in-tratympanic injection of gentamicin most likely doesnot cause complete hair cell destruction and that theremaining hair cell function may account for the high-er gains in the gentamicin-treated patients. For thepresent .study, the issue to be resolved was whethergreater reduction of vestibuiar function as measuredby quantitative aVOR gains and by the qualitativeclinical head thrust test would be associated with agreater degree of vertigo control.
METHODS
Eighteen subjects with unilateral Meniere's diseaseas defined by the 1995 criteria of the American Acad-emy of Otolaryngology-Head and Neck Surgery weretreated with intratympanic gentamicin for vertigo thatwas refractory to medical treatment (salt-restricteddiet, diuretics, vestibuiar suppressant, and antiemeticmedications)."^ All subjects gave informed consentfor the aVOR recordings through a protocol approvedby the Institutional Review Board at the Johns Hop-kins University School of Medicine, the institution atwhich treatment and testing were performed. Pretreat-ment and posttreatment gain data for several of thesubjects have previously been included in an earlierpublication.''
Protocol for Gentamicin Treatments. Gentamicinwas administered as we have previously described.̂ ^The mid-posterior aspect of the tympanic membrane
was anesthetized and punctured, and the middle earwas filled witb a buffered gentamicin solution (26.7mg/mL gentamicin, 0.4 mL typically injected). Thepatients remained supine with the head angled slight-ly down and turned to the contralateral side for 30minutes to continually bathe the round window withgentamicin solution. The solution was then aspiratedfrom the external canal.
A single injection of intratympanic gentamicin wasgiven, and the subjects were assessed approximately3 weeks later to determine whether they bad thesymptoms and signs expected from the ablation ofunilateral vestibuiar function. The subjects were alsoinstructed to call or return if they experienced anyvertigo attacks. The treatment was considered com-plete after 1 injection if the subjects through I yearof follow-up had no vertigo attacks or if they hadvertigo that they judged to be far less severe (notrequiring medication or interruption of activities) andfar less frequent (<10%) than their pretreatment at-tacks (single-treatment group, n = 11). Subjects whohad recurrent vertigo attacks that required medicationor disrupted activities were defmed as ;7o? having con-trol of their Meniere's disease. These subjects weretreated with additional injections of gentamicin andwere categorized in the multiple-treatment group (n= 7). The subjects in the multiple-treatment grouphad a second treatment at a mean of 6.0± 2.9 months(mean ± SD) after the first injection. Three subjectsin the multiple-treatment group continued to haverecurrent vertigo after the second injection and re-ceived additional treatments. (The numbers of totalinjections received were 5 injections for subject M2,3 injections for subject M6, and 3 injections for sub-ject M7.)
Audiograms were obtained before and after eachtreatment. Our previous experience with this protocolhas shown that further hearing loss is noted in ap-proximately 17% of patients when they are tested 6months or more after intratympanic gentamicin treat-ment.'" These long-term hearing changes followingintratympanic gentamicin have not differed from thenatural history of hearing loss in patients with Me-niere's disease who have not received intratympanicgentamicin.'-
Caloric Tests. Caloric tests were performed on sub-jects with Meniere's disease with a temperature switchirrigation technique for 30.5°C and 43.5°C.i' Hori-zontal eye movements were recorded with electro-̂oculography. and the maximum velocity of the slow-phase component of nystagmus was analyzed for uni-lateral weakness and directional preponderance asdetermined by conventional formulas.'^ An ice watercaloric test was performed when tbere was no re-
Un et al. Angular Vestibulo-ocular Reflex Gain & Vertigo Control 779
sponse to warm or cold irrigation of the affected ear(100% asymmetry). If nystagmus was noted in re-sponse to the ice water test, the subject was turnedfrom supine to prone to see whether the nystagmusreversed direction as expected on the basis of a con-vective mechanism.'"^'^
Head Thrust Tests and Gain Calculation. Pretreat-ment head thrust tests were performed on all subjectson tbe same day as treatment except for subjects S8and M3 (in whom they were performed 3 and 196days, respectively, before treatment). All posttreat-ment head thrust tests were performed 2 to 11 weeksafter treatment except for that performed on subjectM7, whose test was done 4 months after treatment.There was no significant difference in the mean timefrom treatment to testing between the two groups(single-treatment group, 40 ± 15 days; multiple-treat-ment group, 51 ±36 days; p = .66).
The subject, seated with the head centered in themagnetic field, was instructed to gaze at a light-emit-ting diode located 124 cm directly forward at eyelevel. The examiner stood behind the subject andgrasped the head over the temporoparietal area. Thehead was kept stationary in a comfortable, "upright"position before each head thrust. This position placedReid's stereotactic line (inferior orbital rim to supe-rior external auditory canal) T ± 7° nose-up fromtbe earth-horizontal plane. From this position the ex-aminer rapidly rotated the head by 10° to 20° in 1 of3 planes: the earth-horizontal plane, the plane con-taining the left anterior and right posterior canals, orthe plane containing the right anterior and left pos-terior canals. For horizontal head thrusts, the headwas turned to the left to excite the left horizontalcanal or to the right to excite tbe right horizontal ca-nal. For left anterior-right posterior head thrusts, thehead was turned down and counterclockwise (withrespect to the subject) in the left anterior-right pos-terior plane to excite the left anterior canal or up andclockwise to excite the right posterior canal. For rightanterior-left posterior bead thrusts, the head wasturned down and clockwise to excite the right anteriorcanal or up and counterclockwise to excite the leftposterior canal. Tbe subject knew which plane wouldbe stimulated in each trial, but could not predict thedirection of the rotation. Approximately 10 to 20 headthrusts were performed in each canal plane.
The instrumentation and technique for recordingeye and head movements during these head thrustswith magnetic search coils have been described indetail elsewbere.'^Our protocol for measuring aVORreflexes elicited by manual head thrusts and for cal-culating gains bas also previously been described.^In brief, monocular or binocular eye movements were
recorded in 3 dimensions at 500-Hz sampling rateswith magnetic search coils embedded in scleral con-tact lenses (Skalar, Delft, the Netherlands). Headmovements were recorded with magnetic search coilsattached to a Plexiglas plate coated with hardeneddental impression compound and molded to the sub-ject's dental occlusion. Eye and head positions in 3dimensions were expressed as rotation vectors andused to derive the angular velocities of the eye andhead. For each head thrust, we calculated the aVORgain by dividing the eye velocity by the bead velocity,using the components of these velocities in the planebeing stimulated. The highest gain value that oc-curred in a 30-ms period before peak head velocitywas taken as the gain for a given trial. The reportedresults are mean gain values obtained from multipletrials performed in each canal plane.
Clinical Head Thrust Te.sts. The clinical head thrusttest is a qualitative visual assessment of tbe aVORin the horizontal canals with the same head thruststimulus tbat is used for tbe quantitative aVOR tests.Gross failure of the aVOR is indicated by the appear-ance of a corrective eye movement following the beadmovement. Clinical head thrust tests were performedon all subjects before and after treatment. The exam-iner stood in front of the seated subject and graspedthe subject's head over the temporoparietal area. Thesubject was asked to look at the examiner's nose.The head was tben rapidly rotated by \0° to 20° inthe earth-horizontal plane toward one side. The sub-ject was noted to have a "head thrust sign" if theexaminer observed a corrective eye movement fol-lowing the head movement. Clinical head thrust testswere performed before quantitative testing, so thattbe decision as to whether the subject had a headthrust sign was independent of tbe results of the quan-titative testing.
Data Analysis. For within-subject comparisons ofgain values before and after treatment, /-tests assum-ing unequal variances were used. Gains, gain asym-metries, and caloric asymmetries between the single-and multiple-treatment groups were compared withthe Mann-Wbitney test. The Fisher exact test wasused to determine the significance of a positive clin-ical head thrust test in differentiating subjects in thesingle- and multiple-treatment groups. Data are re-ported as mean + SD.
RESULTS
Eighteen subjects with unilateral Meniere's diseaserefractory to medical tberapy were treated with a sin-gle intratympanic injection of gentamicin and fol-lowed for I year. Eleven subjects (61%; single-treat-ment group) had control of their vertigo with this

780 Lin et al, Angular Vestibulo-ocular Refle.x Gain & Vertigo Control
SUMMARY OF MEAN AVOR GAINS AND CLINIC AL DATA BEFORE AND AFTER INTRATYMPANICGENTAMICIN TREATMENT
Subject
SIS2S3S4S5S6S7S8S9SIOSll
MlM2M3M4M5M6M7
IHC Gain
0.84/0.34I.II/0..'^30.86/0,450,86/0.39ND/0.270,73/0.320,58/0.311.31/0,380.94/0,200.74/0,741,04/0.61
0,90/0.750.88/0.570.84/0.901,00/0,300.76/0.500,59/0.770.82/1.26
I AC Gain
0,78/0,420,89/0,260.89/0,470.99/0.37ND/0.290,70/0.280,34/0,370.80/0,300.96/0,390,63/0,700,85/0.56
0.48/0.360.69/0,570.93/0.831,05/0,440,83/0.530,63/0.610,87/0,66
IPC Gain
0.57/0.420.92/0.2!0.74/0,350,82/0,30ND/0.180.82/0.480,99/0.320.88/0,290.91/0.210,62/0.680,77/0.67
0.65/0.410,65/0.400.89/0,880,74/0,310,72/0.310,77/0.870,57/0.50
ClinicalHTTSign"
-/+-/+-/+-/+-/+-/+-H/-H
-/+-/+-t-/-H
- / - ( -
- / - l -
- / -
—/—
-/+-t-/+
-/+-/-H
% CaloricAsymmetry''
9/025/884/323/9252/100^15/42100/10032/3133/8217/228/11
24/100^17/18I/I6/ND16/4437/ND4/18
No. ofVertigo Attacks^'
12/178/010/070/33/0
20/052/039/052/015/012/0
6/045/4LV211/47/3
21/312/22
AdditionalInjections^
13.5.7, 1112543,57,9
Data before slash are pretreatment; those after slash are postircuimcnt.
aVOR — angular vestibulo-ocular reflex; S — single-treatment group; M — mitltiple-ireatment group: IHC — ipsilaleral horizontal canal;lAC — ipsilateral anterior canal; IPC — ipsilateral posterior canal; HTT — head thrusi test; ND — nut done,
•"Plus sign indicates appearance of relaxation saccade on HTT. suggesting to clinical examiner deficit in horizonial aVOR; minus sign indicatesno refixation saccade, indicating clinically normal horizontal aVOR,
''Unilateral vesiibular weakness calculated by lormula ot Jongkees et al.'''
••Data are 6 monihs pretreatment (hefore slash) and either 6 months posttreatment or until second Ircalnient (after slash).
•"Data are number of months afler initial treatment until subjects received additional Ireatments.
^Subject had no response to ice-water irrigation.
treatment alone at the I-year follow-up. Seven sub-jects (39%; multiple-treatment group) had recurrentvertigo that required a second treatment at an averageof 6.0 ± 2.9 months after the first treatment. Nine ofthe 11 subjects in the single-treatment group had novertigo attacks in this follow-up period. One subjectin the single-treatment group (SI) had a single epi-sode of mild vertigo 3 months after the treatment,but no vertigo thereafter. The other subject (S4) had3 episodes of mild vertigo 4 months after treatment,but no vertigo in the subsequent follow-up period.The number of vertigo attacks during the 6 monthsbefore and the 6 months after treatment is summa-rized in the Table. '-̂ The single-treatment group sub-jects had experienced vertigo, ipsilateral hearing loss,tinnitus, and/or aural fullness for 7.7 ± 7.7 years(range, I to 25 years) before treatment, and the sub-jects in the multiple-treatment group had had symp-toms for 4.7 ± 4.9 years (range, 0.6 to 15 years, p =.32). The subjects in the single-treatment group were51 ± II years old (range, 32 to 71 years), and thesubjects in the multiple-treatment group were 50 ±15 years old (range, 30 to 75 years). The mean pre-treatment gain was not significantly different (p >.10) between the two groups for any ofthe canals.
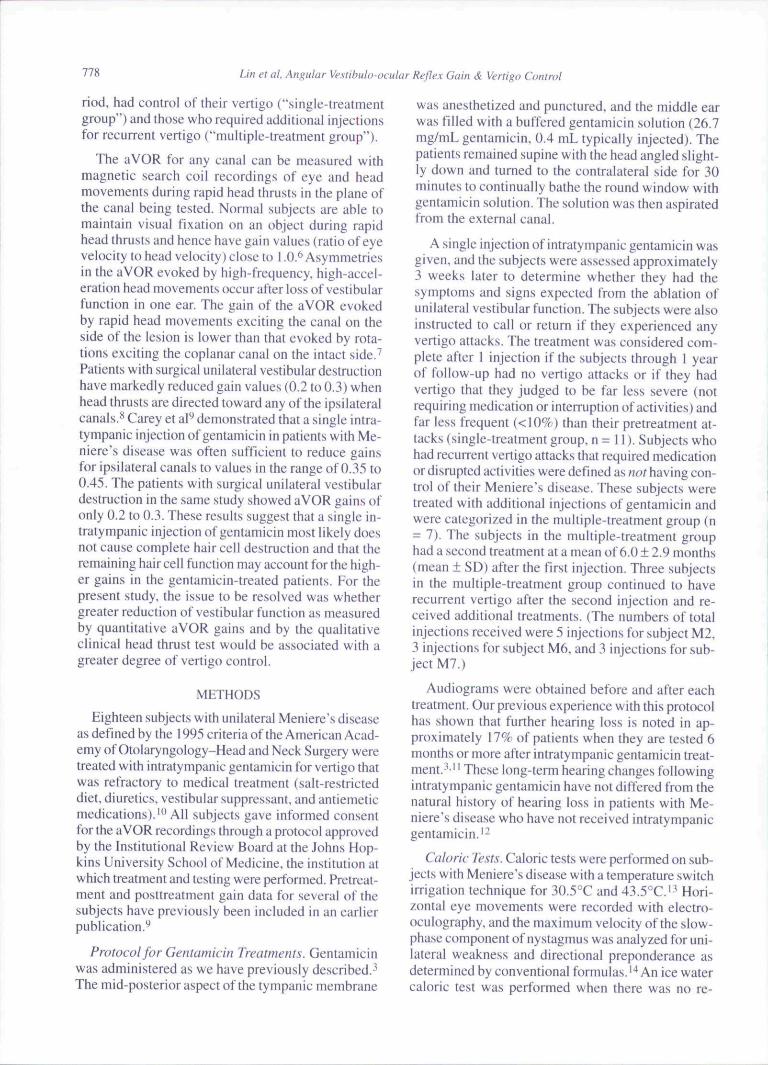
Measurements of a VOR Before and After First In-tratympanic Gentamicin Treatment. Figure I showsthe head and eye velocity traces of a subject in thesingle-treatment group (S11) during rapid rotary headthrusts before and 70 days after treatment. The subjectwas a 49-year-old man with a 15-year history of at-tacks of left fluctuating hearing loss, aural fullness,and vertigo. Just before treatment ofthe left ear witha single intratympanic gentamicin injection, the at-tacks occurred approximately 2 to 3 times per monthdespite medical therapy. After treatment, the subjectdeveloped a positive head thrust sign, and he had novertigo attacks during the I-year follow-up period.
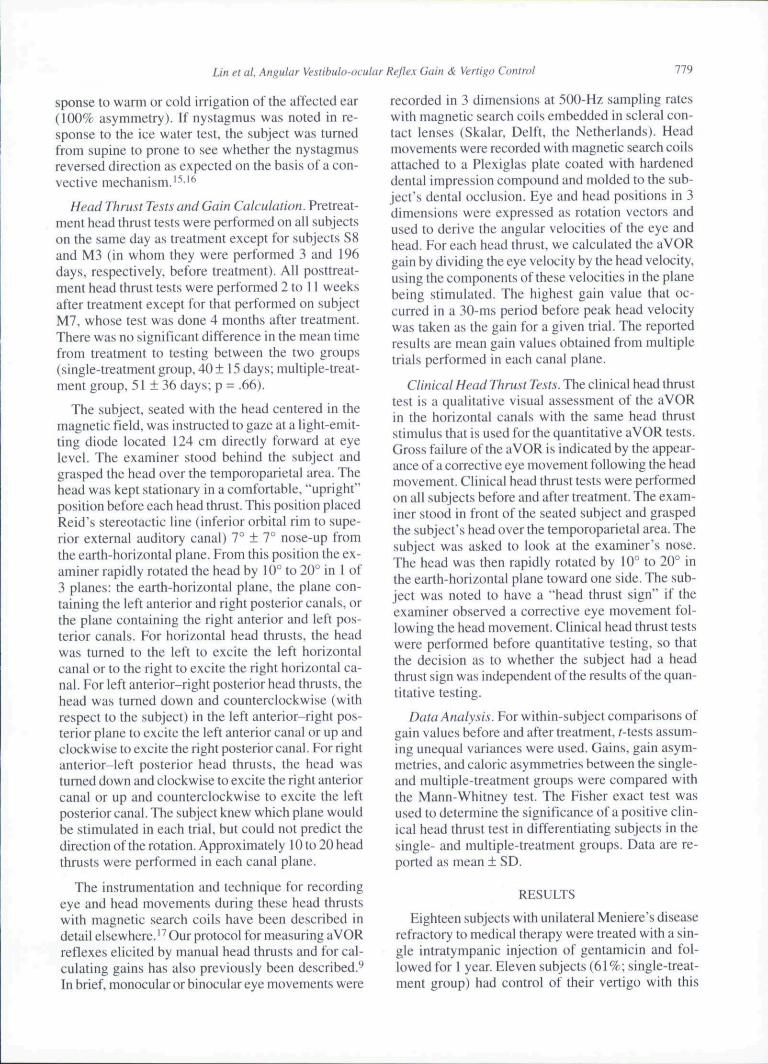
Figure 2 shows the traces for a subject in the mal-tiple-treatment group (M3, a 30-year-old man) beforeand 28 days after the first treatment with intratym-panic gentamicin. Before the first injection of theright ear with intratympanic gentamicin, his attackswere refractory to medical therapy and were charac-terized by right aural fullness, fluctuating hearingloss, and vertigo that would last from 12 to 36 hours.After the first gentamicin treatment, he did not de-velop a head thrust sign. Nine months after treatment,he again began to have attacks of right aural fullness.
Lin et al. Angular Vestibulo-ocular Reflex Gain & Vertigo Control
Ipsilateral
Fig 1. Angular vestibulo-ocular reflex (aVOR)head and eye velocity traces for subject in sin-gle-ireatment group (Sll) before and aftertreatment W\\\\ intratympanic gentamicin. Lightgray lines represent head velocity, dark graylines represent eye velocity, and black segmentsdenote 30 ins before peak bead velocity whengain was calculated. Values in upper rigbt cor-ner of eacb panel represent aVOR gain (mean± SD). HC — borizontal canal. AC — anteriorcanal. PC — posterior canal.
Contra lateral0.8310.08
fluctuating hearing loss, and vertigo lasting severalhours. He described these attacks as being identicalto his previous ones. He had 3 attacks approximately2 weeks apart before being treated with a second in-jection of gentamicin.
Tbe Table displays the mean aVOR gains collectedfrom the 18 subjects before and after treatment withthe first intratympanic injection of gentamicin. After1 treatment, gain for the ipsilateral horizontal canal(IHC) decreased significantly (p < .05) for 9 of 10single-treatment subjects who had both pretreatmentand posttreatment tests available. (The exception wasSIO.) In contrast, only 3 of the 8 multiple-treatmentsubjects (M2. M4. M5) had significant decreases inIHC gain. Significant (p < .05) decreases in gain forthe ipsilateral anterior canal (IAC) were seen aftertreatment for all subjects from both groups exceptfor S7 and SIO, and significant decreases in gain forthe ipsilateral posterior canal (IPC) were also seenin all subjects from both groups except for M3, M6,and SIO.
150 0
Time (ms)
781
HC
Ipsilateral Contralateral
50 100 ISO 0 50 100 150
50 100 150 0 50 100 150
0 50 100 15050 100 150
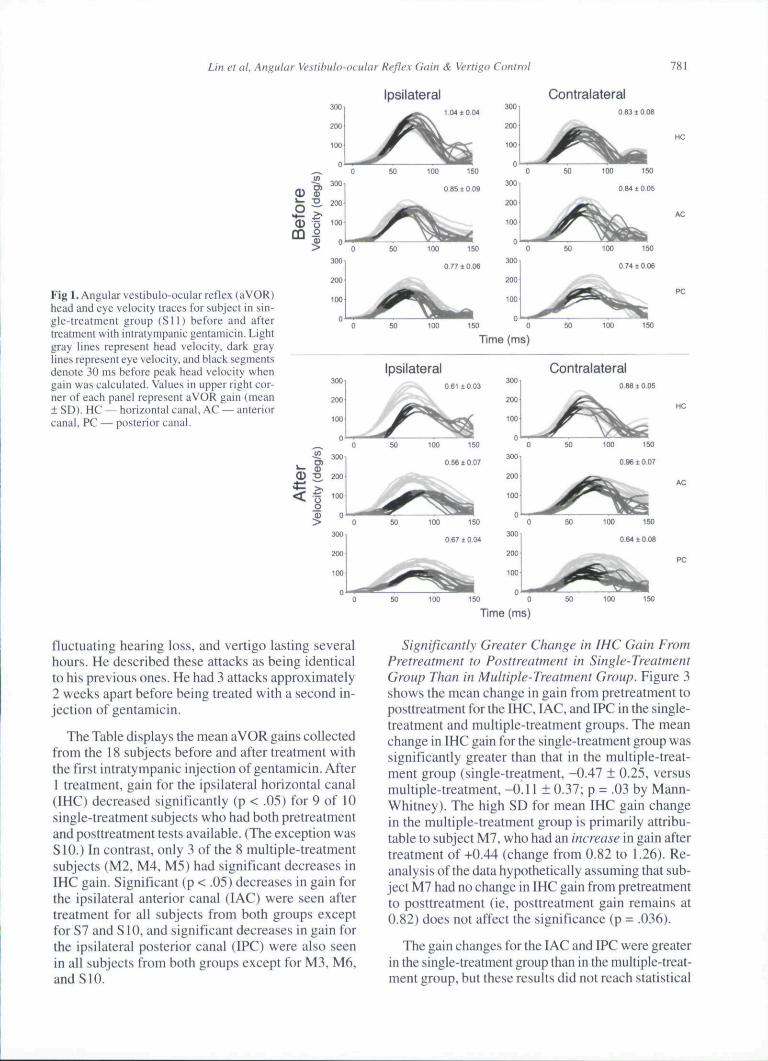
Significantly Greater Change in IHC Gain FromPretreatment to Posttreatment in Single-TreatmentGroup Than in Multiple-Treatment Group. Figure 3shows the mean change in gain from pretreatment toposttreatment for the IHC. IAC, and IPC in the single-treatment and multiple-treatment groups. The meanchange in IHC gain for the single-treatment group wassignificantly greater than that in the multiple-treat-tnent group (single-treatment, -0.47 ± 0.25, versusmultiple-treatment. -0.11 ± 0.37; p = .03 by Mann-Whitney). The high SD for mean IHC gain changein the multiple-treatment group is primarily attribu-table to subject M7, who had an increase in gain aftertreatment of +0.44 (change from 0.82 to 1.26). Re-analysis of the data hypothetically assuming that sub-ject M7 had no change in IHC gain from pretreatmentto posttreatment (ie, posttreatment gain remains at0.82) does not affect the significance (p = .036).
The gain changes for the IAC and IPC were greaterin the single-treatment group than in the multiple-treat-ment group, but these results did not reach statistical

782
300
200
100
0
Lin et al. Angular Vestihiilo-ocular Reflex Gain & Vertigo Control
tpsilateral ContraJateral
50 100 150
0,82 1 0 10
50 100 150 0300
0.89 ± 0 ID
200
100
050 100 150 0 50 100 150
Time (ms)
Ipsilateral Contralateral0.90 ± 0.04 300
200
100
0
PC
Fig 2. aVOR head and eye velocity traces forsubject in multiple-treatment group (M3) be-fore and after treatment with intratyttipanicgentamicin. Light gray lines represent head ve-locity, dark gray lines represent eye velocity,and black segments denote 30 ms before peakhead velocity when gain was calculated. Valuesin upper right corner of each panel representaVOR gain (mean ± SD). HC — horizontal ca-nal. AC — anterior canal, PC — posterior ca-nal.
significance (lAC single versus multiple, -0.37 ±0.25 versus -0.21 ± 0.20. p = . 18; IPC single versusmultiple, -0.41 ± 0.28 versus -0.19 ± 0.20, p = . 11).
Similar results were found when gain asymtnetrydata were compared between the two groups. Themean change in IHC gain asymmetry, but not lACor IPC gain asymmetry, was significantly greater inthe single- than in the multiple-treatment group (datanot shown).
Correlation of Vertigo Recurrence With Failureto Develop Head Thrust Sign After Treatment. Theclinical head thrust tesi is an indicator of diminishedgain in the IHC. A head thrust sign signifies the ex-aminer's observation of a refixating eye movementor "catch-up saccade" after the head is rotationallythrust in the plane of the horizontal canal toward ahypofunctional side.'** Nine of the 11 subjects in thesingle-treatment group and 6 of the 7 subjects in themultiple-treatment group did not have a head thrustsign before treatment. A head thrust sign developedafter treatment in all 9 subjects in the single-treatment
group but in only 4 of the 6 subjects in the multiple-treatment group (see Table). The association betweenfailure to develop a head thrust sign and the need forfuture re-treatment did not reach statistical signifi-cance (Fisher exact test, p = .14).
Mean Change in Caloric A.symmetry Is Not Sig-nificantly Different Between Multiple- and Single-Treatment Groups. Data on pretreatment and post-treattnent caloric asymmetry for the 18 subjects arepresented in the Table. The mean pretreatment caloricasymmetry was not significantly different betweenthe two groups (single-treattnent. 28.9 ± 27.3, versusmultiple-treatment, 15.0 ± 12.7; p = .22). The meanchange in caloric asymmetry from pretreatment toposttreatment was not significantly different betweenthe subjects in the two groups who had botb pretreat-ment and posttreatment caloric data measured (sin-gle-treatment. 25.3 ± 30.0. versus multiple-treatment,23.8 ± 31.3; p = .80). The data from subject S7 werenot used, because the subject had a pretreatment ca-loric asymmetry of 100%.
Lin et al. Angular Vestihiilo-ocuktr Reflex Gain & Veriigo Control 783
Single treatment a Multiple treatments
Fig 3. Mean change in gain, before versus after intratym-panic gentamicin (ITG) treatment, for ipsilateral horizon-tal L-anal (IHC). ipsilateral anterior canal (IAC). and ip.si-lateral posterior canal (IPC). Error bars denote I SD; pvalues denote significance of difference in mean changein gain, before versus after ITG treatment, between multi-ple- and single-treatment groups (Mann-Whitney test).Data from subject S5 were not used in analysis, becausepretreatment data were not available.
DISCUSSION
Tn this study, we investigated whether aVOR gainchanges correlated with vertigo control in subjectswith unilateral Meniere's disease treated with a fixed-dose regimen of 1 intratympanic injection of genta-micin. Our results indicate that control of vertigo inunilateral Meniere's disease is closely associated witha reduction in semicircular canal function as mea-sured by horizontal canal aVOR gain. We tlrst discussthe implications of these findings for our understand-ing of gentamicin's effect on the labyrinth. We thendiscuss the clinical implications of our findings forthe treatment of vertigo in Meniere's disease withintratympanic gentamicin.
Effects of Gentamicin on Labyrinth. Work in ourlaboratory using a chinchilla mode! has recently shedlight on the potential nature of the lesion caused byconservative use of intratympanic gentamicin.''^ Asingle dose of the drug at the concentration used inthe present study was given into the left otic bullaeof chinchillas, and the right ears served as controls.Vestibular nerve afferent physiology and semicircularcanal crista histology were examined after 5 to 25days (early) or 90 to 115 days (late). Afferent record-ings demonstrated that spontaneous afferent firingpersisted at both time periods in the treated ear andthat all classes of discharge regularity were preserved.Nevertheless, the majority of treated afferents didnot measurably respond to tilt or rotation (82% inthe early group and 76% in the late group), and thosethat did respond had vestibular sensitivities that werefractions of those found on the control sides (p <.001). In contrast, sensitivities to galvanic currents.
which may act directly on the vestibular afferents,were unaffected by the treatment. Intratympanic gen-tamicin treatment reduced the histologic density oftype I haircellsby 99%; type II hair cell density wasnot significantly reduced. These findings suggest thatconservative intratympanic gentamicin treatmentcau.ses partial damage and loss of vestibular hair cells(particularly type I hair cells), does not damage theafferent spike initiation zones, and spares enough haircell synaptic activity to drive the spontaneous activ-ity of vestibular afferents.
The results of the present study support the hy-pothesis that successful intratympanic gentamicintreatment reduces vestibular sensory function in thetreated ear. In this study., we quantitatively and quali-tatively assessed vestibular function with aVOR gainand gain asymmetry, caloric asymmetry, and the clin-ical head thrust test. Subjects who had control of theirvertigo after a single intratympanic injection of genta-micin had a greater degree of vestibular hypofunctionas measured by the quantitative head thrust test, andhad a significantly greater change in mean pretreat-ment to posttreattnent IHC gain and gain asymmetrythan did subjects who needed subsequent (multiple)injections.
Our data from the qualitative clinical head thrusttest, although not reaching clinical significance (p =. 14). are consistent with these results. A head thrustsign indicates ipsilateral vestibular hypofunction inthe hori7.ontal canal.'*^ Both subjects (M2 and M3)who started without a head thrust sign before treat-ment and who failed to develop this sign after treat-ment had recurrent vertigo. Although small numbersmay have limited the ability of aqualitative test witha binary outcome (refixation saccade versus no refix-ation saccade) to reach statistical significance, theseresults are consistent with both the quantitative IHCgain data and the physiologic mechanism of the headthrust test.
Another hypothesis for how gentamicin may affectthe labyrinth is the "dark cell hypothesis." which isbased on evidence that aminoglycosides may be di-rectly toxic to dark cells, the principal endolymph-producing cells in the labyrinth. Damage to these cellswould presumably prevent production of excess en-dolymph, limiting hydrops and subsequent vertigo.Pender- '̂' demonstrated dark cell damage in catstreated with daily intratympanic injections of genta-micin. Dark cell damage has also been shown in guin-ea pigs and chicks treated with subcutaneous strep-tomycin.-'"^-^ However, in a more recent study in-volving middle ear instillation of gentamicin or strep-tomycin in chinchillas, scanning electron microscopyrevealed only cochlear and vestibular neuroepithelial
784 Lin et al. Angular Vestihulo-ocular Reflex Gain & Vertigo Control
cell damage and negligible damage to the dark cells.^^
Our results primarily support the hypothesis thatgentamicin exerts its beneficial effect on vertigothrough reduced semicircular canal function. How-ever, the dark cell hypothesis cannot be discountedin all cases. For example, subject S10 had no substan-tial gain changes for the 3 canals, but remained ver-tigo-free at the 1-year follow-up. This finding mayalso simply be due to the recognized high spontane-ous remission rate of Meniere's disease.
Significant increases in IHC canal gains werenoted after gentamicin treatment in subjects M3. M6.and M7. An increase in gain suggests the possibilitythat gentamicin may have had an initial irritative ef-fect on semicircular canal function. Indeed. Parnesand Riddell-'̂ have previously described 3 patientswho developed an irritative (ipsilateral) nystagmusthat persisted for more than a month after intratym-panic gentamicin treatment. Robertson et al̂ *" havealso described possible otolithic irritation after treat-ment with intratympanic gentamicin.
After 1 injection of gentamicin, the single-treat-ment group had a significantly greater pretreatment-to-posttreatment change in IHC gain, but not in IACor IPC gain, than did the multiple-treatment group (Fig3). The significance of the IHC results is not solelyfrom the effect of subject M7. whose increase in IHCgain from pretreatment to posttreatment lessened themean decrease in IHC gain seen in the multiple-treat-ment group relative to the single-treatment group.Reanalysis of the data assuming no change in IHCgain from pretreatment to posttreatment for M7 min-imally affects the significance of the results (p =.036). The lack of significance for the IAC and IPCmay reflect that our technique has less power to detectgain changes in the vertical canals than in the horizon-tal canals. In a previous study.^ we found that it wasmore difficult to thrust the head in the planes of thevertical canals than it is to do so horizontally, andthat peak head thrust velocities were smaller for thevertical canals than for the horizontal canals. Thus,the stimulus for the vertical canals may simply notbe as dynamic as that for the horizontal canals, andsmall changes in vertical canal gain may not be aseasily detected.
Caloric asymmetry was inadequate to predict ver-tigo control in this study. This finding is not surpris-ing, given that there was no consistent correlationbetween caloric and aVOR gain asymmetry data. Be-fore treatment with gentamicin, 8 subjects had abnor-mal (>20%) pretreatment caloric asymmetries, butonly 2 subjects had abnormal IHC gain asymmetries.Based on our data, one possible explanation for thelack of correlation between caloric asymmetry and
aVOR gain asymmetry is that Meniere's disease mayhave a differential impact on vestibular nerve affer-ents in the affected ear such that responses to low-velocity, low-acceleration stimuli (caloric endolymphflow) are reduced more than responses to high-ve-locity, high-acceleration stimuli {head thrusts). There-fore, although the caloric test may be a very sensitiveindicator of subtle loss of function, caloric responsesmay become too impaired before treatment to showsubstantial changes after treatment. Another possibleexplanation for the lack of correlation between caloricand aVOR testing is that responses to rapid headmovements tested with the aVOR may adapt betterto vestibular hypofunction than caloric responses.Rapid angular head movements are encountered ineveryday situations, and therefore the necessary sig-nals are provided for central adaptation. However,for the caloric stimulus, there are no direct physio-logic correlates in terms of head movements. Withoutadequate signals for adaptation, caloric responses be-come rapidly impaired with any reduction in vestib-ular function.
Clinical Implications. Remaining within the thera-peutic window for intratympanic gentamicin to avoidexcess hearing or vestibular loss is made difficult bythe widely varying response to treatment. It is unclearwhy some subjects have a marked decrease in gainafter treatment whereas other subjects have little tono response after the same treatment. Silverstein etaP^ have previously suggested that round windowobstruction may affect the diffusion of medicationinto the perilymph. The round window niche has beenfound to be obstructed by a second "false" membranein up to 20% of human temporal bones.-*^-'' More-over, the thickness of the round window membranemay increase significantly after prior middle ear in-flammation. Hellstrom et al'*'̂ found that the rat roundwindow membrane increased five-fold in thicknessafter purulent otitis media. Despite positioning thepatient with the contralateral ear down for 30 minutesafter the injection, it is unclear how much gentamicinis lost through the eustachian tube or whether an airbubble may block the gentamicin solution's meniscusfrom reaching the round window membrane. Finally,certain subjects may have increased susceptibility tothe vestibulotoxic effects of gentamicin on a geneticbasis, analogous to the increased cochleotoxic sus-ceptibility conferred by identified mitochondrial mu-tations.-""
Previously, there has not been an effective way todetermine when to conclude intratympanic gentami-cin therapy. In our study, caloric data were not ade-quate to predict which patients would have controlof vertigo. The results of this study suggest that quan-titative aVOR measurements may provide an end
Un et al. Angular Vestibulo-ocular Reflex Gain & Vertigo Control 785
point for treatment. Although magnetic search coiltesting is not in widespread use, rapid advances invideo-oculography and other techniques may soonprovide quantitative measurements of the aVORwithout the need for search coils. Although our study
did not have sufficient power to determine the preciseposttreatment aVOR levels needed for vertigo con-trol, larger studies in the future may be able to delin-eate whether a certain level of a VOR function corre-lates with vertigo control.
REFERENCES
1. Schuknechi HF. Ablation therapy for the relief of Me-niere's disease. Laryngoscope i956;66:859-70.
2. Blakley BW. Update on intratympanic gentamiciti for Me-niere's disease. Laryngoscope 2000;l 10:236-40.
3. Minor LB. Intratympanic gentamicin for control of ver-ligo in Meniere's disease: vestibuiar signs that specify comple-tion of therapy. Am J Otol 1999:20:209-19.
4. Kaplan DM. Nedzelski JM. Chen JM. Shipp DB. Intra-tympanit: genlamicin for the treatment of unilateral Meniere'sdisease. Laryngoscope 2000;l 10:1298-305.
5- Harner SG, DriscoU CL. Facer GW. Beatty CW. McDon-ald TJ. Long-term foilow-up of transtynipanic gentamicin forMeniere's syndrome. Otol Neurotol 2001:22:210-4.
6. Aw ST. Haslwanter T. HalmagyiGM,CurthoysIS,YavorRA. Todd MJ. Three-dimensional vector analysis of the humanvesiibuloocular rellex in response to high-acceleration head ro-tations. I. Responses in normal subjects. J Neurophysiol 1996:76:4009-20.
7. Aw ST. Halmagyi GM. HaslwanterT. CurthoysIS, YavorRA. Todd MJ. Three-dimensional vector analysis of the humanvestibuloocular reflex in response to high-acceleration head ro-tations. II. Responses in subjects with unilateral vestibuiar lossand selective semicircular canal occlusion. J Neurophysiol 1996:76:4021-30.
8. Cremer PD, Halmagyi GM. Aw ST. et al. Semicircularcanal plane head impulses delect absent function of individualsemicircular canals. Brain 1998:121:699-716.
9. Carey JP. Minor LB. Peng GC. Delia SantinaCC. CremerPD, Haslwanter T. Changes in the three-dimensional angularvestibulo-ocular reflex following intratympanic gentamicin forMeniere's disease. J Assoc Res Otolaryngol 2002:3:430-43.
10. Committee on Hearing and Equilibrium guidelines for thediagnosis and evaluation of therapy in Meniere's disease. Amer-ican Academy of Otolaryngology-^Head and Neck Foundation,Inc. Otolaryngol Head Neck Surg 1995:113:181-5.
11. Wu IC. Minor LB. Long-term hearing outcome in patientsreceiving intratympanic gentamicin for Meniere's disease. La-ryngoscope 2003:113:815-20.
12. Santos PM. Hall RA. Snyder JM. Hughes LF. Dobie RA.Diuretic and diet effect on Meniere's disease evaluated by the1985 Committee on Hearing and Equilibrium guidelines. Oto-laryngol Head Neck Surg 1993:109:680-9.
13. Proctor L. Dix R. Hughes D. Rentea R. Stimulation ofthe vestibuiar receptor by means of step temperature cbangesduring continuous aural irrigation. Acta Otolaryngol (Stockh)1975;79:425-35.
14. Jongkees LBW. Maas JPM. Pbilipszoon AJ. Clinical nys-tagmography. A detailed study of electro-nystagmography in341 patients with vertigo. Pract Otorhinolaryngol (Basel) 1962;24:65-93.
15. Paige GD. Caloric responses after boHzontal canal inacti-vation. Acta Otolaryngol (Stockb) 1985:100:321-7.
16. Minor LB. Goldberg JM. Influence of static head positionon the horizontal nystagmus evoked by caloric, rotational andoptokinetic stimulalion in tbe squirrel monkey. Exp Brain Res1990:82:1-13.
17. Straumann D. Zee DS. Solomon D. Lasker AG. RobertsDC. Transient torsion during and after saccades. Vision Res1995:35:3321-34.
18. Halmagyi GM, Curtboys IS. A clinical sign of canal pa-resis. Arcb Neurol 1988;45:737-9.
19. Hirvonen TR Minor LB. Hullar TE. Carey JP Effects ofintratympanic gentamicin on vestibuiar afferents and hair cellsin tbe cbinchilla. J Neurophysiol 2005;93:643-55.
20. Pender DJ. Gentamicin tympanoclysis: effects on the ves-tibuiar secrelory cells. Am J Otolaryngol 1985:6:358-67.
21. Park JC, Cohen GM. Vestibuiar ototoxicity in tbe cbick:effects of streptomycin on equilibrium and on ampullary darkcells. Am J Ololaryngol 1982:3:117-27.
22. Park JC. Coben GM. Furtber observations of vestibuiarototoxicity in the chick: effects of streptomycin on tbe ampullarysensory epithelium. Am J Otolaryngol 1984:5:387-93.
23. GeX.SheaJJ. Intramuscular streptomycin effect on darkcells of utricle in guinea pigs. Am J Otol 1993:14:74-8.
24. Chen JM, Kakigi A. Hirakawa H. Mount RJ, HarrisonRV. Middle ear instillation of gentamicin and streptomycin incbincbillas: morpbokjgic appraisal of selective ototoxicity. JOtolaryngo! 1999:28:121-8.
25. Parnes LS, Riddcll D. Irritaiive spontaneous nystagmusfollowing iniraiympanic gentamicin for Meniere's disease. La-ryngoscope 1993:103:745-9.
26. Robertson DD. Garber LZ, Ireland DJ. Ocular torsionmonitoring in cbemical labyrinthectomy. J Otolaryngol 1996;25:171-7.
27. Silverstein H, Rowan PT. Olds MJ, Rosenberg SI. Innerear perfusion and the role of round window patency. Am J Otol1997:18:586-9.
28. Alzamil KS. Linthicum FH Jr. Extraneous round windowmembranes and plugs: possible effect on intratympanic therapy.Ann Otol Rhinol Laryngol 2000:109:30-2.
29. Scbachern PA. Paparella MM. Duvall AJ III. Choo YB.The human round window membrane. An electron microscopicstudy. Arch Otolaryngol 1984; 110:15-21.
30. Hellstrom S. Johansson U, Anniko M. Structure of tberound window membrane. Acta Otolaryngol SuppI (Stockb)1989(suppl457);33-42.
31. Prezanl TR. Agapian JV. Bohlnian MC. et al. Mitochon-drial ribosomai RNA mutation associated with both antibiotic-induced and non-syndromic deafness. Nal Genel 1993;4:289-94.

Related Documents











