Review Adrenal MRI: Techniques and Clinical Applications Evan S. Siegelman, MD * This article is accredited as a journal-based CME activity. If you wish to receive credit for this activity, please refer to the website: www.wileyhealthlearning.com ACCREDITATION AND DESIGNATION STATEMENT Blackwell Futura Media Services designates this journal- based CME activity for a maximum of 1 AMA PRA Category 1 Credit TM . Physicians should only claim credit commensu- rate with the extent of their participation in the activity. Blackwell Futura Media Services is accredited by the Ac- creditation Council for Continuing Medical Education to provide continuing medical education for physicians. EDUCATIONAL OBJECTIVES Upon completion of this educational activity, participants will be better able to review current magnetic resonance imaging techniques and illustrate the MRI features of the commonly encountered lesions of the adrenal gland. ACTIVITY DISCLOSURES No commercial support has been accepted related to the development or publication of this activity. Faculty Disclosures: The following contributors have no conflicts of interest to disclose: Editor-in-Chief: C. Leon Partain, MD, PhD CME Editor: Scott B. Reeder, MD, PhD CME Committee: Scott Nagle, MD, PhD, Pratik Mukher- jee, MD, PhD, Shreyas Vasanawala, MD, PhD, Bonnie Joe, MD, PhD, Tim Leiner, MD, PhD, Sabine Weckbach, MD, Frank Korosec, PhD Author: Evan S. Siegelman, MD This manuscript underwent peer review in line with the standards of editorial integrity and publication ethics maintained by Journal of Magnetic Resonance Imaging. The peer reviewers have no relevant financial relation- ships. The peer review process for Journal of Magnetic Resonance Imaging is double-blinded. As such, the iden- tities of the reviewers are not disclosed in line with the standard accepted practices of medical journal peer review. Conflicts of interest have been identified and resolved in accordance with Blackwell Futura Media Services’s Policy on Activity Disclosure and Conflict of Interest. No relevant financial relationships exist for any individual in control of the content and therefore there were no conflicts to resolve. INSTRUCTIONS ON RECEIVING CREDIT For information on applicability and acceptance of CME credit for this activity, please consult your professional licensing board. This activity is designed to be completed within an hour; physicians should claim only those credits that reflect the time actually spent in the activity. To successfully earn credit, participants must complete the activity during the valid credit period. Follow these steps to earn credit: Log on to www.wileyhealthlearning.com Read the target audience, educational objectives, and activity disclosures. Read the article in print or online format. Reflect on the article. Access the CME Exam, and choose the best answer to each question. Complete the required evaluation component of the activity. This activity will be available for CME credit for twelve months following its publication date. At that time, it will be reviewed and potentially updated and extended for an additional period. Hospital of the University of Pennsylvania, Perelman School of Medicine, University of Pennsylvania, Department of Radiology, Philadelphia, Pennsylvania, USA. *Address reprint requests to: E.S.S., Hospital of the University of Pennsylvania, Perelman School of Medicine, University of Pennsylvania, 1st Floor Silverstein, Department of Radiology, 34th and Spruce St., Philadelphia, PA 19104-4283. E-mail: [email protected] Received September 6, 2011; Accepted January 4, 2012. DOI 10.1002/jmri.23601 View this article online at wileyonlinelibrary.com. JOURNAL OF MAGNETIC RESONANCE IMAGING 36:272–285 (2012) CME V C 2012 Wiley Periodicals, Inc. 272

Adrenal Gland MR
Nov 16, 2015
adrenal gland MR
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
-
Review
Adrenal MRI: Techniques and Clinical Applications
Evan S. Siegelman, MD*
This article is accredited as a journal-based CME activity.If you wish to receive credit for this activity, please refer tothe website: www.wileyhealthlearning.com
ACCREDITATION AND DESIGNATION STATEMENT
Blackwell Futura Media Services designates this journal-based CME activity for a maximum of 1 AMA PRA Category1 CreditTM. Physicians should only claim credit commensu-rate with the extent of their participation in the activity.
Blackwell Futura Media Services is accredited by the Ac-creditation Council for Continuing Medical Education toprovide continuing medical education for physicians.
EDUCATIONAL OBJECTIVES
Upon completion of this educational activity, participantswill be better able to review current magnetic resonanceimaging techniques and illustrate the MRI features of thecommonly encountered lesions of the adrenal gland.
ACTIVITY DISCLOSURES
No commercial support has been accepted related to thedevelopment or publication of this activity.
Faculty Disclosures:
The following contributors have no conflicts of interest todisclose:
Editor-in-Chief: C. Leon Partain, MD, PhD
CME Editor: Scott B. Reeder, MD, PhD
CME Committee: Scott Nagle, MD, PhD, Pratik Mukher-jee, MD, PhD, Shreyas Vasanawala, MD, PhD, Bonnie Joe,MD, PhD, Tim Leiner, MD, PhD, Sabine Weckbach, MD,Frank Korosec, PhD
Author: Evan S. Siegelman, MD
This manuscript underwent peer review in line withthe standards of editorial integrity and publication ethicsmaintained by Journal of Magnetic Resonance Imaging.The peer reviewers have no relevant financial relation-
ships. The peer review process for Journal of MagneticResonance Imaging is double-blinded. As such, the iden-tities of the reviewers are not disclosed in line with thestandard accepted practices of medical journal peerreview.
Conflicts of interest have been identified and resolvedin accordance with Blackwell Futura Media ServicessPolicy on Activity Disclosure and Conflict of Interest. Norelevant financial relationships exist for any individual incontrol of the content and therefore there were no conflictsto resolve.
INSTRUCTIONS ON RECEIVING CREDIT
For information on applicability and acceptance of CMEcredit for this activity, please consult your professionallicensing board.
This activity is designed to be completed within an hour;physicians should claim only those credits that reflect thetime actually spent in the activity. To successfully earncredit, participants must complete the activity during thevalid credit period.
Follow these steps to earn credit:
Log on to www.wileyhealthlearning.com Read the target audience, educational objectives, andactivity disclosures.
Read the article in print or online format. Reflect on the article. Access the CME Exam, and choose the best answer toeach question.
Complete the required evaluation component of theactivity.
This activity will be available for CME credit for twelvemonths following its publication date. At that time, it willbe reviewed and potentially updated and extended for anadditional period.
Hospital of the University of Pennsylvania, Perelman School of Medicine, University of Pennsylvania, Department of Radiology, Philadelphia,Pennsylvania, USA.*Address reprint requests to: E.S.S., Hospital of the University of Pennsylvania, Perelman School of Medicine, University of Pennsylvania, 1stFloor Silverstein, Department of Radiology, 34th and Spruce St., Philadelphia, PA 19104-4283. E-mail: [email protected] September 6, 2011; Accepted January 4, 2012.DOI 10.1002/jmri.23601View this article online at wileyonlinelibrary.com.
JOURNAL OF MAGNETIC RESONANCE IMAGING 36:272285 (2012)
CME
VC 2012 Wiley Periodicals, Inc. 272
-
The article reviews current magnetic resonance imaging(MRI) techniques and illustrates the MRI features of thecommonly encountered lesions of the adrenal gland. MRmay not always be able to characterize an adrenal mass.In these instances, reviewing the patients clinical historyand prior imaging can usually differentiate benign frommalignant lesions, even if you cannot establishing anexact tissue diagnosis. The reader is referred to otherreviews of adrenal imaging that emphasizes the use of CTand imagingmanagement algorithms that are beyond thepurview of this focused review (16).
Key Words: adrenal gland; pheochromocytoma; adrenaladenoma; chemical shift imagingJ. Magn. Reson. Imaging 2012;36:272285.VC 2012 Wiley Periodicals, Inc.
MAGNETIC RESONANCE IMAGING(MRI) TECHNIQUES
In-Phase and Opposed-Phase ChemicalShift Imaging
THE CHEMICAL SHIFT between lipid and water pro-tons is 3.5 ppm. At 1.5 T the chemical shift is 220Hz, which corresponds to once every 4.6 msec. Thus,at 1.5 T the ideal dual echo gradient echo sequencehas echo times of 2.3 and 4.6 msec. On 3 T MR sys-tems the chemical shift of 440 Hz results in a dualecho sequence with optimized echo times of 1.15 and2.3 msec (7). Independent of MR field strength thereare three principles that can be used to optimize thechemical shift sequence for adrenal and abdominalimaging.
1. Both the in-phase and opposed images should beobtained in the same breath-hold (eg, as a dualecho gradient echo sequence). Simultaneousimage acquisition eliminates slice misregistrationbetween the opposed-phase and in-phaseimages.
2. The first echo of the dual echo sequence shouldbe the opposed-phase image. This will ensurethat loss of adrenal gland signal intensity on theopposed-phase image compared with the in-phase image is secondary to the presence of lipidand water protons within the same voxel. If thesecond, longer echo time corresponded to theopposed-phase image, then signal loss could beeither from intracellular lipid or from T2* suscep-tibility effects (8,9).
3. The lowest echo time pair of opposed- and in-phase values should be chosen in order to maxi-mize signal-to-noise and minimize T2* suscepti-bility and T2 effects. Thus, at 3 T a dual echogradient echo sequence with echo times of 1.15and 2.3 msec is preferred to 3.45 and 4.6 msec.
Many practices now use a dual echo gradient echosequence instead of a spin echo or fast spin echosequence when performing T1-weighting imaging ofthe abdomen (10).
Twenty years ago Don Mitchell et al (11) publishedthe seminal article that showed the utility of chemical
shift MRI in the detection and characterization of in-tracellular lipid with adrenal masses (Fig. 1a,b). Otherinvestigators subsequently confirmed the value of thistechnique (1223).
There are three ways one can establish the presenceof lipid within an adrenal mass. The first is to qualita-tively compare both the in-phase and correspondingopposed-phase images side-by-side on a workstationusing identical window settings. If the adrenal masshas lower signal intensity on the opposed-phaseimage, it contains lipid (19). A second more rigorousmethod is to create a subtraction image (Fig. 1c) (theopposed-phase image is subtracted from the in-phaseimage) (24). Subtraction images can be generated bymost MR systems or by any number of secondary ven-dor products. Any signal present on the subtractedimage indicates the presence of lipid and water pro-tons within the same voxel (24). If one wanted to per-form a quantitative measurement of adrenal lesionlipid then the chemical shift index can be calculated(21). The chemical shift index is defined as follows:
Chemical shift index [(Signal intensity of adre-nal mass on in-phase image Signal intensity ofadrenal mass on opposed-phase image)/Signalintensity of adrenal mass on in-phase image] 100.
A chemical shift index of >15%20% detects mostlipid-containing adrenal adenomas with high specific-ity (13,23,25). Rarely, lipid containing adrenal metas-tases can occur are exceptions to this rule. Both he-patocellular carcinoma (26,27) and clear cell renal cellcarcinoma (28) contain intracellular lipid. Patientswith these primary malignancies can develop adrenalmetastases that also contains intracellular lipidand lose signal intensity on chemical shift imaging(Fig. 2) (2931). Fortunately, these patient presenta-tions are rare and the clinical history of malignancy isknown.
Unenhanced computed tomography (CT) scans canalso establish the presence of intracellular lipid withinadrenal lesions. An adrenal mass can be character-ized as an adenoma if the lesion measures
-
gradient echo sequence is ideal for detecting intra-cellular lipid it can also be used to characterize mac-roscopic fat by depicting an etching or India-inkartifact at an interface between intralesional or perile-sional fat and adjacent water containing tissue (40)
(Fig. 3a,b). I suggest that to unequivocally establishthe presence of macroscopic fat within an adrenalmyelolipoma, one should compare an in-phase T1-weighted image with a corresponding fat-suppressedT1-weighted sequence (4143). These techniques have
Figure 1.
274 Siegelman
-
been used in the female pelvis to establish the pres-ence of fat within mature cystic teratomas (43,44).Fat-suppressed gradient echo techniques are pre-ferred over spin echo techniques for two reasons.First, gradient echo techniques can more readily beperformed in a breath-hold. Second, when a fat-sup-pressed gradient echo sequence is performed with anopposed-phase echo time, it shows greater loss of rel-ative signal intensity when compared with a corre-sponding fat-suppressed in-phase gradient echo orspin echo technique (45). CT has similar diagnosticaccuracy in the detection and characterization of mac-roscopic fat compared with MR (Fig. 3d).
T2-Weighted Imaging
Studies performed in the late 1980s showed that bothquantitative and qualitative evaluation of adrenalgland T2 signal intensity had moderate accuracy indifferentiating between adrenal adenomas and meta-static disease. Adenomas tend to have signal intensity
comparable to liver or muscle (Fig. 1f), while adrenalmetastases have T2 signal intensity more similar tospleen (46,47). While these trends in T2 signal inten-sity still hold true today, chemical shift imagingremains the most sensitive and specific MR techniqueto differentiate adenomas from nonadenomas.
Heavily T2-weighted fast spin echo sequences (eg,with echo times >180 msec) are obtained in many ab-dominal imaging protocols. Just as these sequencescan be helpful to characterize nonsolid liver lesionssuch as cysts and hemangiomas, the uncommon ad-renal cyst or pseudocyst can be characterized withheavily T2-weighted sequences (41).
Diffusion-Weighted Imaging
The last decade has seen an greater utilization of dif-fusion-weighted imaging techniques in the abdomen(4850). The current literature suggest that neitherdiffusion-weighted imaging nor evaluation of theapparent diffusion coefficients of adrenal masses are
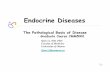
Figure 1. MR and CT illustration of a lipid-rich benign right adrenal adenoma in a 72-year-old man. I clarify below howchemical shift imaging estimated that the adenoma contains 40% lipid. a: In-phase T1 weighted gradient echo image (TR 130 msec, TE 4.8 msec, flip angle 90) shows a 2-cm mass of the right adrenal gland (large arrow). There is mild promi-nence of the lateral limb of the left adrenal gland (small arrow). I have modified the signal intensity values to facilitate the ex-planation of the contrast mechanisms on the subsequent pulse sequences. The signal intensity of the adrenal mass is 100,which is the sum of the water and lipid signal intensities. b: Corresponding opposed-phase T1 weighted image (TE 2.4msec) shows homogeneous moderate loss of signal intensity indicating the presence of intracellular lipid. The resulting signalintensity within the lesion is 20. Based on simple arithmetic, one can then estimate that the adenoma contains 40% lipid.With an optimally timed opposed-phase image and homogenous water and fat protons a resultant signal intensity of 20occurs when 40% of signal that is secondary to lipid will opposecancel a corresponding 40% of water signal, leaving a resid-ual 20%. There is subtle loss of signal intensity within the lateral limb of the left adrenal gland (small arrow). The low signalintensity posterior and lateral to the right adrenal gland represents signal loss secondary to volume averaging of the upperpole of the right kidney with the adjacent perirenal fat. c: Postprocessed subtraction (in-phase/opposed-phase) shows thosevoxels that contain both lipid and water protons as high in signal intensity. Many radiologists find this image helpful in orderto establish the presence of intracellular lipid without having to perform signal intensity measurements on the in- andopposed-phase images. I have found an additional advantage of this sequence is that many radiologists prefer to view highsignal intensity pathology contrasted with a low signal intensity background. In this image the 80% loss of signal intensitybetween the in- and opposed-phase image (100 to 20) of the right adrenal adenoma is depicted as positive signal that meas-ures 80. The highest signal intensity would be expected to be at fat water interfaces where voxels have roughly equivalent sig-nal from lipid and water. The interfaces that exhibited an etching artifact on the opposed-phase image have the highestsignal intensity on this subtraction image. Signal is present with the mesenteric and retroperitoneal fat as these tissues arenot composed of hydrogen protons in a pure lipid environment. Adipocytes have lysosomes and cell membranes that containprotons that behave like water. Thus, it is the intracellular water protons within fat containing tissues that account for themild loss of signal intensity on opposed-phase imaging and resultant positive signal on this subtraction image. d: Corre-sponding water-suppressed image (TE 2.4 msec). Many MR systems have the ability to perform such Dixon techniqueswhere both fat only and water only images are acquired during the same sequence that the dual-echo in- and opposed-phase images are obtained. Such fat only sequences can depict macroscopic fat containing tissues as high signal intensity.This pulse sequence is less sensitive than the opposed-phase sequence and the subtraction image (B,C) for showing high sig-nal intensity within tissues containing less than 50% lipid. In this instance the signal intensity of the right adrenal adenomais 40. I find it easier to characterize adenomas using the dual-echo gradient echo image pair with or without the subtractionimage than relying on a water suppressed image. e: Fat-suppressed T1-weighted image (TE 2.4 msec) shows optimal sup-pression of tissues composed of macroscopic fat. This is the preferred pulse sequence for showing the loss of fat signal withinadrenal myelolipomas (Fig. 3). This sequence is less robust for depicting a change in contrast in those tissues that containless than 50% lipid. For example, the adrenal adenoma has signal intensity of 60 (compared with 100 in the correspondingin-phase image). The opposed-phase image has twice the signal loss because the lipid in the adenoma cancels an equivalentamount of water signal at the echo time of 2.4 msec. On this sequence the fat within the gland is suppressed so it is notavailable to oppose water proton signal intensity, even though it is acquired with an opposed-phase echo time. The normalhigh signal intensity of the liver and pancreas are readily appreciated on this image. They have the same signal intensity asthe in-phase image. However, by suppressing the fat, the dynamic range becomes improved to show the relative difference inT1-signal intensity among the various abdominal organs. f: T2-weighted fast spin echo image (TE 104 msec) shows theright adrenal mass has signal intensity that it hyperintense to liver and paraspinal muscle and hypointense relative to spleen.Absolute or relative T2 signal intensity can not reliably differentiate between adrenal adenomas and nonadenomas. g: Unen-hanced CT shows that the right adrenal mass if of low attenuation. It had measurements of 7 Hounsfield units (HU).
Adrenal MRI Techniques, Clinical Applications 275
-
useful in differentiating adrenal adenomas from meta-static disease (5153).
MR Spectroscopy
There is limited experience with use of MR spectros-copy (MRS) in the characterization of adrenal masses.Studies have shown that MRS can differentiate adeno-mas from nonadenomas because the former has alarger lipid peak (54) with a corresponding greaterlipid/creatine ratio (55). It is unclear whether MRSimproves distinction between adrenal adenomas ver-sus nonadenomas compared with an optimized dualecho gradient echo sequence. One potential nicheapplication of MRS is in the characterization of adre-nal pheochromocytoma. Kim et al (56) have shownthat three patients with surgically proven pheochro-mocytoma had a unique spectral peak at 6.8 ppmthat corresponded with the presence of intralesionalcatecholamines.
Gadolinium-Enhanced Imaging
Multiphase enhanced CT with delayed imaging can of-ten differentiate adrenal adenomas from nonadeno-mas. The details of washout CT kinetics is discussedelsewhere (34,5759). In brief, adenomas tend to losegreater CT attenuation than nonadenomas on imagingperformed between 1 and 15 minutes after iodine con-trast administration. If an unenhanced CT showsattenuation values of less than 10, then enhancedimaging is not required to establish a diagnosis of ad-enoma. However, lipid-poor adenomas that haveunenhanced HU of >10 or do not lose signal intensityon opposed-phase gradient echo images have similarCT washout enhancement patterns as lipid richadenomas (60,61). Thus, an enhanced CT withdelayed imaging could be performed in order to char-acterize a lipid-poor or lipid-absent adrenal mass as abenign adenoma.
There has been little published experience concern-ing the utility of gadolinium-enhanced MRI in thecharacterization of adrenal masses, and what hasbeen published showed conflicting results. One studythat evaluated the MR enhancement features of adre-nal masses found that neither absolute enhancementnor gadolinium washout kinetics were useful in differ-entiating adenomas from nonadenomas (19). However,two studies from over 20 years ago showed promisingresults (62,63). I currently do not rely on the enhance-ment features of an adrenal mass to characterize it asbenign.
PET/MRI
A description of the use of positron emission tomogra-phy (PET) and PET/CT in the evaluation of the adre-nal gland is beyond the purview of this review; thereader is referred to a 2011 meta analysis by Bolandet al (64). As of this writing some of the first integratedPET-MRI systems have become available. It is tooearly to determine whether such hybrid systems willoffer significant advantages in adrenal gland evalua-tion compared with current imaging techniques (65).
MANAGEMENT OF ADRENAL MASSES
The management of an adrenal mass detected by MRIis influenced by the clinical history. The following dis-cussions are based on the two most commonlyencountered clinical settings. The first is the inciden-tal adrenal lesion. This is defined by the AmericanCollege of Radiology and others as an adrenal mass(>1 cm) discovered incidentally on cross-sectionalimaging examination performed for other reasons (6).The second clinical situation is when one detects anadrenal lesion in a patient with a known primarymalignancy.
There have been many reviews on the imaging fea-tures, pathology, and/or management of adrenalincidentalomas by radiologists (5,6,66,67) endocri-nologists/internists (6870) surgeons (71,72), andmultidisciplinary panels (73). The management of thepatient depends on the clinical context in which theadrenal mass is detected.
Patients With No Known Primary Malignancy
If a patient does not have a known malignancy thenan adrenal mass discovered at cross-sectional imag-ing will rarely represent occult metastatic disease. Ina CT study from Rhode Island Hospital not a singleadrenal malignancy was found among 973 consecu-tive non-oncologic patients with 1049 adrenal masses.Even among the 14 patients who developed a subse-quent cancer on follow-up imaging, the initial adrenalmass remained stable (74). In a subpopulation ofthese patients, 321 adrenal lesions with HU of >10were present in 290 patients. None of these lesionsthat could not be characterized as a benign adenomaby CT HU measurement showed growth or wereshown to be malignant at follow-up imaging. Thus,radiologists may be justified in stating that there is lit-tle or no chance of malignancy when encountering anisolated adrenal mass in a patient without cancer.
The consensus is that tissue sampling or surgicalexcision should be performed for an adrenal inciden-taloma that measures >4 cm in order to excludemalignancy (68,69,75). Others suggest excision onlyfor those lesions >6 cm and either surgery or closefollow-up in those masses that measure between 4and 6 cm (73). The reason for having such a lowthreshold for tissue sampling is that the risk of malig-nancy in adrenal incidentalomas >6 cm is 25%(5,72,73,75). As the technique of laparoscopic adre-nalectomy has matured, surgeons have a lowerthreshold for excising suspect adrenal masses (76). Inone center adrenocortical carcinomas measuring upto 10 cm were successfully removed with a laparo-scopic approach (77). Obviously, biopsy or surgerycan be avoided if imaging can characterize the largeradrenal mass as a benign lesion such as myelolio-poma (Fig. 3) or cyst (70).
There is still no clear consensus how often patientswith
- Dr. Cawood et al (78) that such recommendationswould result in potential unnecessary radiation to thepatient along with increased financial and emotionalcosts. The Italian Association of Clinical Endocrinolo-gists (AME) (70) posit that there is insufficient data toprovide confident recommendations of the frequencyof imaging follow-up but do state that there is littleutility in performing imaging following a
-
adenomas, aldosterone-producing adrenal adenomas,and pheochromocytoma.
Pheochromocytoma
Pheochromocytomas are catecholamine-secretingneoplasms. 90% of pheochromocytomas originatewithin the adrenal medulla and 90% of adrenal pheo-chromocytomas are benign (79,80). The classic signsand symptoms of pheochromocytoma are hyperten-sion, along with the triad of episodic headaches,sweating, and palpitations (81,82). One-quarter ofpatients with pheochromocytomas will present with anadrenal incidentaloma and between 1% and 15% of ad-renal incidentalomas will be secondary to pheochromo-cytoma (70,79,80,83,84). The clinical findings of pheo-chromocytoma are nonspecific and sporadic. Manypatients with pheochromocytoma, like President Eisen-hower, are only found to have the tumor at autopsy(81,85). In one autopsy series of 54 patients with pheo-chromocytoma, the diagnosis was unexpected in 75%yet felt to contribute to patient mortality in over half(86). Because pheochromocytoma has been called thegreat masquerader (86) and the great mimic (82)endocrinologists suggest that all patients who are
found to have an adrenal mass should be screenedwith 24-hour urine metanephrines in order to excludethe presence of excess catecholamine production(68,70).
Patients with specific heritable syndromes are athigher risk of developing pheochromocytoma. Thesesyndromes include von Hippel Landau (VHL), type 1neurofibromatosis, multiple endocrine neoplasia type2 (MEN2), and subtypes of the paraganglioma syn-dromes (87). Up to 25% of patients with sporadic phe-ochromocytoma contain germline mutations at genetictesting (88). The genetics and clinical manifestationsof these conditions are beyond the purview of this ar-ticle but are referenced for those with interest (87,89).
As adrenal pheochromocytoma is derived from theadrenal medulla and not the cholesterol-rich adrenalcortex, pheochromocytomas do not lose signal inten-sity on chemical shift imaging and almost all have HUof >10 (20,84,90) (Fig. 4ad). Pheochromocytomasthat contains lipid are rare and reportable (91). Thus,while it may be difficult or impossible for radiologiststo distinguish between hyperfunctioning and nonhy-perfunctioning adrenal adenoma, I think it is reasona-ble to state that a pheochromocytoma can beexcluded with high confidence when an unenhanced
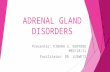
Figure 3. MR illustration on an asymptomatic left adrenal myeloliopoma in a 71-year-old woman. a: In-phase T1-weighted gra-dient echo image (TR 159 msec, TE 4.6 msec) shows a heterogeneous left abdominal mass that has components that aremostly hyperintense relative to liver. b: Corresponding opposed-phase T1 weighted image (TE 2.3 msec) shows internal loss ofsignal intensity (arrows) within some of the intratumoral foci where adipocytes and nonadipocytes are within the same voxel.Etching artifact (double arrows) around an oval component within the anterior portion of the mass indicates a fatwater inter-face. As the surrounding tissue follows the signal intensity of mesenteric and subcutaneous fat, one could conclude that this isalso composed of fat. c: Fat-suppressed T1-weighted gradient echo image obtained as a 3D technique (TR 4.0, TE 1.8 msec,flip angle 10) shows signal loss both within the anterior and posterior portions of the mass. This confirms the presence ofmacroscopic fat. Other pulse sequences confirmed that this mass was originating from the adrenal gland. An exophytic leftupper pole angiomyolipoma or left retroperitoneal well-differentiated liposarcoma could have a similar appearance (123125). d:Corresponding unenhanced CT scan also shows the presence of macroscopic fat within the mass.
278 Siegelman
-
CT or chemical shift MR establishes the presence oflipid within an adrenal lesion.
Other MRI features of pheochromocytomas are highT2 signal intensity relative to skeletal muscle andoccasional T2 signal intensity approaching that of cer-ebral spinal fluid (CSF) (Fig. 4e) (90). One wouldexpect true isointensity to CSF to occur focally withinthe less common cystic pheochromocytoma (92) orthose larger lesions that have cystic necrosis (93). Ondynamic enhanced MR and CT, pheochromocytomastypically hyperenhance compared with adenomas(90,93). CT washout kinetics should not be used toexclude a pheochromocytoma as there can be overlapwith adenomas (94).
Hyperfunctioning Adrenal Cortical Neoplasms
Cortisol-Producing Adrenal Neoplasms
Cortisol-producing adrenal adenoma. Two-thirds ofpatients with Cushing syndrome are secondary to
ACTH producing pituitary adenomas (Cushing dis-ease) (9597). In patients with Cushing disease theadrenal glands typically are enlarged bilaterally andmaintain their adreniform shape. Twenty percent ofcases of Cushing syndrome are secondary to cortisolproduction by the adrenal glands (96). Most of theseadrenal lesions are cortisol-producing adenomas andfewer will be from adrenal cortical carcinoma. In onereview of three case series 12% of adrenal incidentalo-mas were found to be cortisol-producing adenomas(70), while the group from Rhode Island Hospital foundonly one cortisol-producing adenoma among 1049 con-secutive adrenal incidentalomas (74). The size andamount of lipid within an adrenal adenoma does notdifferentiate hyperfunctioning from nonhyperfunction-ing lesions (98). However, a specific imaging feature isrelative atrophy of the remainder of the ipsilateral ad-renal and contralateral adrenal glands (95,99).
The various endocrine tests to evaluate for Cushingsyndrome is beyond the scope of this review but is
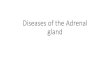
Figure 4. CT and MRI fea-tures of a pheochromocy-toma in a 61-year-oldwoman with hypertension.a: Unenhanced CT examshows a left adrenal massthat measured 20 Houns-field units. Thus the lesioncan not be characterized asan adenoma. bd: In-phase(b), opposed-phase (c), andcorresponding subtractionimage (d) shows a low sig-nal intensity adrenal lesionon in-phase imaging thatdoes not show signal losson opposed-phased imagingand no corresponding sig-nal on the subtractionimage. e: Fat-suppressedrespiratory triggered T2-weighted image shows thatthe adrenal mass has het-erogeneous signal intensityand is hyperintense relativeto spleen. These are sug-gestive but not diagnosticimaging features of pheo-chromocytoma. The patienthad a confirmatory 24-hoururine metanephrine test.
Adrenal MRI Techniques, Clinical Applications 279
-
detailed elsewhere (96). Common signs and symptomsof Cushing syndrome include central obesity, hyper-tension, diabetes, and depression (69). Cushing syn-drome and metabolic syndrome share several clinicalfeatures (100). In one case series, patients with bothmetabolic syndrome and an adrenal incidentalomabenefited from adrenalectomy (101). It is hypothesizedthat these patients had subclinical Cushing syn-drome. One should suggest a diagnosis of subclinicalCushing syndrome in patients with an adrenal ade-noma who have coexistent obesity, hypertension,and hepatic steatosis. The latter is readily depictedon chemical shift imaging and is associated withboth Cushing syndrome and metabolic syndrome(102,103).
Cortisol-producing adrenal cortical carcinoma. Adrenalcortical carcinomas are rare, with an annual inci-dence of 12 per million (104,105). In a series of4027 adrenal cortical carcinomas in 3982 patientsthe median size was 13 cm, with an interquartilerange of 8 to 29 cm (105). In another series of 725 ad-renal cortical carcinomas less than 5% of tumors wereless than 6 cm in size. Adrenal cortical carcinomascan be either hyperfunctioning (60%) or nonhyper-functioning (40%). Nonhyperfunctioning tumors tendto present when they are of a larger size, similar toretroperitoneal sarcomas. Signs and symptoms arerelated to local mass effect. Hyperfunctioning tumorsmay present with signs and symptoms of Cushingsyndrome or virilization due to androgen secretion(106).
The MRI features of adrenal cortical carcinomashave been reported in small series. Cross-sectional
imaging features include large size, ill-define margins,and internal heterogeneity (107). As these carcinomasare derived from the adrenal cortex, chemical shiftMR can reveal intracellular lipid within portions ofthese tumors (Fig. 5) (108,109) The presence of tumorthrombus in the inferior vena cava through spreadfrom the adrenal veins can help to differentiate adre-nal cortical carcinomas from metastatic disease(41,110). Clinically, when one encounters an adrenalmass that has heterogeneous loss of signal intensityon opposed-phase imaging, the most likely diagnosisis a benign adrenal cortical adenoma composed ofboth lipid-rich and lipid-poor adrenal cortical cells(14). However, if the size is >4 cm, the outer marginsare ill defined, or if there is thrombus present in theadjacent adrenal vein, renal vein or IVC, the massshould be considered an adrenal cortical carcinoma
Aldosterone-producing adrenal adenoma
Primary aldosteronism (PA) is a form of secondaryhypertension that is secondary to increased aldoste-rone production independent of the renin-angiotensinaxis (111). In the older literature it was postulatedthat 1% of patients with hypertension may have PA.However, with the implementation of a more sensitivescreening test (plasma aldosterone / plasma renin ac-tivity [PRA] ratio [abbreviated ARR]) and the realiza-tion that only a minority of patients with PA have hy-pokalemia, it is now estimated that up to 12% ofpatients with hypertension may be secondary to PA(111,112).
There are two forms of PA: single aldosterone-pro-ducing adenomas and bilateral adrenal hyperplasia.
Figure 5. MR illustration ofan adrenal cortical carci-noma in an 87-year-oldwoman. a: Coronal fast spinecho T2-weighted imageshows a large left retroperi-toneal mass. bd: In-phase(b), opposed-phase (c), andsubtraction image (d) showsheterogeneous signal inten-sity mass on in-phase imag-ing that shows subtle signalloss on opposed-phasedimaging that is confirmedas positive signal (arrows)on the corresponding sub-traction image. The patienthad pathology-proven meta-static adrenal cortical carci-noma. As this malignancy isderived from the adrenalcortex, it can show thepresence of lipid on chemi-cal shift imaging.
280 Siegelman
-
Patients with a single hypersecreting aldosterone-pro-ducing adenoma benefit from adrenalectomy, whilepatients with bilateral hyperplasia are treated medi-cally. Similar to cortisol-producing adenomas, theMRI features of aldosterone-producing adenomas arenot specific in terms of size or lipid content. Atrophyof the contralateral adrenal gland can suggest thepresence of adenoma hypersecretion. Conversely,thickening of the limbs of the bilateral adrenal glandscan suggest a diagnosis of hyperplasia (113).
As Drs. Cicala and Mantero discuss (111), oneshould not hesitate to perform a laparoscopic adre-nalectomy in a young woman with hypertension, hy-pokalemia, and an abnormal elevated ARR. However,with the prevalence of adenomas on cross-sectioningimaging being as high as 3% in individuals in their5th decade and 10% in their 8th decade (73,83), olderhypertensive patients should have a confirmatory hor-monal test prior to adrenalectomy. One procedurethat radiologists can perform to confirm a hyperfunc-
tioning lesion is adrenal vein sampling; increased se-rum aldosterone should lateralize to the side that hasthe adenoma (114).
In one study of 11 hypertensive patients with primaryaldosteronism and single adenomas, the adrenal veinaldosterone hypersecretion was ipsilateral to the ade-noma in eight, contralateral in two, and symmetricin one. All 10 patients who underwent adrenalectomy(the ipsilateral adrenal in eight and the contralateral ad-renal gland in two) improved clinically (115). In a muchlarger series of 950 patients with primary aldosteronism,15% would have had unnecessary adrenalectomy, 4%would have had the wrong adrenal gland removed, and19% of patients would have been deprived of adrenalec-tomy if the decision to perform or not perform adrenalec-tomy was based on the CT and MR findings without con-firmatory adrenal vein sampling. One review suggestslimiting the use of cross-sectioning imaging to exclude ahyperfunctioning adrenal cortical carcinoma as the etio-logy of the hypertension (111).
Figure 6. MR and CT imaging of growth of an adrenal metastases in a 58-year-old woman with bronchogenic carcinoma. a:Coronal fast spin echo T2-weighted image shows a left apical bronchogenic carcinoma and a heterogeneous left adrenal mass(arrow). b,c: In- and opposed-phase images show no loss of signal intensity within the left adrenal mass. d: Unenhanced CTexamination performed 4 months later shows marked interval growth. The mass had HU of 30.
Adrenal MRI Techniques, Clinical Applications 281
-
Patients With Known Primary Malignancy
In patients with known primary cancers, differentiat-ing between an adrenal adenoma and metastatic dis-ease has implications in terms of treatment, staging,and prognosis. The decision to perform therapeuticadrenalectomy for known metastatic disease is con-troversial. The literature suggests that patients whomay benefit from adrenal metastatectomy should haveisolated metastatic disease to the adrenal gland fromrenal cell or colon primary tumors (116,117). Whenpatients with colorectal cancer have prior resection ofliver metastases, no survival benefit was shown whena subsequent adrenal metatasis was also removed.
When imaging patients with primary malignanciesand metastatic disease to the adrenal gland, addi-tional sites of metastatic disease are often depictedconcurrently (Fig. 2). Metastatic disease to the adrenalgland differs from adenomas in many respects. First,most adrenal adenomas lose signal intensity on chemi-cal shift imaging, where it is only the rare metastaticlipid-containing hepatocellular carcinoma or metastaticclear cell renal cell carcinoma that contains lipid. Sec-ond, metastatic lesions of the adrenal gland grow fasterthan adrenal adenomas (Fig. 6). Most adenomas willstay the same size when followed by imaging and 20%may grow by 12 cm over a 3-year period (70,118).There is less data on the growth rate of adrenal metas-tases in part because patients die before mid- andlong-term follow-up imaging is performed. However, itcan be assumed that most metastatic foci will showsignificant growth at 6 months follow-up, while almostall adenomas will show minimal or no growth (5,119).Third, patients with metastatic disease often have theprimary malignancy (Fig. 6) and other sites of meta-static disease (Fig. 2) depicted on imaging. In a studyfrom MD Anderson of 1639 patients who presentedwith metastatic disease of unknown primary, only four(0.2%) presented with isolated metastatic disease tothe adrenal gland. The metastases were bilateral inthree and each of the four patients had an adrenalmass that was larger than 6 cm. The characterizationof these adrenal lesions should not create a diagnosticdilemma. Finally, size does matter. On average, meta-static adrenal lesions are larger than adenomas. In twostudies that compared the imaging features of 61adenomas with 42 adrenal metastases the latter hadan average size range of 4.55.0 cm, while the formerbenign adenomas had an average size range of 1.92.4cm (53,120). Some oncologic patients may still haveindeterminate adrenal masses that cannot be catego-rized based on current and/or prior imaging. If clinicalmanagement requires adrenal mass categorization, onecould perform an image-guided biopsy to establish thepresence of metastatic disease (121,122).
CONCLUSION
I leave you with three take-home messages concerningMRI of the adrenal gland.
1. If an adrenal lesion losses signal intensity on anopposed-phase image when compared with an
in-phase image, the lesion contains intracellularlipid and is likely an adrenal adenoma. Chemicalshift imaging cannot establish whether an adre-nal mass is hyperfunctioning or not. Radiologistsshould familiarize themselves with the signs,symptoms, and evaluation of hyperfunctioningadrenal lesions so we can eliminate the wordsclinical correlation is suggested from our imag-ing reports.
2. In patients with no known primary malignancy,an incidental adrenal lesion that does notcontain lipid on chemical shift imaging is notoccult metastatic disease. Those adrenal lesionsthat do not lose signal intensity are mostlikely to represent lipid-poor adenomas or apheochromocytoma.
3. Adrenal metastases are not uncommon inpatients with primary malignancies. Intervalgrowth of adrenal metastases, larger size, andfindings of other sites of metastatic disease areoften present. Aggressively searching for anyprior cross-sectional imaging to establish growthis always preferable to suggesting a follow-upimaging exam or tissue sampling in order to es-tablish a diagnosis. The former strategy is cost-effective, minimizes uncertainty for the patient,the patients family and healthcare providers,and should be considered an obligation for thoseof us involved in the performance and interpreta-tion of diagnostic imaging.
REFERENCES
1. Blake MA, Cronin CG, Boland GW. Adrenal imaging. AJR Am JRoentgenol 2010;194:14501460.
2. Boland GW. Adrenal imaging: why, when, what, and how? Part1. Why and when to image? AJR Am J Roentgenol 2010;195:W377381.
3. Boland GW. Adrenal imaging: why, when, what, and how? Part3. The algorithmic approach to definitive characterization of theadrenal incidentaloma. AJR Am J Roentgenol 2011;196:W109111.
4. Boland GW. Adrenal imaging: why, when, what, and how? Part2. What technique? AJR Am J Roentgenol 2011;196:W15.
5. Boland GW, Blake MA, Hahn PF, Mayo-Smith WW. Incidentaladrenal lesions: principles, techniques, and algorithms for imag-ing characterization. Radiology 2008;249:756775.
6. Berland LL, Silverman SG, Gore RM, et al. Managing incidentalfindings on abdominal CT: white paper of the ACR incidentalfindings committee. J Am Coll Radiol 2010;7:754773.
7. Merkle EM, Schindera ST. MR imaging of the adrenal glands:1.5T versus 3T. Magn Reson Imaging Clin N Am 2007;15:365372, vii.
8. Schindera ST, Soher BJ, Delong DM, Dale BM, Merkle EM.Effect of echo time pair selection on quantitative analysis for ad-renal tumor characterization with in-phase and opposed-phaseMR imaging: initial experience. Radiology 2008;248:140147.
9. Tsushima Y, Dean PB. Characterization of adrenal masses withchemical shift MR imaging: how to select echo times. Radiology1995;195:285286.
10. Yamashita Y, Yamamoto H, Namimoto T, Abe Y, Takahashi M.Phased array breath-hold versus non-breath-hold MR imagingof focal liver lesions: a prospective comparative study. J MagnReson Imaging 1997;7:292297.
11. Mitchell DG, Crovello M, Matteucci T, Petersen RO, MiettinenMM. Benign adrenocortical masses: diagnosis with chemicalshift MR imaging. Radiology 1992;185:345351.
12. Bilbey JH, McLoughlin RF, Kurkjian PS, et al. MR imaging ofadrenal masses: value of chemical-shift imaging for
282 Siegelman
-
distinguishing adenomas from other tumors. AJR Am J Roent-genol 1995;164:637642.
13. Fujiyoshi F, Nakajo M, Fukukura Y, Tsuchimochi S. Characteri-zation of adrenal tumors by chemical shift fast low-angle shotMR imaging: comparison of four methods of quantitative evalua-tion. AJR Am J Roentgenol 2003;180:16491657.
14. Gabriel H, Pizzitola V, McComb EN, Wiley E, Miller FH. Adrenallesions with heterogeneous suppression on chemical shift imag-ing: clinical implications. J Magn Reson Imaging 2004;19:308316.
15. Haider MA, Ghai S, Jhaveri K, Lockwood G. Chemical shift MRimaging of hyperattenuating (>10 HU) adrenal masses: does itstill have a role? Radiology 2004;231:711716.
16. Israel GM, Korobkin M, Wang C, Hecht EN, Krinsky GA. Com-parison of unenhanced CT and chemical shift MRI in evaluatinglipid-rich adrenal adenomas. AJR Am J Roentgenol 2004;183:215219.
17. Jhaveri KS, Wong F, Ghai S, Haider MA. Comparison of CT his-togram analysis and chemical shift MRI in the characterizationof indeterminate adrenal nodules. AJR Am J Roentgenol 2006;187:13031308.
18. Korobkin M, Giordano TJ, Brodeur FJ, et al. Adrenal adenomas:relationship between histologic lipid and CT and MR findings.Radiology 1996;200:743747.
19. Korobkin M, Lombardi TJ, Aisen AM, et al. Characterization ofadrenal masses with chemical shift and gadolinium-enhancedMR imaging. Radiology 1995;197:411418.
20. Namimoto T, Yamashita Y, Mitsuzaki K, et al. Adrenal masses:quantification of fat content with double-echo chemical shift in-phase and opposed-phase FLASH MR images for differentiationof adrenal adenomas. Radiology 2001;218:642646.
21. Outwater EK, Siegelman ES, Huang AB, Birnbaum BA. Adrenalmasses: correlation between CT attenuation value and chemicalshift ratio at MR imaging with in-phase and opposed-phasesequences. Radiology 1996;200:749752.
22. Outwater EK, Siegelman ES, Radecki PD, Piccoli CW, MitchellDG. Distinction between benign and malignant adrenal masses:value of T1-weighted chemical-shift MR imaging. AJR Am JRoentgenol 1995;165:579583.
23. Rescinito G, Zandrino F, Cittadini G Jr, Santacroce E, GiasottoV, Neumaier CE. Characterization of adrenal adenomas and me-tastases: correlation between unenhanced computed tomogra-phy and chemical shift magnetic resonance imaging. ActaRadiol 2006;47:7176.
24. Savci G, Yazici Z, Sahin N, Akgoz S, Tuncel E. Value of chemicalshift subtraction MRI in characterization of adrenal masses.AJR Am J Roentgenol 2006;186:130135.
25. Halefoglu AM, Yasar A, Bas N, Ozel A, Erturk SM, Basak M.Comparison of computed tomography histogram analysis andchemical-shift magnetic resonance imaging for adrenal masscharacterization. Acta Radiol 2009;50:10711079.
26. Basaran C, Karcaaltincaba M, Akata D, et al. Fat-containinglesions of the liver: cross-sectional imaging findings withemphasis on MRI. AJR Am J Roentgenol 2005;184:11031110.
27. Martin J, Sentis M, Zidan A, et al. Fatty metamorphosis of hepa-tocellular carcinoma: detection with chemical shift gradient-echo MR imaging. Radiology 1995;195:125130.
28. Outwater EK, Bhatia M, Siegelman ES, Burke MA, Mitchell DG.Lipid in renal clear cell carcinoma: detection on opposed-phasegradient-echo MR images. Radiology 1997;205:103107.
29. Sydow BD, Rosen MA, Siegelman ES. Intracellular lipidwithin metastatic hepatocellular carcinoma of the adrenalgland: a potential diagnostic pitfall of chemical shift imagingof the adrenal gland. AJR Am J Roentgenol 2006;187:W550551.
30. Kreft B, Zhou H, Albers P. [Adrenal gland metastasis of clear-cell renal cell carcinoma: a diagnostic problem in chemical-shiftMRT imaging.] Rofo 2003;175:12751277.
31. Shinozaki K, Yoshimitsu K, Honda H, et al. Metastatic adrenaltumor from clear-cell renal cell carcinoma: a pitfall of chemicalshift MR imaging. Abdom Imaging 2001;26:439442.
32. Ho LM, Paulson EK, Brady MJ, Wong TZ, Schindera ST. Lipid-poor adenomas on unenhanced CT: does histogram analysisincrease sensitivity compared with a mean attenuation thresh-old? AJR Am J Roentgenol 2008;191:234238.
33. Johnson PT, Horton KM, Fishman EK. Adrenal imaging withmultidetector CT: evidence-based protocol optimization and in-terpretative practice. Radiographics 2009;29:13191331.
34. Kamiyama T, Fukukura Y, Yoneyama T, Takumi K, Nakajo M.Distinguishing adrenal adenomas from nonadenomas: combineduse of diagnostic parameters of unenhanced and short 5-minutedynamic enhanced CT protocol. Radiology 2009;250:474481.
35. Perri M, Erba P, Volterrani D, et al. Adrenal masses in patientswith cancer: PET/CT characterization with combined CT histo-gram and standardized uptake value PET analysis. AJR Am JRoentgenol 2011;197:209216.
36. Cyran KM, Kenney PJ, Memel DS, Yacoub I. Adrenal myeloli-poma. AJR Am J Roentgenol 1996;166:395400.
37. Kenney PJ, Wagner BJ, Rao P, Heffess CS. Myelolipoma: CT andpathologic features. Radiology 1998;208:8795.
38. Pereira JM, Sirlin CB, Pinto PS, Casola G. CT and MR imaging ofextrahepatic fatty masses of the abdomen and pelvis: techniques,diagnosis, differential diagnosis, and pitfalls. Radiographics2005;25:6985.
39. Rao P, Kenney PJ,Wagner BJ, Davidson AJ. Imaging and pathologicfeatures of myelolipoma. Radiographics 1997;17:13731385.
40. Hood MN, Ho VB, Smirniotopoulos JG, Szumowski J. Chemicalshift: the artifact and clinical tool revisited. Radiographics 1999;19:357371.
41. Elsayes KM, Mukundan G, Narra VR, et al. Adrenal masses: MRimaging features with pathologic correlation. Radiographics2004;24(Suppl)1:S7386.
42. Krebs TL, Wagner BJ. MR imaging of the adrenal gland:radiologic-pathologic correlation. Radiographics 1998;18:14251440.
43. Bazot M, Boudghene F, Billieres P, Antoine J, Uzan S, Bigot J.Value of fat-suppression gradient-echo MR imaging in the diag-nosis of ovarian cystic teratomas. Clin Imaging 2000;24:146153.
44. Outwater EK, Blasbalg R, Siegelman ES, Vala M. Detection oflipid in abdominal tissues with opposed-phase gradient-echoimages at 1.5 T: techniques and diagnostic importance. Radio-graphics 1998;18:14651480.
45. Siegelman ES, Outwater EK, Vinitski S, Mitchell DG. Fat sup-pression by saturation/opposed-phase hybrid technique: spinecho versus gradient echo imaging. Magn Reson Imaging 1995;13:545548.
46. Baker ME, Blinder R, Spritzer C, Leight GS, Herfkens RJ, Dun-nick NR. MR evaluation of adrenal masses at 1.5 T. AJR Am JRoentgenol 1989;153:307312.
47. Kier R, McCarthy S. MR characterization of adrenal masses:field strength and pulse sequence considerations. Radiology1989;171:671674.
48. Bittencourt LK, Matos C, Coutinho AC Jr. Diffusion-weightedmagnetic resonance imaging in the upper abdomen: technicalissues and clinical applications. Magn Reson Imaging Clin N Am2011;19:111131.
49. Qayyum A. Diffusion-weighted imaging in the abdomen and pel-vis: concepts and applications. Radiographics 2009;29:17971810.
50. Koh DM, Collins DJ. Diffusion-weighted MRI in the body: appli-cations and challenges in oncology. AJR Am J Roentgenol 2007;188:16221635.
51. Miller FH, Wang Y, McCarthy RJ, et al. Utility of diffusion-weighted MRI in characterization of adrenal lesions. AJR Am JRoentgenol 2010;194:W179185.
52. Tsushima Y, Takahashi-Taketomi A, Endo K. Diagnostic utilityof diffusion-weighted MR imaging and apparent diffusion coeffi-cient value for the diagnosis of adrenal tumors. J Magn ResonImaging 2009;29:112117.
53. Sandrasegaran K, Patel AA, Ramaswamy R, et al. Characteriza-tion of adrenal masses with diffusion-weighted imaging. AJRAm J Roentgenol 2011;197:132138.
54. Leroy-Willig A, Roucayrol JC, Luton JP, Courtieu J, NiesenbaumN, Louvel A. In vitro adrenal cortex lesions characterization byNMR spectroscopy. Magn Reson Imaging 1987;5:339344.
55. Faria JF, Goldman SM, Szejnfeld J, et al. Adrenal masses: char-acterization with in vivo proton MR spectroscopyinitial experi-ence. Radiology 2007;245:788797.
56. Kim S, Salibi N, Hardie AD, et al. Characterization of adrenalpheochromocytoma using respiratory-triggered proton MR
Adrenal MRI Techniques, Clinical Applications 283
-
spectroscopy: initial experience. AJR Am J Roentgenol 2009;192:450454.
57. Sangwaiya MJ, Boland GW, Cronin CG, Blake MA, Halpern EF,Hahn PF. Incidental adrenal lesions: accuracy of characteriza-tion with contrast-enhanced washout multidetector CT10-mi-nute delayed imaging protocol revisited in a large patientcohort. Radiology 2010;256:504510.
58. Caoili EM, Korobkin M, Francis IR, et al. Adrenal masses: char-acterization with combined unenhanced and delayed enhancedCT. Radiology 2002;222:629633.
59. Foti G, Faccioli N, Manfredi R, Mantovani W, Mucelli RP. Evalu-ation of relative wash-in ratio of adrenal lesions at early bipha-sic CT. AJR Am J Roentgenol 2010;194:14841491.
60. Pena CS, Boland GW, Hahn PF, Lee MJ, Mueller PR. Characteri-zation of indeterminate (lipid-poor) adrenal masses: use ofwashout characteristics at contrast-enhanced CT. Radiology2000;217:798802.
61. Park BK, Kim CK, Kim B, Lee JH. Comparison of delayedenhanced CT and chemical shift MR for evaluating hyperattenu-ating incidental adrenal masses. Radiology 2007;243:760765.
62. Krestin GP, Freidmann G, Fishbach R, Neufang KF, Allolio B.Evaluation of adrenal masses in oncologic patients: dynamiccontrast-enhanced MR vs CT. J Comput Assist Tomogr 1991;15:104110.
63. Krestin GP, Steinbrich W, Friedmann G. Adrenal masses: evalu-ation with fast gradient-echo MR imaging and Gd-DTPA-enhanced dynamic studies. Radiology 1989;171:675680.
64. Boland GW, Dwamena BA, Jagtiani Sangwaiya M, et al. Charac-terization of adrenal masses by using FDG PET: a systematicreview and meta-analysis of diagnostic test performance. Radi-ology 2011;259:117126.
65. Wehrl HF, Sauter AW, Judenhofer MS, Pichler BJ. CombinedPET/MR imagingtechnology and applications. Technol CancerRes Treat 2010;9:520.
66. Dunnick NR, Korobkin M. Imaging of adrenal incidentalomas:current status. AJR Am J Roentgenol 2002;179:559568.
67. Siegelman ES. MR imaging of the adrenal neoplasms. MagnReson Imaging Clin N Am 2000;8:769786.
68. Terzolo M, Bovio S, Pia A, Reimondo G, Angeli A. Managementof adrenal incidentaloma. Best Pract Res Clin Endocrinol Metab2009;23:233243.
69. Young WF Jr. Clinical practice. The incidentally discovered adre-nal mass. N Engl J Med 2007;356:601610.
70. Terzolo M, Stigliano A, Chiodini I, et al. AME position statementon adrenal incidentaloma. Eur J Endocrinol 2011;164:851870.
71. Shen WT, Sturgeon C, Duh QY. From incidentaloma to adreno-cortical carcinoma: the surgical management of adrenal tumors.J Surg Oncol 2005;89:186192.
72. ONeill CJ, Spence A, Logan B, et al. Adrenal incidentalomas:risk of adrenocortical carcinoma and clinical outcomes. J SurgOncol 2010;102:450453.
73. Grumbach MM, Biller BM, Braunstein GD, et al. Management ofthe clinically inapparent adrenal mass (incidentaloma). AnnIntern Med 2003;138:424429.
74. Song JH, Chaudhry FS, Mayo-Smith WW. The incidental adre-nal mass on CT: prevalence of adrenal disease in 1,049 consec-utive adrenal masses in patients with no known malignancy.AJR Am J Roentgenol 2008;190:11631168.
75. Mantero F, Terzolo M, Arnaldi G, et al. A survey on adrenal inci-dentaloma in Italy. Study Group on Adrenal Tumors of the Ital-ian Society of Endocrinology. J Clin Endocrinol Metab 2000;85:637644.
76. Mazzaglia PJ, Vezeridis MP. Laparoscopic adrenalectomy: bal-ancing the operative indications with the technical advances. JSurg Oncol 2010;101:739744.
77. Brix D, Allolio B, Fenske W, et al. Laparoscopic versus open ad-renalectomy for adrenocortical carcinoma: surgical and onco-logic outcome in 152 patients. Eur Urol 2010;58:609615.
78. Cawood TJ, Hunt PJ, OShea D, Cole D, Soule S. Recommendedevaluation of adrenal incidentalomas is costly, has high false-positive rates and confers a risk of fatal cancer that is similar tothe risk of the adrenal lesion becoming malignant; time for arethink? Eur J Endocrinol 2009;161:513527.
79. Lenders JW, Eisenhofer G, Mannelli M, Pacak K. Phaeochromo-cytoma. Lancet 2005;366:665675.
80. Plouin PF, Amar L, Lepoutre C. Phaeochromocytomas and func-tional paragangliomas: clinical management. Best Pract ResClin Endocrinol Metab 2010;24:933941.
81. Manger WM. An overview of pheochromocytoma: history, cur-rent concepts, vagaries, and diagnostic challenges. Ann N YAcad Sci 2006;1073:120.
82. Cohen DL, Fraker D, Townsend RR. Lack of symptoms inpatients with histologic evidence of pheochromocytoma: a diag-nostic challenge. Ann N Y Acad Sci 2006;1073:4751.
83. Mansmann G, Lau J, Balk E, Rothberg M, Miyachi Y, BornsteinSR. The clinically inapparent adrenal mass: update in diagnosisand management. Endocr Rev 2004;25:309340.
84. Kasperlik-Zaluska AA, Roslonowska E, Slowinska-Srzednicka J,et al. 1,111 patients with adrenal incidentalomas observed at asingle endocrinological center: incidence of chromaffin tumors.Ann N Y Acad Sci 2006;1073:3846.
85. Messerli FH, Loughlin KR, Messerli AW, Welch WR. The presi-dent and the pheochromocytoma. Am J Cardiol 2007;99:13251329.
86. Sutton MG, Sheps SG, Lie JT. Prevalence of clinically unsus-pected pheochromocytoma. Review of a 50-year autopsy series.Mayo Clin Proc 1981;56:354360.
87. Opocher G, Schiavi F. Genetics of pheochromocytomas and par-agangliomas. Best Pract Res Clin Endocrinol Metab 2010;24:943956.
88. Neumann HP, Bausch B, McWhinney SR, et al. Germ-line muta-tions in nonsyndromic pheochromocytoma. N Engl J Med 2002;346:14591466.
89. Barontini M, Dahia PL. VHL disease. Best Pract Res Clin Endo-crinol Metab 2010;24:401413.
90. Elsayes KM, Menias CO, Siegel CL, Narra VR, Kanaan Y, Hus-sain HK. Magnetic resonance characterization of pheochromocy-tomas in the abdomen and pelvis: imaging findings in 18surgically proven cases. J Comput Assist Tomogr 2010;34:548553.
91. Blake MA, Krishnamoorthy SK, Boland GW, et al. Low-densitypheochromocytoma on CT: a mimicker of adrenal adenoma.AJR Am J Roentgenol 2003;181:16631668.
92. Lee TH, Slywotzky CM, Lavelle MT, Garcia RA. Cystic pheochro-mocytoma. Radiographics 2002;22:935940.
93. Blake MA, Kalra MK, Maher MM, et al. Pheochromocytoma:an imaging chameleon. Radiographics 2004;24(Suppl 1):S8799.
94. Park BK, Kim CK, Kwon GY, Kim JH. Re-evaluation of pheo-chromocytomas on delayed contrast-enhanced CT: washoutenhancement and other imaging features. Eur Radiol 2007;17:28042809.
95. Choyke PL, Doppman JL. Case 18: adrenocorticotropic hormone-dependent Cushing syndrome. Radiology 2000;214:195198.
96. Newell-Price J. Diagnosis/differential diagnosis of Cushingssyndrome: a review of best practice. Best Pract Res Clin Endo-crinol Metab 2009;23(Suppl 1):S514.
97. Orth DN. Cushings syndrome. N Engl J Med 1995;332:791803.98. Ichiyanagi O, Sasagawa I, Izumi T, et al. Relationship between
clear cell/compact cell ratio and computed tomographic attenu-ation number in adrenocortical adenoma. Int Urol Nephrol1999;31:585590.
99. Choyke PL. Commentary on Computed tomography in the diag-nosis of adrenal disease and Nonfunctioning adrenal masses:incidental discovery on computed tomography. AJR Am JRoentgenol 2009;192:568570.
100. Krikorian A, Khan M. Is metabolic syndrome a mild form of Cush-ings syndrome? Rev Endocr Metab Disord 2010;11:141145.
101. Chiodini I, Morelli V, Salcuni AS, et al. Beneficial metaboliceffects of prompt surgical treatment in patients with an adrenalincidentaloma causing biochemical hypercortisolism. J ClinEndocrinol Metab 2010;95:27362745.
102. Law K, Brunt EM. Nonalcoholic fatty liver disease. Clin Liver Dis2010;14:591604.
103. Rockall AG, Sohaib SA, Evans D, et al. Hepatic steatosis inCushings syndrome: a radiological assessment using computedtomography. Eur J Endocrinol 2003;149:543548.
104. Kebebew E, Reiff E, Duh QY, Clark OH, McMillan A. Extent ofdisease at presentation and outcome for adrenocortical carci-noma: have we made progress? World J Surg 2006;30:872878.
284 Siegelman
-
105. Bilimoria KY, Shen WT, Elaraj D, et al. Adrenocortical carci-noma in the United States: treatment utilization and prognosticfactors. Cancer 2008;113:31303136.
106. Fassnacht M, Allolio B. Clinical management of adrenocortical car-cinoma. Best Pract Res Clin Endocrinol Metab 2009;23:273289.
107. Bharwani N, Rockall AG, Sahdev A, et al. Adrenocortical carci-noma: the range of appearances on CT and MRI. AJR Am JRoentgenol 2011;196:W706714.
108. Schlund JF, Kenney PJ, Brown ED, Ascher SM, Brown JJ,Semelka RC. Adrenocortical carcinoma: MR imaging appearancewith current techniques. J Magn Reson Imaging 1995;5:171174.
109. Mackay B, el-Naggar A, Ordonez NG. Ultrastructure of adrenalcortical carcinoma. Ultrastruct Pathol 1994;18:181190.
110. Chiche L, Dousset B, Kieffer E, Chapuis Y. Adrenocortical carci-noma extending into the inferior vena cava: presentation of a15-patient series and review of the literature. Surgery 2006;139:1527.
111. Cicala MV, Mantero F. Primary aldosteronism: what consensusfor the diagnosis. Best Pract Res Clin Endocrinol Metab 2010;24:915921.
112. Mulatero P, Stowasser M, Loh KC, et al. Increased diagnosis ofprimary aldosteronism, including surgically correctable forms,in centers from five continents. J Clin Endocrinol Metab 2004;89:10451050.
113. Lingam RK, Sohaib SA, Vlahos I, et al. CT of primary hyperal-dosteronism (Conns syndrome): the value of measuring the ad-renal gland. AJR Am J Roentgenol 2003;181:843849.
114. Kahn SL, Angle JF. Adrenal vein sampling. Tech Vasc IntervRadiol 2010;13:110125.
115. Schwab CW, 2nd, Vingan H, Fabrizio MD. Usefulness of adrenalvein sampling in the evaluation of aldosteronism. J Endourol2008;22:12471250.
116. Muth A, Persson F, Jansson S, Johanson V, Ahlman H, Wang-berg B. Prognostic factors for survival after surgery for adrenalmetastasis. Eur J Surg Oncol 2010;36:699704.
117. Mourra N, Hoeffel C, Duvillard P, Guettier C, Flejou JF, Tiret E.Adrenalectomy for clinically isolated metastasis from colorectalcarcinoma: report of eight cases. Dis Colon Rectum 2008;51:18461849.
118. Barzon L, Sonino N, Fallo F, Palu G, Boscaro M. Prevalence andnatural history of adrenal incidentalomas. Eur J Endocrinol2003;149:273285.
119. Pantalone KM, Gopan T, Remer EM, et al. Change in adrenalmass size as a predictor of a malignant tumor. Endocr Pract2010;16:577587.
120. Gufler H, Eichner G, Grossmann A, et al. Differentiation of adre-nal adenomas from metastases with unenhanced computed to-mography. J Comput Assist Tomogr 2004;28:818822.
121. Paulsen SD, Nghiem HV, Korobkin M, Caoili EM, Higgins EJ.Changing role of imaging-guided percutaneous biopsy of adrenalmasses: evaluation of 50 adrenal biopsies. AJR Am J Roent-genol 2004;182:10331037.
122. Mazzaglia PJ, Monchik JM. Limited value of adrenal biopsy inthe evaluation of adrenal neoplasm: a decade of experience.Arch Surg 2009;144:465470.
123. Craig WD, Fanburg-Smith JC, Henry LR, Guerrero R, BartonJH. Fat-containing lesions of the retroperitoneum: radiologic-pathologic correlation. Radiographics 2009;29:261290.
124. Ellingson JJ, Coakley FV, Joe BN, Qayyum A, Westphalen AC,Yeh BM. Computed tomographic distinction of perirenal liposar-coma from exophytic angiomyolipoma: a feature analysis study.J Comput Assist Tomogr 2008;32:548552.
125. Israel GM, Bosniak MA, Slywotzky CM, Rosen RJ. CT differen-tiation of large exophytic renal angiomyolipomas and perirenalliposarcomas. AJR Am J Roentgenol 2002;179:769773.
Adrenal MRI Techniques, Clinical Applications 285
Related Documents