CHAPTER 6 Patient, Subordinate, and Professional Advocacy To see what is right, and not do it, is want of courage, or of principle. —Confucius 124

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
C H A P T E R
6
Patient, Subordinate, andProfessional Advocacy
To see what is right, and not do it, is want of
courage, or of principle.
—Confucius
124

Advocacy—helping others to grow and fulfill their potential—is a critically importantleadership role. Many of the leadership skills that are described in this book, such asrisk taking, vision, self-confidence, ability to articulate needs, and assertiveness, areused in the advocacy role. Management skills are also needed to be an effectiveadvocate.
Nurse leader–managers often find themselves in the role of advocate for theirpatients, subordinates, and the profession. The actions of an advocate are to informothers of their rights and to ascertain that they have sufficient information onwhich to base their decisions. The term advocacy actually comes from the Latinword advocatus, which means “one summoned to give evidence’’ (Blais, Hayes,Kozier, Erb, 2002, p. 61). The goals then of the advocate are to inform, enhanceautonomy, and respect the decisions of others.
Advocacy, in fact, has been recognized as one of the most vital and basic roles ofthe nursing profession since the time of Florence Nightingale. The role, however, iscomplex. Nurses may act as advocates by helping others make informed decisions,by acting as an intermediary in the environment, or by directly intervening on thebehalf of others (Blais et al., 2002).
This chapter will examine the processes through which advocacy is learned aswell as the ways in which leader–managers can advocate for their patients, subordi-nates, and the profession. Specific suggestions for interacting with legislators andthe media to influence health policy are included. Leadership roles and manage-ment functions essential for advocacy are shown in Display 6.1.
BECOMING AN ADVOCATE
Foley, Minick, and Kee (2002) suggest that although advocacy is assumed to be aninherent part of all nursing curricula and is present in all clinical practice settings,the nursing literature contains little description of how nurses learn the advocacyrole. Indeed, in research conducted by Foley et al., participants suggested thatbeing committed to protect and care for others was a core family or communityvalue that reflected who they were as individuals and that it was not deeply rootedin any learning process. Other study participants, however, stated that they learnedadvocating practices by watching how other nurses interacted with patients and bytalking with the nurses about what they did. Still other participants reported thatadvocacy skills were gained as a result of the increased self-confidence they gainedfrom working with mentors who provided a supportive environment for gainingexperience. Regardless of how advocacy is learned, there are nursing values centralto advocacy. These values emphasize caring, autonomy, respect, and empowerment.(See Display 6.2.)
PATIENT ADVOCACY
Standard V, number 3, of the American Nurses Association (ANA) Standards ofProfessional Performance in Clinical Practice (1998) states that the nurse acts as apatient advocate and assists patients in developing skills so that they can advocate
125CHAPTER 6 � Patient, Subordinate, and Professional Advocacy
Nurses may act asadvocates by eitherhelping others makeinformed decisions,by acting as anintermediary in theenvironment, or bydirectly intervening on behalf of others.
126 UNIT 2 � Foundation for Effective Leadership and Management
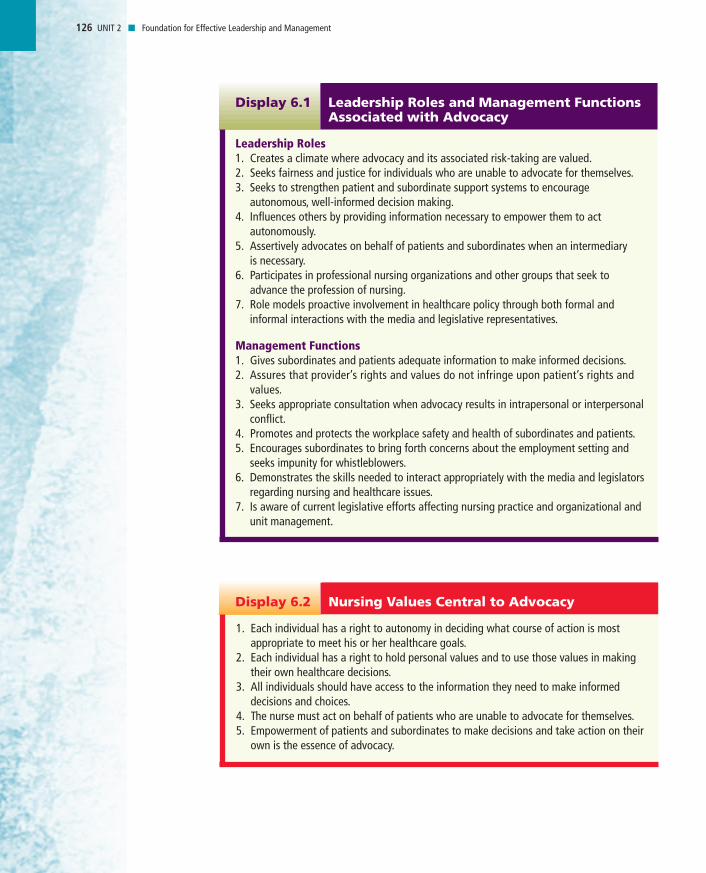
Leadership Roles1. Creates a climate where advocacy and its associated risk-taking are valued.2. Seeks fairness and justice for individuals who are unable to advocate for themselves.3. Seeks to strengthen patient and subordinate support systems to encourage
autonomous, well-informed decision making.4. Influences others by providing information necessary to empower them to act
autonomously.5. Assertively advocates on behalf of patients and subordinates when an intermediary
is necessary.6. Participates in professional nursing organizations and other groups that seek to
advance the profession of nursing.7. Role models proactive involvement in healthcare policy through both formal and
informal interactions with the media and legislative representatives.
Management Functions1. Gives subordinates and patients adequate information to make informed decisions.2. Assures that provider’s rights and values do not infringe upon patient’s rights and
values.3. Seeks appropriate consultation when advocacy results in intrapersonal or interpersonal
conflict.4. Promotes and protects the workplace safety and health of subordinates and patients.5. Encourages subordinates to bring forth concerns about the employment setting and
seeks impunity for whistleblowers.6. Demonstrates the skills needed to interact appropriately with the media and legislators
regarding nursing and healthcare issues.7. Is aware of current legislative efforts affecting nursing practice and organizational and
unit management.
Leadership Roles and Management FunctionsAssociated with Advocacy
Display 6.1
1. Each individual has a right to autonomy in deciding what course of action is mostappropriate to meet his or her healthcare goals.
2. Each individual has a right to hold personal values and to use those values in makingtheir own healthcare decisions.
3. All individuals should have access to the information they need to make informeddecisions and choices.
4. The nurse must act on behalf of patients who are unable to advocate for themselves.5. Empowerment of patients and subordinates to make decisions and take action on their
own is the essence of advocacy.
Nursing Values Central to AdvocacyDisplay 6.2
for themselves. Patient advocacy is necessary because disease almost always resultsin decreased independence, loss of freedom, and interference with the ability tomake choices autonomously. Benner (2003, p. 375) concurs, arguing that being a“good’’ practitioner means more than just examining patient rights; it requiresbeing moved by the patient’s plight and responding to the patient as a person.Thus, advocacy becomes the foundation and essence of nursing, and nurses have aresponsibility to promote human advocacy.
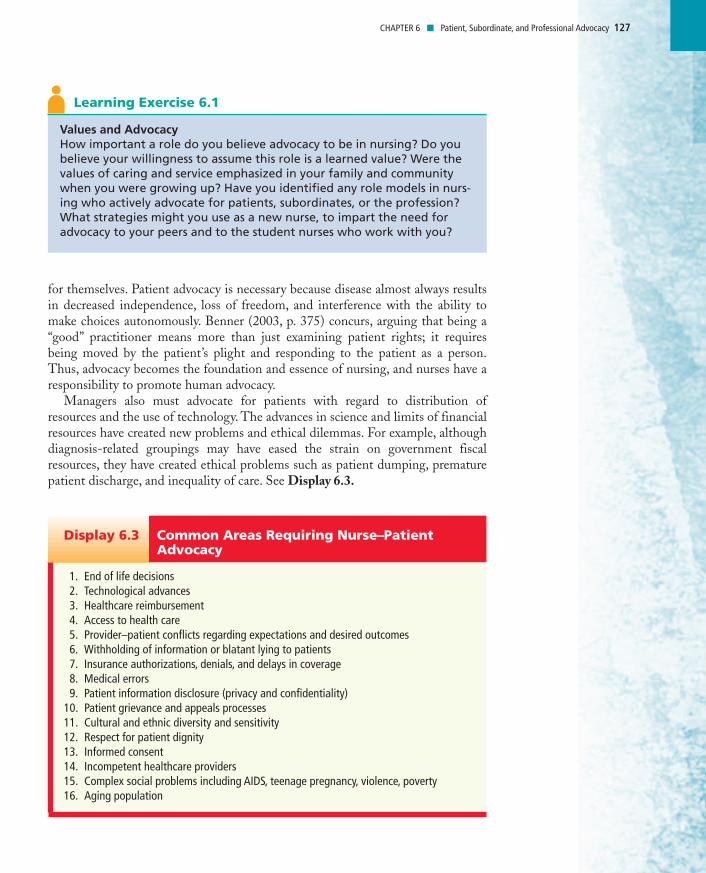
Managers also must advocate for patients with regard to distribution ofresources and the use of technology. The advances in science and limits of financialresources have created new problems and ethical dilemmas. For example, althoughdiagnosis-related groupings may have eased the strain on government fiscalresources, they have created ethical problems such as patient dumping, prematurepatient discharge, and inequality of care. See Display 6.3.
127CHAPTER 6 � Patient, Subordinate, and Professional Advocacy
Values and AdvocacyHow important a role do you believe advocacy to be in nursing? Do youbelieve your willingness to assume this role is a learned value? Were thevalues of caring and service emphasized in your family and communitywhen you were growing up? Have you identified any role models in nurs-ing who actively advocate for patients, subordinates, or the profession?What strategies might you use as a new nurse, to impart the need foradvocacy to your peers and to the student nurses who work with you?
Learning Exercise 6.1
1. End of life decisions2. Technological advances3. Healthcare reimbursement4. Access to health care5. Provider–patient conflicts regarding expectations and desired outcomes6. Withholding of information or blatant lying to patients7. Insurance authorizations, denials, and delays in coverage8. Medical errors9. Patient information disclosure (privacy and confidentiality)
10. Patient grievance and appeals processes11. Cultural and ethnic diversity and sensitivity12. Respect for patient dignity13. Informed consent14. Incompetent healthcare providers15. Complex social problems including AIDS, teenage pregnancy, violence, poverty16. Aging population
Common Areas Requiring Nurse–Patient Advocacy
Display 6.3

First- and middle-level managers are in the best position to advocate forpatients affected by such problems. Benner (2003) states:
Meeting patients and their families and recognizing their concerns abouthealth care comprise the everyday ethical comportment of the practitioner.Patients and families, while encouraged to become empowered and take moreresponsibility for their health, are often vulnerable due to lack of knowledge ofhealth care or due to crisis and reduced capacities. Thus, ethically and legally,healthcare workers are expected to act in the best interests of patients (p. 374).
It is important, however, for the patient advocate to be able to differentiatebetween controlling patient choices (domination and dependence) and in assistingpatient choices (allowing freedom). “When appropriate assessments are conducted,nurses care in ways that offer support, expanding patient possibilities, and engen-dering independence—thus advocacy. In contrast, nurses who impose their valuesand opinions on patients limit patient’s possibilities and create situations of domi-nation and dependence’’ (Foley et al., 2002, p. 185). It is essential that patients haveat least mutual responsibilities in decision making.
128 UNIT 2 � Foundation for Effective Leadership and Management
Considering CultureYou are a staff nurse on a medical unit. One of your patients, Mr. Dau, is a56-year-old Hmong immigrant to the United States. He has lived in thiscountry for four years and became a citizen two years ago. His English ismarginal, although he understands more than he can verbalize. He wasadmitted to the hospital with sepsis resulting from urinary tract infection.His condition is now stable.
Today, Mr. Dau’s physician informed him that his CT scan shows a largetumor in his prostate that is likely cancer. She wants to do immediatefollow-up testing and surgical resection of the tumor to relieve hissymptoms of hesitancy and urinary retention. She tells him that althoughthe tumor is probably cancerous, she believes it will respond well totraditional cancer treatments. Her expectation is that Mr. Dau shouldrecover fully.
One hour later, when you go in to check on Mr. Dau, you find himsitting on his bed, with his suitcase packed, waiting for a ride home. Heinforms you that he is checking out of the hospital. He states that hebelieves he can make himself better at home with herbs and throughprayers by the Hmong “faith healer.” He concludes by telling you that “ifhe is meant to die, that there is little anyone can do.” When you reaffirmthe hopeful prognosis reported by his physician that morning, Mr. Dausays, “She is just trying to give me false hope. I need to go home andprepare for my death.”Assignment: What should you do? How can you best advocate for thispatient? Is the problem a lack of information? How does culture play arole in the patient’s decision? Can paternalism be justified in this case?
Learning Exercise 6.2
It is important, however,for the patient advocateto be able todifferentiate betweencontrolling patientchoices (domination and dependence) andassisting patient choices(allowing freedom).

129CHAPTER 6 � Patient, Subordinate, and Professional Advocacy
1. The patient has the right to considerate and respectful care.2. The patient has the right to and is encouraged to obtain from physicians and their
direct caregivers relevant, current, and understandable information concerning diag-nosis, treatment, and prognosis.
3. The patient has the right to make decisions about the plan of care prior to and during thecourse of treatment and to refuse a recommended treatment or plan of care to the extentpermitted by law and hospital policy and to be informed of the medical consequences ofthis action. In case of such refusal, the patient is entitled to other appropriate care andservices that the hospital provides or transfer to another hospital. The hospital shouldnotify patients of any policy that might affect patient choice within the institution.
4. The patient has the right to have an advance directive (such as a living will, healthcare proxy, or durable power of attorney for health care) concerning treatment ordesignating a surrogate decision maker with the expectation that the hospital willhonor the intent of that directive to the extent permitted by law and hospital policy.
5. The patient has the right to every consideration of privacy. Case discussion, consultation,examination, and treatment should be conducted so as to protect each patient’s privacy.
6. The patient has the right to expect that all communications and records pertaining tohis/her care will be treated as confidential by the hospital, except in cases such assuspected abuse and public health hazards when reporting is permitted or required bylaw. The patient has the right to expect that the hospital will emphasize the confiden-tiality of this information when it releases it to any other parties entitled to reviewinformation in these records.
7. The patient has the right to review the records pertaining to his/her medical care andto have the information explained or interpreted as necessary, except when restrictedby law.
8. The patient has the right to expect that, within its capacity and policies, a hospital willmake reasonable response to the request of a patient for appropriate and medicallyindicated care and services. The hospital must provide evaluation, service, and/or referralas indicated by the urgency of the case. When medically appropriate and legally permis-sible, or when a patient has so requested, a patient may be transferred to another facili-ty. The institution to which the patient is to be transferred must first have accepted thepatient for transfer. The patient must also have the benefit of complete information andexplanation concerning the need for, risks, benefits, and alternatives to such a transfer.
9. The patient has the right to ask and to be informed of the existence of business rela-tionships among the hospital, educational institutions, other health care providers, orpayers that may influence the patient’s treatment and care.
(display continues on page 130)
A Patient’s Bill of RightsDisplay 6.4
Patient Rights
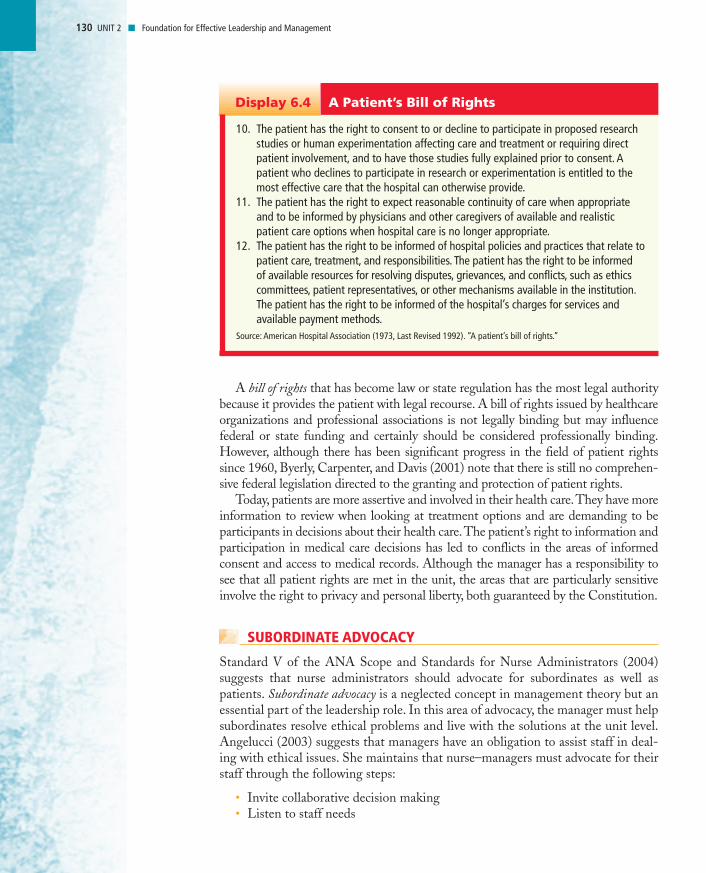
The legislative controls of nursing practice primarily protect the rights of patients.Until the 1960s, patients had few rights; in fact, patients often were denied basichuman rights during a time when they were most vulnerable. In 1973, however, theAmerican Hospital Association published its first Patient Bill of Rights, which wasrevised in 1992 (Display 6.4). Many healthcare organizations and states havepassed a bill of rights for patients since that time.
A bill of rights that has become law or state regulation has the most legal authoritybecause it provides the patient with legal recourse. A bill of rights issued by healthcareorganizations and professional associations is not legally binding but may influencefederal or state funding and certainly should be considered professionally binding.However, although there has been significant progress in the field of patient rightssince 1960, Byerly, Carpenter, and Davis (2001) note that there is still no comprehen-sive federal legislation directed to the granting and protection of patient rights.
Today, patients are more assertive and involved in their health care.They have moreinformation to review when looking at treatment options and are demanding to beparticipants in decisions about their health care.The patient’s right to information andparticipation in medical care decisions has led to conflicts in the areas of informedconsent and access to medical records. Although the manager has a responsibility tosee that all patient rights are met in the unit, the areas that are particularly sensitiveinvolve the right to privacy and personal liberty, both guaranteed by the Constitution.
SUBORDINATE ADVOCACY
Standard V of the ANA Scope and Standards for Nurse Administrators (2004)suggests that nurse administrators should advocate for subordinates as well aspatients. Subordinate advocacy is a neglected concept in management theory but anessential part of the leadership role. In this area of advocacy, the manager must helpsubordinates resolve ethical problems and live with the solutions at the unit level.Angelucci (2003) suggests that managers have an obligation to assist staff in deal-ing with ethical issues. She maintains that nurse–managers must advocate for theirstaff through the following steps:
• Invite collaborative decision making• Listen to staff needs
130 UNIT 2 � Foundation for Effective Leadership and Management
10. The patient has the right to consent to or decline to participate in proposed researchstudies or human experimentation affecting care and treatment or requiring directpatient involvement, and to have those studies fully explained prior to consent. Apatient who declines to participate in research or experimentation is entitled to themost effective care that the hospital can otherwise provide.
11. The patient has the right to expect reasonable continuity of care when appropriateand to be informed by physicians and other caregivers of available and realisticpatient care options when hospital care is no longer appropriate.
12. The patient has the right to be informed of hospital policies and practices that relate topatient care, treatment, and responsibilities. The patient has the right to be informed of available resources for resolving disputes, grievances, and conflicts, such as ethicscommittees, patient representatives, or other mechanisms available in the institution.The patient has the right to be informed of the hospital’s charges for services andavailable payment methods.
Source: American Hospital Association (1973, Last Revised 1992). “A patient’s bill of rights.’’
A Patient’s Bill of RightsDisplay 6.4
• Get to know staff personally• Take time to understand the challenges faced by the staff in delivering care• Face challenges and solve problems together• “Go to bat’’ for staff when needed
Managers must recognize what subordinates are striving for and the goals andvalues subordinates consider appropriate. The leader–manager should be able toguide subordinates toward actualization while defending their right to autonomy.To help nurses deal with ethical dilemmas in their practice, nurse–managers shouldestablish and utilize appropriate support groups, ethics committees, and channelsfor dealing with ethical problems.
Another critical part of subordinate advocacy is workplace advocacy. In workplaceadvocacy, the manager works to see that the work environment is both safe andconducive to professional and personal growth for subordinates. Occupationalhealth and safety must be assured by interventions such as reducing worker expo-sure to needle sticks or blood and body fluids. Subordinates should also be able tohave the expectation that their work hours and schedules will be reasonable, thatstaffing ratios will be adequate to support safe patient care, that wages will be fairand equitable, and that nurses will be allowed participation in organizational deci-sion making. When these working conditions do not exist, managers must advocateto higher levels of the administrative hierarchy to correct the problems.
Top- and middle-level managers can advocate for subordinates in a different way.For example, when the healthcare industry has faced the crisis of inadequate humanresources and nursing shortages, many organizations have made quick, poorly
131CHAPTER 6 � Patient, Subordinate, and Professional Advocacy
How Can You Best Advocate?You are a unit supervisor in a skilled nursing facility. One of your aides,Martha Greenwald, recently reported that she suffered a “back strain”several weeks ago when she was lifting an elderly patient. She did notreport the injury at the time because she did not think it was serious.Indeed, she finished the remainder of her shift and has performed all ofher normal work duties since that time.
Today, Martha reports that she has just left her physician’s office andthat he has advised her to take four to six weeks off from work to fullyrecover from her injury. He has also prescribed physical therapy andelectrical nerve stimulation for chronic pain. Martha is a relatively newemployee, so she has not yet accrued enough sick leave to cover herabsence. She asks you to complete the paperwork for her absence and thecost of her treatments to be covered as a work-related injury.
When you contact the Worker’s Compensation case manager for yourfacility, you learn that the claim will be investigated; however, with nowritten or verbal report of the injury at the time it occurred, that there isgreat likelihood the claim will be rejected.Assignment: How best can you advocate for this subordinate?
Learning Exercise 6.3

thought-out decisions to find short-term solutions to a long-term and severe problem.New workers have been recruited at a phenomenally high cost, yet the problems thatcaused high worker attrition have not been solved. Top- and middle-level managersmust advocate for subordinates in solving problems and making decisions abouthow best to use limited resources. These decisions must be made carefully, followinga thorough examination of the political, social, economic, and ethical costs.
Top- and middle-level managers must also be willing to advocate for whistle-blowers, who speak out about organizational practices they believe may be harmfulor inappropriate. Subordinates want the assurance that if they are acting within thescope of their expertise that they will be able to speak up through appropriate chan-nels without fear of retaliation (Green & Jordan, 2002). While whistle-blower pro-tection has been advocated for at the federal level and has passed in some states,many employees are reluctant to report unsafe conditions for fear of retaliation.Nurses should check with their state association to assess the status of whistleblower protection in their state (Green & Jordan).
PROFESSIONAL ADVOCACY
Managers also must be advocates for the nursing profession. This type of advocacyis described by Quinn and Smith (1987):
Choosing to enter a profession amounts to voluntarily biting off a chunk ofthe human condition. The professional chooses to become involved (withexpertise and commitment) in an area of human life in which important ele-ments of human welfare are at stake and in which people must depend onexperts. In making that choice, the professional becomes committed to livingwith and wrestling with the problem of professional issues and sometimesunavoidable consequences (p. 55).
Joining a profession requires making a very personal decision to involve oneselfin a system of roles that is socially defined. Thus, entry into a profession involves apersonal and public promise to serve others with the special expertise that a profes-sion can provide and that society legitimately expects it to provide.
Professional issues are always ethical issues. When nurses find a discrepancybetween their perceived role and society’s expectations, they have a responsibility toadvocate for the profession. At times, individual nurses believe the problems of theprofession are too big for them to make a difference. A professional commitmentmeans that people cannot shrink from their duty to question and contemplateproblems that face the profession. They cannot afford to become powerless or help-less or claim that one person cannot make a difference. Often, one voice is all ittakes to raise the consciousness of colleagues within a profession.
If nursing is to advance as a profession, practitioners and managers must broad-en their sociopolitical knowledge base to understand better the bureaucracies inwhich they live. This includes speaking out on consumer issues, continuing andexpanding attempts to influence legislation, and increasing membership on govern-mental health policy-making boards and councils. Only then will nurses be able toinfluence the tremendous problems facing society today in terms of the homeless,
132 UNIT 2 � Foundation for Effective Leadership and Management
A professionalcommitment means that people cannotshrink from their duty to question andcontemplate problemsthat face the profession.
Top- and middle-levelmanagers must also bewilling to advocate forwhistle-blowers whospeak out aboutorganizational practicesthey believe may beharmful or inappropriate.

teenage pregnancy, drug and alcohol abuse, inadequate health care for the poor andelderly, and medical errors. These are essential advocacy roles for the profession.
There are many ways for the profession and individual nurses to advocate socialissues. For example, the ANA has advocated for more diversity in nursing (Gonzalez,1999). A leadership role would be one that supports and advocates for diversity with-in an organization. Other issues the ANA and its constituent member associationshave been working to bring attention to include the impact of the current nursingshortage on the quality of care; staffing ratios; and working conditions for nurses,including mandatory overtime. Indeed, in April 2002, the ANA and more than 60partner organizations issued a report entitled Nursing’s Agenda for the Future, whichdetailed the complex factors leading to and exacerbating the current nursing shortage.
Blakeney (2003) suggests that other organizations outside of nursing are alsostepping forward to bring these issues to the attention of the public, media, andpolicy makers. For example, in July 2002, the U.S. Department of Health and HumanServices released a report, Projected Supply, Demand, and Shortages of RegisteredNurses: 2000–2020. In August 2002, the Joint Commission on Accreditation ofHealthcare Organizations released Health Care at the Crossroads: Strategies forAddressing the Evolving Nursing Crisis. In addition, Johnson and Johnson HealthCare Systems, Inc. launched a $20 million campaign in February 2002 to attractmore people to nursing and to increase awareness of the value of the nursing pro-fession in society and America’s health care system (Nursing Shortage, 2002).
133CHAPTER 6 � Patient, Subordinate, and Professional Advocacy
Write It Down. What Would You Change?List five things you would like to change about nursing or the healthcaresystem. Prioritize the changes you have identified. Write a one-page essayabout the change you believe is most needed. Identify the strategies youcould use individually and collectively as a profession to make the changehappen. Be sure you are realistic about the time, energy, and fiscalresources you have to implement your plan.
Learning Exercise 6.4 A
Nursing’s Advocacy Role in Legislation and Public Policy
A distinctive feature of American society is the manner in which citizens can partici-pate in the political process. People have the right to express their opinions aboutissues and candidates by voting. People also have relatively easy access to lawmakersand policy makers and can make their individual needs and wants known. Theoreti-cally, then, any one person can influence those in policy-making positions. In reality,this rarely happens; policy decisions are generally focused on group needs or wants.
Reutter and Williamson (2000) argue that one of the most effective strategiesfor improving the health and welfare of a population is by advocating for its health-care policy. “Nurses at all levels of practice must create and develop strategies topromote and increase the participation of registered nurses in the political processand healthcare policy decision making’’ (Greipp, 2002, p. 35).

The need for organized group efforts by nurses to influence legislative policy haslong been recognized in this country. In fact, the first state associations were organ-ized expressly for unifying nurses to influence the passage of state licensure laws.Political action committees (PACs) of the Congress of Industrial Organizationsattempt to persuade legislators to vote in a particular way. Lobbyists of the PACmay be members of a group interested in a particular law or paid agents of thegroup that wants a specific bill passed or defeated. Nursing must become moreactively involved with PACs to influence healthcare legislation and PACs provideone opportunity for small donors to feel like they are making a difference.
In addition, professional organizations generally espouse standards of care that arehigher than those required by law. Voluntary controls often are forerunners of legalcontrols. Nurses who participate in professional organizations are integral in deter-mining whether voluntary or legal controls represent what nursing is and should be.
Currently, nursing lobbyists in our nation’s capitol are influencing legislation onquality, access to care issues, patient and health worker safety, healthcare restructur-ing, direct reimbursement for advanced practice nurses, and funding for nursingeducation. Representatives of the American Nurse’s Association regularly attendand provide testimony for meetings of the U.S. Department of Health and HumanServices (DHHS), the Department of Health, the National Institutes of Health(NIH), Occupational Safety and Health Administration (OSHA), and the WhiteHouse to be sure that the “nursing perspective’’ is heard in health policy issues(Huston, 1998).
As a whole, the nursing profession has not yet recognized the full potential ofcollective political activity. Nurses must exert their collective influence and maketheir concerns known to policy makers before they can have a major impact onpolitical and legislative outcomes. Because they have been reluctant to becomepolitically involved, nurses have failed to have a strong legislative voice in the past.Legislators and policy makers generally are more willing to deal with nurses as agroup rather than as individuals; thus, joining and supporting professional organi-zations allow nurses to become active in lobbying for a stronger nurse practice actor for the creation or expansion of advanced nursing roles.
In addition to active participation in national nursing organizations, nurses caninfluence legislation and health policy in many ways. Nurses who want to be direct-ly involved can lobby legislators either in person or by letter. This process may seemintimidating to the new nurse; however, many books and workshops are availablethat deal with the subject and a common format is used.
Personal letters are more influential than form letters and the tone should beformal but polite. The letter should also be concise (no more than one page). Besure to address the legislator properly by title. Establish your credibility early in theletter as both a constituent and as a healthcare expert. State your reason for writingthe letter in the first paragraph and refer to the specific bill you are writing about.Then state your position on the issue and give personal examples as necessary tosupport your position. Offer your assistance as a resource person for additionalinformation. Then, sign the letter, including your name and contact information.Remember too to be persistent and to write legislators repeatedly who are undecidedon an issue. Display 6.5 displays a format common to letters written to legislators.
134 UNIT 2 � Foundation for Effective Leadership and Management
Nurses who participatein professionalorganizations areintegral in determiningwhether voluntary orlegal controls representwhat nursing is andshould be.
135CHAPTER 6 � Patient, Subordinate, and Professional Advocacy
March 15, 2005
The Honorable John DoeMember of the SenateState Capitol, Room ____City, State, Zip Code
Dear Senator Doe,I am a registered nurse and member of the American Nurses Association (ANA). I am
also a constituent in your district. I am writing in support of SB XXX, which requires theestablishment of minimum RN staffing ratios in acute care facilities. As a staff nurse on anoncology unit in our local hospital, I see first-hand the problems that occur when staffingis inadequate to meet the complex needs of acutely ill patients: medical errors, patientand nurse dissatisfaction, workplace injuries, and perhaps most importantly, the inabilityto spend adequate time with and comfort patients who are dying.
I have enclosed a copy of a recent study conducted by John Smith and published in theJanuary 2005 edition of Nurses Today. This article details the positive impact of legisla-tive staffing ratio implementation on patient outcomes as measured by medication errors,patient falls, and nosocomial infection rates.
I strongly encourage you to vote for SB XXX when it is heard by the Senate Businessand Professions Committee next week. Thank you for your ongoing concern with nursingand healthcare issues and for your past support of legislation to improve healthcarestaffing. Please feel free to contact me if you have any questions or would like additionalinformationRespectfully,
Nurse Nancy
Nurse Nancy, R.N., B.S.N.Street,City, State, Zip CodePhone number including area codeEmail address
Exemplar: A Letter to Your LegislatorDisplay 6.5
Realistic Advocacy for the Nursing ProfessionDo you belong to your state nursing organization or student nursingorganization? Why or why not? Make a list of six other things you coulddo to advocate for the profession. Be specific. Is your list realistic in termsof your energy and commitment to nursing?
Learning Exercise 6.5A
Other nurses may choose to monitor the progress of legislation, count congres-sional votes, and track specific legislator’s voting intents as well as past votingrecords. Still other nurses may choose join network groups where colleagues meet todiscuss professional issues and pending legislation.
For nurses interested in a more indirect approach to professional advocacy, theirrole may be to influence and educate the public about nursing and the nursingagenda to reform health care. This may be done by speaking with professional andcommunity groups about healthcare and nursing issues and by interacting directlywith the media. Never underestimate the influence a single nurse may have even inwriting letters to the editor of local newspapers, or by talking about nursing andhealthcare issues with friends, family, neighbors, teachers, clergy, and civic leaders.
Nursing’s Role in the Media
Although nurses have the greatest knowledge about nursing issues, too few are will-ing to interact with the media about vital nursing and healthcare issues. This isespecially unfortunate because both the media and the public place a high trust innurses and want to hear about healthcare issues from a nursing perspective.
Many nurses avoid media exposure because they believe they lack the expertise todo so or because they lack self-confidence. The reality is that “nurses possesstremendous amounts of knowledge, clinical experience, and intellectual and com-munication skills that can contribute to and expand the dialogue and debate sur-rounding healthcare issues and subsequent decision making’’ (Greipp, 2002, p. 35),and self-confidence is usually simply a matter of being prepared for the task at hand.
Trossman (2003) suggests that nurses can ease into the spokesperson role by firstpresenting information on a hot healthcare topic in a group setting where they alreadyfeel comfortable. Nurses should also complete media training programs to increasetheir self-confidence in working with journalists. Regardless, the first few media inter-actions will likely be stressful, just like any new task or learning. Trossman, however,offers the following basic tips to help nurses navigate media waters (Display 6.6):
136 UNIT 2 � Foundation for Effective Leadership and Management
1. Be prepared or at least as prepared as possible given a reporter’s deadline. This meansresearching the topic if there is time, knowing up-to-date information, and knowingthree or four facts or figures that can be cited about pertinent issues.
2. Stick to three or four key points that will drive home your message and repeat themduring the interview.
3. Make it easy for the media by providing them with clear, concise information and bymeeting reporter’s deadlines.
4. Stay on track by sticking to predetermined points, using phrases such as “I think theimportant point is....’’ Also avoid repetition of any negative language a reporter mightpick up on and instead focus on solutions or strategies to solve problems.
5. Don’t be afraid to say that you do not have enough information or expertise to answera question. Be sure not to guess when factual data is needed.
Tips for Interacting with the MediaDisplay 6.6
The bottom line is that “stories about healthcare are hot’’ right now and nursesneed to respond “when the iron is hot’’ (Trossman, 2003, p. 69) to advocate both fortheir profession and for the patients they serve.
INTEGRATING LEADERSHIP ROLES AND MANAGEMENT FUNCTIONS IN ADVOCACY
Nursing leaders and managers recognize they have an obligation not only to advo-cate for the needs of their patients, subordinates, and themselves at a particulartime, but also to be active in furthering the goals of the profession. To accomplishall these types of advocacy, nurses must value autonomy and empowerment.
The leadership roles and management functions, however, to achieve advocacywith patients, subordinates, and for the profession differ greatly. Advocating forpatients requires that the manager create a work environment that recognizespatient’s needs and goals as paramount. This means creating a work culturewhere patients are respected, well informed, and empowered. The leadership rolerequired to advocate for patients is often one of risk taking, particularly whenadvocating for a patient may be in direct conflict with provider or institutionalgoals. Leaders must also be willing to accept and support patient choices thatmay be different from their own.
137CHAPTER 6 � Patient, Subordinate, and Professional Advocacy
Preparing for a Media InterviewYou are the staffing coordinator for a medium-sized community hospitalin California. Minimum staffing ratios were implemented in January 2004.While this has represented an even greater challenge in terms of meetingyour organization’s daily staffing needs, you believe the impetus behindthe legislative mandate was sound. You also are a member of the statenursing association that sponsored this legislation and wrote letters ofsupport for its passage. Your hospital and the state hospital associationfought unsuccessfully against the passage of minimum staffing ratios.
The local newspaper contacted you this morning and wants tointerview you about staffing ratios in general as well as how these ratiosare impacting the local hospital. You approach your CNO and she tells youto go ahead and do the interview if you want, but to remember that youare a representative of the hospital.Assignment: Assume that you have agreed to participate in the interview.1. How might you go about preparing for the interview?2. Identify three or four factual points you can state during the interview
as your sound bites. What would be your primary points of emphasis?3. Is there a way to reconcile any potential conflict between your person-
al feelings about staffing ratios and those of your employer? Howwould you respond if asked directly by the reporter to comment aboutwhether staffing ratios are a good idea?
Learning Exercise 6.6
Advocating for subordinates requires that the manager create a safe and equi-table work environment where employees feel valued and appreciated. When work-ing conditions are less than favorable, the manager is responsible for relaying theseconcerns to higher levels of management and advocating for needed changes. Thesame risk taking that is required in patient advocacy is a leadership role in subordi-nate advocacy, since subordinate needs and wants may be in conflict with theorganization. There is always a risk that the organization will view the manageradvocate as a troublemaker, but this does not provide an excuse for managers to becomplacent in this role. Managers also must advocate for subordinates in creatingan environment where ethical concerns, needs, and dilemmas can be openly dis-cussed and resolved.
Advocating for the profession requires the nurse manager be informed andinvolved in all legislation affecting the unit, organization, and the profession. Themanager also must be an astute handler of public relations and demonstrate skill inworking with the media. It is the leader, however, who proactively steps forth to bea role model and active participant in educating the public and improving healthcare through the political process.
❊ Key Concepts
• Advocacy is helping others to grow and self-actualize and is a leadership role.• Managers, by virtue of their many roles, must be advocates for patients,
subordinates, and the profession.• It is important for the patient advocate to be able to differentiate between
controlling patient choices (domination and dependence) and in assistingpatient choices (allowing freedom).
• Since the 1960s, the NLN, the American Hospital Association, and manystates have passed bills of rights for patients. Although these are not legallybinding, they can be used to guide professional practice.
• In workplace advocacy, the manager works to see that the work environment isboth safe and conducive to professional and personal growth for subordinates.
• Professional issues are ethical issues. When nurses find a discrepancybetween their perceived role and society’s expectations, they have aresponsibility to advocate for the profession.
• If nursing is to advance as a profession, practitioners and managers mustbroaden their sociopolitical knowledge base to understand better thebureaucracies in which they live.
• Because legislators and policy makers are more willing to deal with nursesas a group rather than as individuals, joining and actively supportingprofessional organizations allows nurses to have a greater voice in healthcareand professional issues.
• Nurses need to exert their collective influence and make their concernsknown to policy makers before they can have a major impact on politicaland legislative outcomes.
• Nurses have great potential to educate the public and influence policythrough the media as a result of the public’s high trust in nurses and becausethe public wants to hear about healthcare issues from a nursing perspective.
138 UNIT 2 � Foundation for Effective Leadership and Management
More Learning Exercises and Applications
139CHAPTER 6 � Patient, Subordinate, and Professional Advocacy
Ethics and AdvocacyYou are a new graduate staff nurse in a home health agency. One of yourpatients is a 23-year-old male with acute schizophrenia who was justreleased from the local county, acute care, behavioral healthcare facility,following a 72-hour hold. He has no insurance. His family no longer hascontact with him and he is unable to hold a permanent job. He is non-compliant in taking his prescription drugs for schizophrenia. He is home-less and has been sleeping and eating intermittently at the local homelessshelter; however, they recently asked him not to return, since he isincreasingly agitated and at times, violent. He calls you today and asksyou “to help him with the voices in his head.”
You approach the senior RN case manager in the facility for help inidentifying options for this individual to get the behavioral healthcareservices he needs. She suggests that you tell the patient to go to“Maxwell’s Mini Mart,” a local convenience store, at 3 P.M. today and towait by the counter. Then she tells you that you should contact the policeat 2:55 P.M. and tell them that Maxwell’s Mini Mart is being robbed byyour patient, so that he will be arrested. She states that “she does thiswith all of her uninsured mental health patients, since the state Medicaidprogram offers only limited mental health services and the state penalsystem provides full mental health services for the incarcerated.” She goeson to say that the mini-mart owner and the police are aware of what sheis doing and support the idea since it is the only way “patients really havea chance of getting better.” She ends the conversation by saying, “I knowyou are a new nurse and don’t understand how the real world works, butthe reality is that this is the only way I can advocate for patients like thisand you need to do the same for your patients.”Assignment:1. Will you follow the advice of the senior RN case manager?2. If not, how else might you advocate for this patient? 3. What are the legal, ethical, and advocacy implications of this case?
Learning Exercise 6.7
Letter Writing in AdvocacyIdentify three legislative bills affecting nursing that are currently beingconsidered either in committee, the House of Representatives, or the Sen-ate. Select one and draft a letter to your state assemblyperson or senatorregarding your position on the bill.
Learning Exercise 6.8 A
140 UNIT 2 � Foundation for Effective Leadership and Management
Determining Nursing’s Entry LevelGrandfathering is the term used to grant certain people working withinthe profession for a given period of time, or prior to a deadline date, a privilege of applying for a license without meeting normal requirementssuch as taking the licensing examination. Grandfathering clauses havebeen used to allow licensure for wartime nurses—those with on-the-jobtraining and expertise—even though they did not graduate from anapproved school of nursing.
Some professional nursing organizations are once again proposing thatthe BSN become the entry-level requirement for professional nursing.Some have suggested, as a concession to current ADN and diploma-prepared nurses, that all nurses who have passed the state board ofregistered nursing licensure examination before the new legislation,regardless of educational preparation or experience, would retain thetitle of professional nurse. Non-baccalaureate nurses after that timewould be unable to use the title professional nurse.Assignment: Talk about this issue in a group. Do you believe the BSN- as-entry-level proposal advocates the advancement of the nursingprofession? Is grandfathering conducive to meeting this goal? Would youpersonally support both of these proposals? Does the long-standinginternal dissension about making the BSN the entry level into professionalnursing reduce nursing’s status as a profession? Do lawmakers or thepublic understand this dilemma or care about it?
Learning Exercise 6.9
How Would You Proceed?You are an RN case manager for a large insurance company. SheilaJohannsen is a 34-year-old mother of two small children. She wasdiagnosed with advanced, metastatic breast cancer six months ago.Traditional chemotherapy and radiation seem to have slowed the spreadof the cancer, but the prognosis is not good.
Sheila contacted you this morning to report that she has been in contactwith a physician at one of the most innovative medical centers in the coun-try. He told her that she might benefit from an experimental gene therapytreatment; however, she is ineligible for participation in the free clinicaltrials since her cancer is so advanced. The cost for the treatment then isapproximately $150,000. Sheila states that she does not have the financialresources to pay for the treatment and begs you “to do whatever youcan,to get the insurance company to pay. Otherwise, she will die.”
You know that your insurance company almost always disallows thecost of experimental treatments. You also know that even with theexperimental treatment, Sheila’s probability of a cure is minimal.Assignment: Decide how you will proceed. How can you best advocate for this patient?
Learning Exercise 6.10
Web Links
ANA-PAChttp://www.nursingworld.org/gova/federal/gfederal.htmThis American Nurses Association web page has a large selection of political action sitesto choose from.
ANA—National Awards Programhttp://www.ana.org/about/honaward/staff.htmThis American Nurses Association web page details the award criteria and includesnomination forms for the Staff Nurse Advocate of the Year Award. The Staff NurseAdvocacy Award was established in 1998 to recognize excellence in individual staffnurses who provide direct patient care in all practice settings and who have advocatedfor their patients.
David L. Bazelon Center for Mental Health Lawhttp://www.bazelon.org/about/index.htmThis center is one of the nation’s leading advocates for people with mental disabilities,with precedent setting litigation outlawing institutional abuse and providing protec-tions against arbitrary confinement.
Electronic Policy Networkhttp://movingideas.org/A source for current public policy issues, including healthcare policy. Provides searchengine for current policy issues.
Foundation for Informed Medical Decision Makinghttp://www.fimdm.org/index.htmlThe primary mission of the Foundation for Informed Medical Decision Making(FIMDM) is to strengthen the role patients play in selecting treatments for their med-ical conditions. The site includes a bibliography as well as helpful links.
Sigma Theta Tau International: Media Guide to Health Care Experts(1999–2004)http://www.nursingsociety.org/media/ME_intro.htmlSource for healthcare experts from various medical specialties and practices who are will-ing to interact with the media.
Iroquois Healthcare Alliance—Representing Healthcare Providers in UpstateNew York (2004)http://www.iroquois.org/advocacy.htmProvides sample electronic letters that can be sent to legislators and government officialsregarding multiple pending healthcare bills. Includes links to determine current govern-ment officials who will vote on pending legislation.
ReferencesAmerican Hospital Association. (1973, last revised 1992). “A patient’s bill of rights.” Available
at http://web.carroll.edu/msmillie/bioethics/patbillofrights.htm. Accessed October 14, 2004.American Nurses Association. (1998). Standards of clinical nursing practice (2nd edition).
Washington, D.C.: American Nurses Publishing.
141CHAPTER 6 � Patient, Subordinate, and Professional Advocacy

American Nurses Association. (2004). Scope and standards for nurse administrators (2nd ed.)Washington, D.C.: American Nurses Publishing.
Angelucci, P. (2003). Ethics committees: Guidance through gray areas. Nursing Management,34(6), 30–33.
Benner, P. (2003). Current controversies in critical care. Enhancing patient advocacy andsocial ethics. American Journal of Critical Care, 12(4), 374–375.
Blais, K. K., Hayes, J. S., Kozier, B. & Erb, G. (2002). Professional nursing practice (4th ed.).Upper Saddle River, NJ: Prentice Hall.
Blakeney, B. (2003, January). Addressing the nursing shortage. American Journal of Nursing.Career Guide 2003 (Part 2 of 2). 16.
Byerly, R. T., Carpenter, J. E., & Davis, J. (2001). Managed care and the evolution ofpatient rights. Journal of Nursing Administration’s Healthcare Law, Ethics, & Regulation,3(2), 58–67.
Foley, B. J., Minick, M.P., & Kee, C.C. (2002). How nurses learn advocacy. Journal ofNursing Scholarship, 34(2), 181–186.
Gonzalez, R. (1999). ANA advocates more diversity in nursing. American Journal of Nursing,99(11), 24.
Green , A., & Jordan, C. B. (2002). Workplace advocacy and workplace issues. In Cherry,B. & Jacob, S. R. (Eds.). Contemporary nursing. Issues, trends, & management (2nd ed.).St. Louis: Mosby.
Greipp, M.E. (2002). Forces driving healthcare policy decisions. Policy, Politics, & NursingPractice, 3(1), 35–42.
Huston, C. (1998). We’re not in Kansas anymore: Shaping a new and better healthcaresystem. Revolution: Journal of Nurse Empowerment, 8(3/4), 44–45.
Nursing shortage: Johnson & Johnson campaign aims to increase awareness, generateinterest. (2002). Nursing Economics, 20(2), 93–95.
Quinn, C. A., & Smith, M. D. (1987). The professional commitment: Issues and ethics innursing. Philadelphia: W. B. Saunders.
Reutter, L., & Williamson, D. (2000). Advocating healthy public policy: Implications for baccalaureate nursing education. Journal of Nursing Education, 39, 21–26.
Trossman, S. (2003). Media relations 101. American Journal of Nursing, 103(1), 69–70.
BibliographyAllen, J. E. (2003, July 21). Alone in the ER: People receiving invasive or lifesaving
treatment often want loved ones present, but many hospitals limit access. Los AngelesTimes, pp. F3.
Bass, M. (2003). Oncology nurses’ perceptions of their role in resuscitation decisions.Professional Nurse, 18(12), 710–713.
Bell, S. (2003). CAN addressing professional advocacy. Arizona Nurse, 56(5), 3.Center for American Nurses. (2003). Background on workplace advocacy initiatives at the
national level. Prairie Rose, 72(3), 10.Des Jardin, K. E. (2001). Political involvement in nursing—Politics, ethics, and strategic
action. (Second article in a two-part series). AORN Journal, 74(5), 613–615, 617–618,621–626.
Dinsdale, P. (2000). Robust research is key to nurses’ political influence. Nursing Standard,14(31), 7.
Ecker, H. A. (2003). Washington watch. Politics and responsibility: Lend your voice andmake a difference in the 2004 elections—and beyond. American Journal of Nursing,103(11), 29.
142 UNIT 2 � Foundation for Effective Leadership and Management

Fletcher, M. (2002). Mortgages for nurses? Political will lacking in shortage solution.Canadian Nurse, 98(9), 9.
Grace, P. J. (2001). Professional advocacy: Widening the scope of accountability. NursingPhilosophy, 2(2), 151–162.
Kaiser reverses on transplant denial for HIV-positive patient. (2003). AIDS Policy Law,18(20), 2.
Mason, D. J. (2002). Invisible nurses: Media neglect is one cause of the nursing shortage.American Journal of Nursing, 102(8), 7.
Paniagua, H. (2003). Developing practice nurses’ political voice. Journal of Practical Nursing,14(1), 34–37.
Reutter, L. & Duncan, S. (2002). Preparing nurses to promote health-enhancing publicpolicies. Policy, Politics, & Nursing Practice, 3(4), 294–305.
Schoeter, K. (2003). May the force be with you: Nurses need to break the bonds of theirdependency and become empowered so they can stand up for their patients’ wishes.Surgical Services Management, 9(4), 6–8.
Steele, S. (2003). Analyzing and promoting issues in health policy: Nurse manager’sperspective. Nursing Economic$, 21(2), 80–83.
Ulmer, B. C. (2000). President’s message. Professional advocacy. AORN Journal, 72(1),9–11.
Zavadsky, M. (2003). Expert advice: Insights & innovations from top industryprofessionals. How to change public policy. EMS Insider, 30(11), 6–7.
143CHAPTER 6 � Patient, Subordinate, and Professional Advocacy

Related Documents











