2020 Is there still a place for Penetrating Keratoplasty? Dimitrios Mikropoulos PhD

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

2020Is there still a
place for Penetrating
Keratoplasty?
Dimitrios MikropoulosPhD

HISTORICAL OVERVIEW
Over the past century, keratoplasty has evolved considerably

On 7 December 1905 Eduard Zirm performs
the first successful human corneal transplantation
HISTORICAL OVERVIEW

Anton Elschnigperformed the first
anterior lamellar keratoplasty in 1914
HANUS LIBICKY, M.D.A Personal Sketch of Professor Anton ElschnigSURVEY OF OPHTHALMOLOGY VOLUME 26. NUMBER 5. MARCH-APRIL 1982
HISTORICAL OVERVIEW

Ramon Castroviejo (1904–1987)
Major contribution to popularizing PKP in USA
and globally
HISTORICAL OVERVIEW

The first successful human case of EK was reported by Charles Tillett in 1956
Mark A. Terry, MD. Trans Am Ophthalmol Soc. 2009 Dec; 107: 184–191.
HISTORICAL OVERVIEW

1984 Dr. Eduardo Arenas Archila describes deep lamellar keratoplastyusing injection of intrastromal air
HISTORICAL OVERVIEW
Archila EA. Deep lamellar keratoplasty dissection of host tissue with intrastromal air injection. Cornea. 1984;3(3):217–218

1998. Gerrit Melles reports first human endothelial keratoplastyvia the sclerolimbus
1999. Gerrit Melles describes a technique of deep anterior lamellar keratoplasty (DALK)
In 2006, Melles went on to describe a technique known as Descemet membrane endothelial keratoplasty (DMEK)
HISTORICAL OVERVIEW

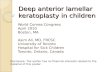
PRESENT
(B) PK
(C) ALK
(D) DALK
(E) DSAEK
(F) DMEKDonald T H Tan et al. Lancet 2012; 379: 1749–61
Penetrating keratoplasty has traditionally been the
treatment of choice for corneal opacification
We now have many different types of keratoplasty, and
many of those involve new techniques as well as
instrumentation


PK Advantages
Can be used for any indication (stromal and/ or endothelial disease)
Potentially the best optical result since no lamellar corneal interface problem exist
Easy learning curve

PK Disadvantages
Increased risks of many complications
compared with lamellar techniques
Endothelial failure, Acute endothelial rejection: 20% by 5 years
Choroidal haemorrhage About 1:200 or less
Regular and irregular astigmatism common
Persistent epithelial defects and corneal melt
Microbial keratitis (5% microbial keratitis, usually suture related)
Donald T H Tan et al. Lancet 2012; 379: 1749–61

ALK Advantages
Replacing only epithelium and corneal stroma
Retention of healthy endothelium
Eliminating endothelial allograft rejection, the major cause of graft failure affecting PK
Reinhart WJ et al. Ophthalmology 2011; 118: 209–18.

ALK Disadvantages
Regular and irregular astigmatism common
Neurotrophic cornea
Persistent epithelial defects and corneal melt
Microbial keratitis (usually suture related)
Reinhart WJ et al. Ophthalmology 2011; 118: 209–18.

ALK compared with PKAdvantages
Extraocular procedure resulting in a low risk of many complications, including transplant rejection and failure
Less topical steroid use than PK or EK
Early suture removal safe

ALK compared with PKDisadvantages
Usually more technically demanding than PK
Fails unless host endothelium is healthy
Regular and irregular astigmatism the same as for PK

EK Advantages
Predictability and
rapid visual rehabilitation due to the elimination of astigmatism
Terry MA Cornea 2006; 25: 873–78Lee WB et al. Ophthalmology 2009; 116: 1818–30

Endothelial failure; Endothelial cell loss higher in EK at the time of surgery, but similar to PK by 12 months postop
Transplant rejection; Endothelial rejection rates probably similar to PK rates
Transplant detachment; Detachment of the posterior lamellar in 5–30% of cases. Most reports are less than 10%. Can be re-attached by re-injecting air
Terry MA Cornea 2006; 25: 873–78Lee WB et al. Ophthalmology 2009; 116: 1818–30
EK Disadvantages

EK compared with PKAdvantages
EK is much safer and simpler than PK
No induced astigmatism resulting in early visual recovery and better visual outcomes

EK compared with PKDisadvantages
Suboptimum visual results in:
• Opacities in residual stroma
• Interface opacities
• Transplant folds

PENETRATING vs LAMELLAR
Ti SE, Scott JA, Janardhanan P, Tan DT. Therapeutic keratoplasty for advanced suppurative keratitis. Am J Ophthalmol 2007; 143: 755–62.
Lamellar surgery offers several advantages over penetrating keratoplasty by replacing only the diseased layer of the cornea
PK still has a role in corneal transplant because not all patients are candidates for lamellar procedures
PK remains the dominant technique for the management of deep-seated corneal infection such as fungal keratitis unresponsive to medical therapy

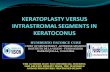
PENETRATING KERATOPLASTY
Pre op One week postop
Pre op One week postop

CONCLUSION
Corneal transplantation has changed dramatically since its early days over 100 years ago, when the gold standard of surgery was full thickness penetrating keratoplasty
The main standard of care nowadays is to remove only the diseased part of the recipient cornea and to replace it with a donor corneal lamella
There are still a significant number of patients having corneal diseases involving all corneal layers, and for which PK will remain the only way to regain their vision

“Study the past if you would define the future”
Confucius
Related Documents