1.40 p=0.145

1.40 p=0.145
Jan 01, 2016
1.40 p=0.145. Epidemiologic Association. Chance Bias Confounding Truth. CHANCE. “…the results of the retrospective cohort study was inconclusive with all but two of the data being non-significant.” - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1.40p=0.145


Epidemiologic Association
• Chance
• Bias
• Confounding
• Truth

CHANCE
• “…the results of the retrospective cohort study was inconclusive with all but two of the data being non-significant.”
• “…analysis of self-reported cancer rates for children who had played at the site (Exhibit E) shows that while that was a positive association, the results were not statistically significant. “

1387 study participants, 73 self reported cancers

Self-Reported Cancer
Yes No
Nyanza Site Yes 36 547 236
Waste Ponds & Lagoons
No 36 767 1,151
72 1314 1386OR = 1.40 (95% CI 0.87, 2.25)
p=0.16
Assume MDPH Study ResultsWere as Below
What Does p=0.16 mean?
OR=1.40
P=0.08 P=0.0895% CI 0.87, 2.25
P=0.16

Self-Reported Cancer
Yes No
Nyanza Site Yes 36 547 236
Waste Ponds & Lagoons
No 36 767 1,151
72 1314 1386OR = 1.40 (95% CI 0.87, 2.25)
p=0.16
Self-Reported Cancer
Yes No
Nyanza Site Yes 72 1,094 1,166
Waste Ponds & Lagoons
No 72 1,534 1,606
144 2628 2772
OR = 1.40 (95% CI 1.00, 1.96)p=0.047
Assume MDPH Study ResultsWere as Below
50% Participation
What if MDPH StudyHad Full Participation?
X 2

What is Bias?• Bias means that there is a systematic error in the
design or results• The measured (or estimated) variable is different
from the truth.• Depends on the question!
– Biased sample sample does not represent population– Biased exposure exposure ≠ true value– Diagnostic bias Disease ≠ true disease – Epidemiologic Bias association ≠ truth
• NOTE: Biased sample, or exposure, or disease does not mean association is biased (epidemiologic bias)!!

SELECTION BIAS
• “Selection bias may play a significant role if the 1,387 people out of 2,054 who agreed to participate were more likely to have cancer compared to those who declined participation.”
• “… individuals who may have already died either from cancer or unknown unrelated causes and thus were untraceable would significantly bias our findings.”
• “There is a chance of those people with cancer having enrolled in the study versus those who did not have cancer.”

Self-Reported Cancer
Yes No
Nyanza Site Yes 36 547 236
Waste Ponds & Lagoons
No 36 767 1,151
72 1314 1386OR = 1.40 (95% CI 0.87, 2.25)
p=0.16
OR = 1.40 (95% CI 1.00, 1.97)p=0.052
What if 50% of the Cancer Cases Died Before MDPH Study ?
Ca X 2Actual Cancer
Yes No
Nyanza Site Yes 72 547 619
Waste Ponds & Lagoons
No 72 767 839
144 1314 1458
Assumed MDPH Study Results

Self-Reported Cancer
Yes No
Nyanza Site Yes 36 547 236
Waste Ponds & Lagoons
No 36 767 1,151
72 1314 1386OR = 1.40 (95% CI 0.87, 2.25)
p=0.16
OR = 1.40 (95% CI 0.93, 2.11)p=0.104
What if Exposed People Were Twice as Likely to Participate ?
Ca X 2
Assumed MDPH Study Results
Self-Reported Cancer
Yes No
Nyanza Site Yes 72 1,094 1,166
Waste Ponds & Lagoons
No 36 767 803
108 1,861 1969

SELECTION BIAS
• “There is a chance of those people with cancer having enrolled in the study versus those who did not have cancer.”
• Only 40 out of 73 cancers confirmed

Self-Reported Cancer
Yes No
Nyanza Site Yes 36 547 236
Waste Ponds & Lagoons
No 36 767 1,151
72 1314 1386OR = 1.40 (95% CI 0.87, 2.25)
p=0.16
OR = 1.39 (95% CI 0.74, 2.60)p=0.30
What if only 40 Confirmed Cancer Cases Included ?
Assumed MDPH Study Results
Confirmed Cancer
Yes No
Nyanza Site Yes 20 563 583
Waste Ponds & Lagoons
No 20 783 803
40 1346 1386

SELECTION BIAS
• Possible sources:– Selection of eligible participants– Differential participation– Loss to follow-up
• Requires:– Selection based on both exposure and
outcome
• SELECTION DOES NOT IMPLY SELECTION BIAS

INFORMATION BIAS
• “The difference between self-reporting and confirmed cases especially in view of the prolonged resentment held by the community members towards Nyanza lends some doubt to the results.”

CONFOUNDING BIAS
• “A number of potential confounders have been considered, others such as the possibility of other or previously existing sources of contamination have not been ruled out.”
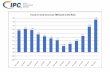
• Age, sex, race ?

1.40p=0.145
1.17p=0.50
0.78p=0.58
1.35p=0.20
1.17p=0.50
1.36p=0.17
1.47p=0.106
1.26p=0.31
1.82p=0.176

Confounding Bias
• Confounding bias results when the association between exposure and disease is altered (biased) by a third variable (i.e. the confounder)
• Confounder by definition:– An independent determinant for the outcome (i.e. it is associated
with the outcome among the unexposed) AND – Associated with the exposure of interest through a noncausal
mechanism.
• Confounding– Inevitable in all studies. It is not investigator induced; it is a basic
characteristic of nature.– Can be minimized, but it is never possible to know effects of all
confounders– Best one can do is design study to reduce confounding and
collect information on known or suspected confounders to control in analysis.

Evaluating of Confounding
• Crude vs. Adjusted Associations– Confounding bias is the difference between the crude (unadjusted)
effect estimate and the effect estimate adjusted for the posited confounder.
– Rule of Thumb: at least a 10% change in effect estimate produced by adjustment for a true confounder
• Test of significance– Have no role in the identification or assessment of confounding
– The association of the confounder with the outcome or exposure does not have to be statistically significant to produce a substantial difference between crude and adjusted effect estimates.
• Residual Confounding– Confounding Bias remains after inclusion of the confounder in the
analysis due to mismeasurement of confounder or inadequate model for the confounder

Control of Confounding in Design
• Randomization– Random allocation of exposure (clinical trial)– Cannot (unlikely) to be realized in environmental epidemiology
• Restriction– Restrict participation by potential confounder
• No confounding if potential confounder does not vary across subjects
– Straight forward and inexpensive– Reduces number of subjects (and power)– Residual confounding possible– Limits generalizability (extrapolation)
• Improves validity of study
• Matching– Reduces confounding in cohort study– Induces confounding in case control
• Must control for matching variables
– Improves efficiency to control in analysis

EFFECT MODIFICATION
• “We already know that genetics plays a large role in many cancer etiologies. Family history is a significant confounder within our findings.”


Effect Modification
• Variation in the association between outcome and exposure across levels of some other variable.
• Confounders can also be effect modifiers.

Epidemiologic Association
• Chance
• Bias
• Confounding
• Truth

CAUSALITY
• “… the biological plausibility and the latency period of each type of cancer mentioned needs to be established in this population.”
• “Dose-response relationships need to be strengthened.”

CAUSALITY
• “We would recommend the use of GIS mapping techniques, a more detailed qualitative assessment of exposure histories among cases and controls in Ashland and the consideration of other communities with similar exposures to liquid hazardous waste during the same time period.”
• “Coordination with other communities with similar exposures across the country may serve to increase the numbers of exposures and cancers and improve statistical analysis.”

AUSTIN BRADFORD HILLThe Environment and Disease: Association or
Causation?Proc Royal Soc Med 1965; 58:295-300.
• Strength• Consistency• Specificity• Temporality• Biological
Gradient
• Plausibility• Coherence• Experiment• Analogy

Hill Criteria for Causation
• STRENGTH– First upon my list I would put the
strength of the association.– In thus putting emphasis upon the
strength of an association we must, nevertheless, look at the obverse of the coin. We must not be too ready to dismiss a cause-and-effect hypothesis merely on the grounds that the observed association appears to be slight.
Top

Hill Criteria for Causation
• CONSISTENCY.– Has it been repeatedly observed by
different persons, in different places, circumstances and times?
– ...there will be occasions when repetition is absent or impossible and yet we should not hesitate to draw conclusions.
Top

Hill Criteria for Causation
• SPECIFICITY– ...specificity of the association, the third
characteristic which invariably we must consider.
– ...if specificity exists we may be able to draw conclusions without hesitation; if it is not apparent, we are not thereby necessarily left sitting irresolutely on the fence.
Top

Hill Criteria for Causation
• TEMPORALITY– ...temporal relationship of the
association - which is the cart and which is the horse?
Top

Hill Criteria for Causation
• BIOLOGICAL GRADIENT– ...if the association is one which can
reveal a biological gradient, or dose-response curve, then we should look most carefully for such evidence.
Top

Hill Criteria for Causation
• COHERENCE– ...cause-and-effect interpretation of our
data should not seriously conflict with the generally known facts of the natural history and biology of the disease...
Top

Hill Criteria for Causation
• EXPERIMENT– ... Occasionally it is possible to appeal to
experimental, or semi-experimental, evidence. For example, because of an observed association some preventive action is taken.
Top

Hill Criteria for Causation
• PLAUSIBILITY– It will be helpful if the causation we
suspect is biologically plausible. But this is a feature I am convinced we cannot demand. What is biologically plausible depends upon the biological knowledge of the day.
Top

Hill Criteria for Causation
• ANALOGY– In some circumstances it would be fair
to judge by analogy.
Top

Hill Criteria for Causation
• TESTS OF SIGNIFICANCE– No formal tests of significance can
answer those questions. Such tests can, and should remind us of the effects that the play of chance can create, and they will instruct us in the likely magnitude of those effects. Beyond that they contribute nothing to the 'proof' of our hypothesis.

Hill Criteria for Causation
• CONCLUSIONS– All scientific work is incomplete -
whether it be observational or experimental. All scientific work is liable to be upset or modified by advancing knowledge. That does not confer upon us a freedom to ignore the knowledge we already have, or to postpone the actions that it appears to demand at a given time.

CAUSALITY
• “It is crucial that with further testing and investigations, we do not ignore action that must be taken in order to minimize exposure to the residents of Ashland.”
Related Documents