Advances in mechanical ventilation Dr. Venugopal Reddy. MD, EDIC, FCARCSI Associate Professor of Anesthesia & CCM Director of Surgical Critical Care Medicine Penn State College of Medicine Hershey Medical Center, Hershey Pennsylvania, USA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Advances in mechanical ventilation
Dr. Venugopal Reddy. MD, EDIC, FCARCSIAssociate Professor of Anesthesia & CCMDirector of Surgical Critical Care Medicine
Penn State College of Medicine Hershey Medical Center, Hershey
Pennsylvania, USA

Dual control modes2000: ARDS Network. Ventilation with low VTTraditional versus Dual control
Dual control Auto-regulated pressure controlled modes delivering desired tidal volume with-in-a-breath (PC to VC)breath-breathCombination of both
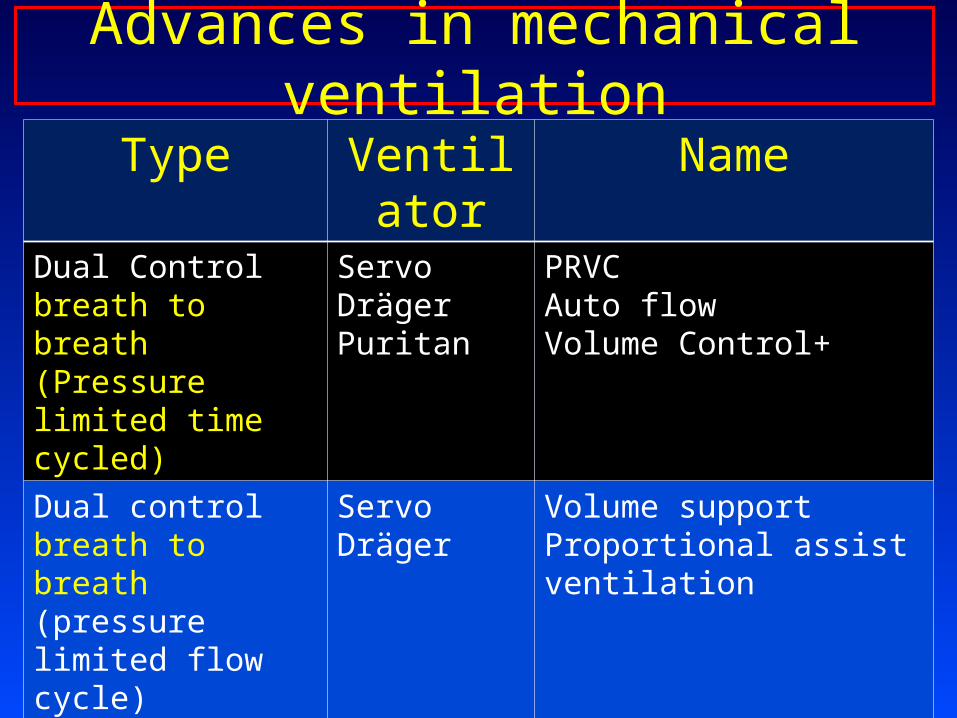
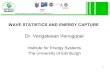
Advances in mechanical ventilation
Type Ventilator
Name
Dual Control breath to breath (Pressure limited time cycled)
ServoDrägerPuritan
PRVCAuto flowVolume Control+
Dual control breath to breath (pressure limited flow cycle)
ServoDräger
Volume supportProportional assist ventilation
Modes that allow spontaneous breathing
Dräger-Evita 4Servo Maquet
BiPAP and APRVBi Vent
Dual Control breath to breath
Hamilton Galileo
Adaptive Support ventilation
Pressure Regulated Volume Control Ventilation
Volume control ventilation
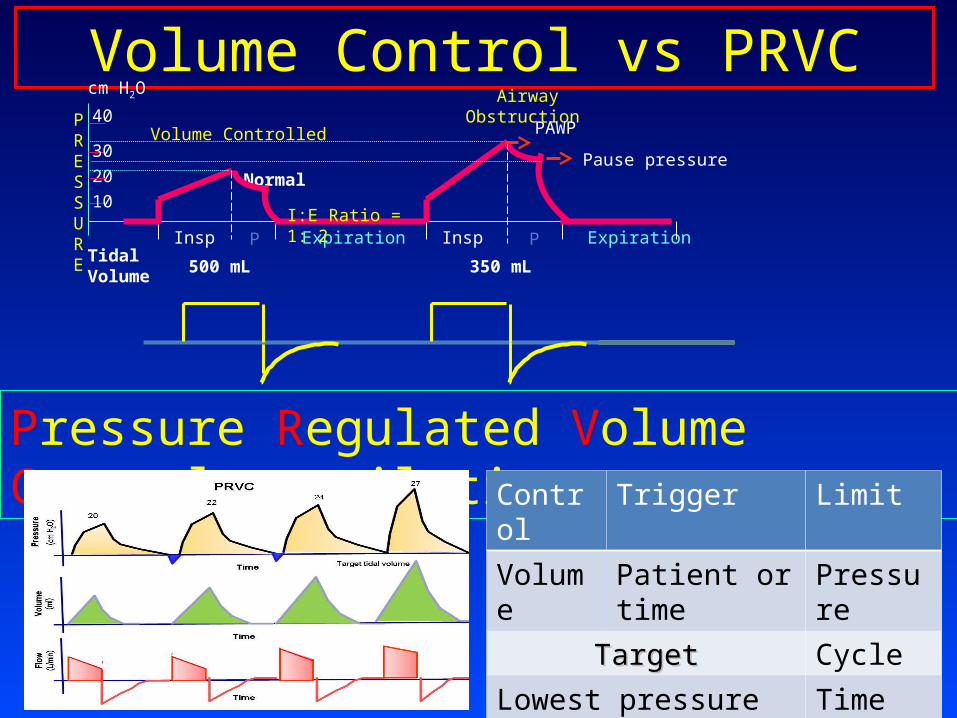
Volume Control vs PRVC
Pressure Regulated Volume Control ventilation
Volume Controlled
Airway Obstruction
Normal
Insp P Expiration
PRESSURE
cm H2O
Insp P Expiration
10
20
30
40
Tidal Volume
500 mL 350 mL
PAWP
Pause pressure
I:E Ratio = 1: 2
Control Trigger Limit
Volume Patient or time Pressure
TargetTarget Cycle
Lowest pressure for set volume
Time

(1)Test breath (5 cm H2O above PEEP) (2)Pressure increases to deliver set tidal volume (3)maximum available pressure (4)breath delivered at preset VE, f, and TI
(5)when VT corresponds to set value, pressure remains constant(6)if preset volume increases, pressure decreases
Pressure regulated volume control (PRVC)

Pressure Regulated Volume Control
Weaning is much easier Apnea: Pressure controlled time cycled breath Patient triggers 2 breaths switches to VSV Maximum pressure at any time is <5 cm H20
below the pressure alarm Activation of alarm: indicates change in
patient lung mechanics and requires evaluation
Pressur
eFlow
Volume Set tidal volume
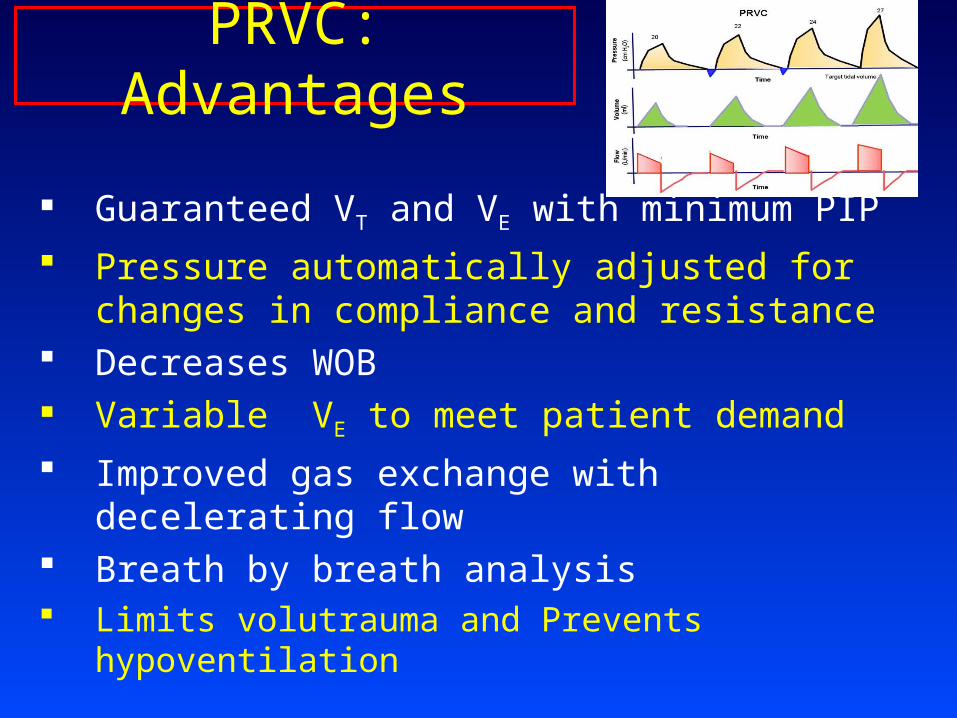
PRVC: Advantages
Guaranteed VT and VE with minimum PIP Pressure automatically adjusted for changes in
compliance and resistance Decreases WOB Variable VE to meet patient demand Improved gas exchange with decelerating flow Breath by breath analysis Limits volutrauma and Prevents hypoventilation
Pres
sure
Flow
Volu
me
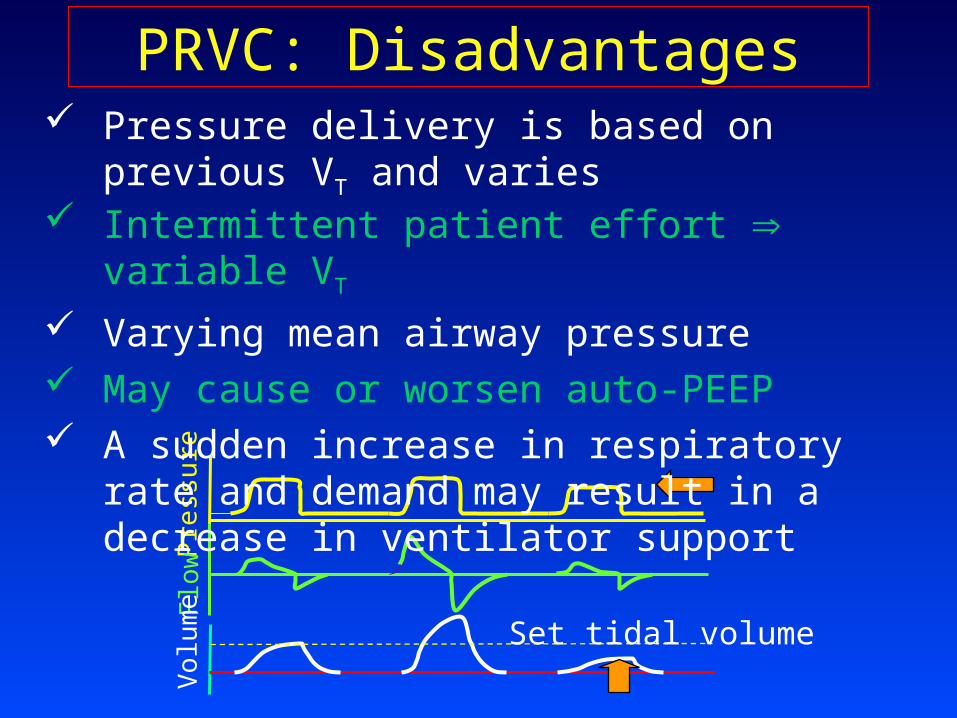
Set tidal volume
PRVC: Disadvantages Pressure delivery is based on previous VT and varies Intermittent patient effort variable VT
Varying mean airway pressure May cause or worsen auto-PEEP A sudden increase in respiratory rate and demand
may result in a decrease in ventilator support
PRVC: Indications
Patient who require the lowest possible pressure and a guaranteed consistent VT
When inspiratory pressure varies due to intra-abdominal pressure (laparoscopy, robotic)
ALI/ARDS Patients requiring high and/or variable MV Patient with changes in Compliance or
Resistance
Pressure Support
Volume Support

Volume support ventilation ServoControl Trigger Limit Target Cycle
Pressure Patient Pressure Volume Flow
5 cm H2O
Apnea
Constant exp. Flow
1 2 3 4 5
Upper Pressure limit 5 cm H2O
PRVC
Pressure support
0
5
10Pressure
Trigger Trigger Trigger
PEEP
Apnea
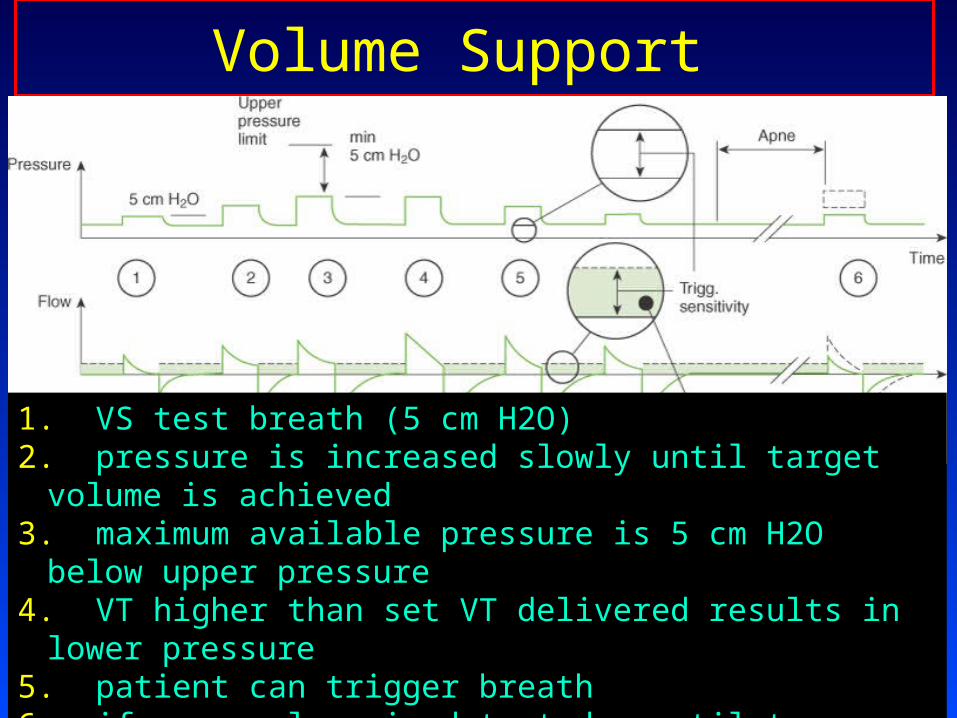
Volume Support
1. VS test breath (5 cm H2O)2. pressure is increased slowly until target volume is achieved3. maximum available pressure is 5 cm H2O below upper pressure4. VT higher than set VT delivered results in lower pressure5. patient can trigger breath6. if apnea alarm is detected, ventilator switches to PRVC
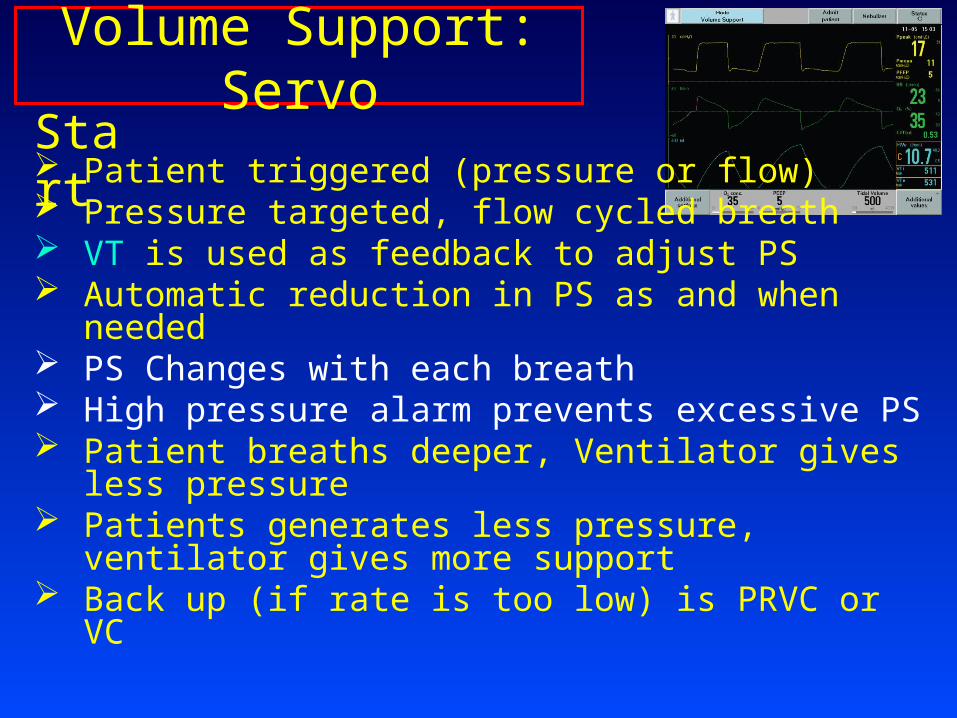
Volume Support: ServoStart Patient triggered (pressure or flow) Pressure targeted, flow cycled breath VT is used as feedback to adjust PS Automatic reduction in PS as and when needed PS Changes with each breath High pressure alarm prevents excessive PS Patient breaths deeper, Ventilator gives less
pressure Patients generates less pressure, ventilator gives
more support Back up (if rate is too low) is PRVC or VC
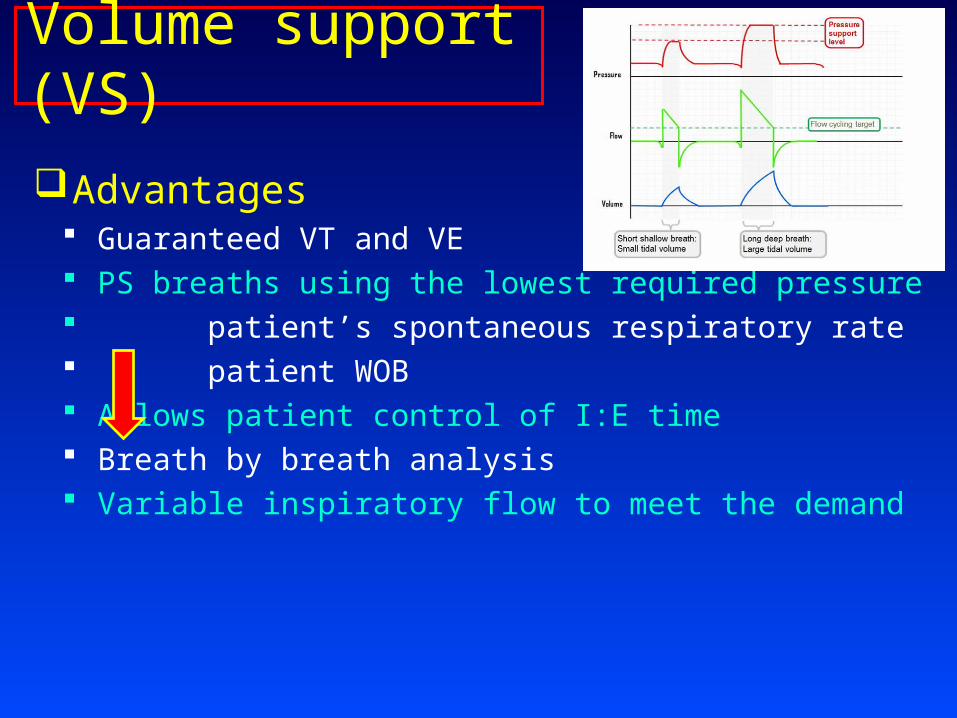
Volume support (VS)
Advantages Guaranteed VT and VE PS breaths using the lowest required pressure patient’s spontaneous respiratory rate patient WOB Allows patient control of I:E time Breath by breath analysis Variable inspiratory flow to meet the demand

Volume support (VS)
Disadvantages Spontaneous ventilation required VT selected may be too large or small for patient Varying mean airway pressure Auto-PEEP may affect proper functioning A sudden increase in respiratory rate and demand
may result in a decrease in ventilator support

Volume Support (VS)
Indications• Spontaneous breathing patient who require
minimum VE
• Patients who have inspiratory effort who need adaptive support
• Patients who are asynchronous with the ventilator• Used for patient who are ready to wean
Pressure Controlled Inverse Ratio ventilation (PC-IRV)
Airway Pressure Release Ventilation (APRV)
Pressure Controlled ventilationWith Normal I:E Ratio
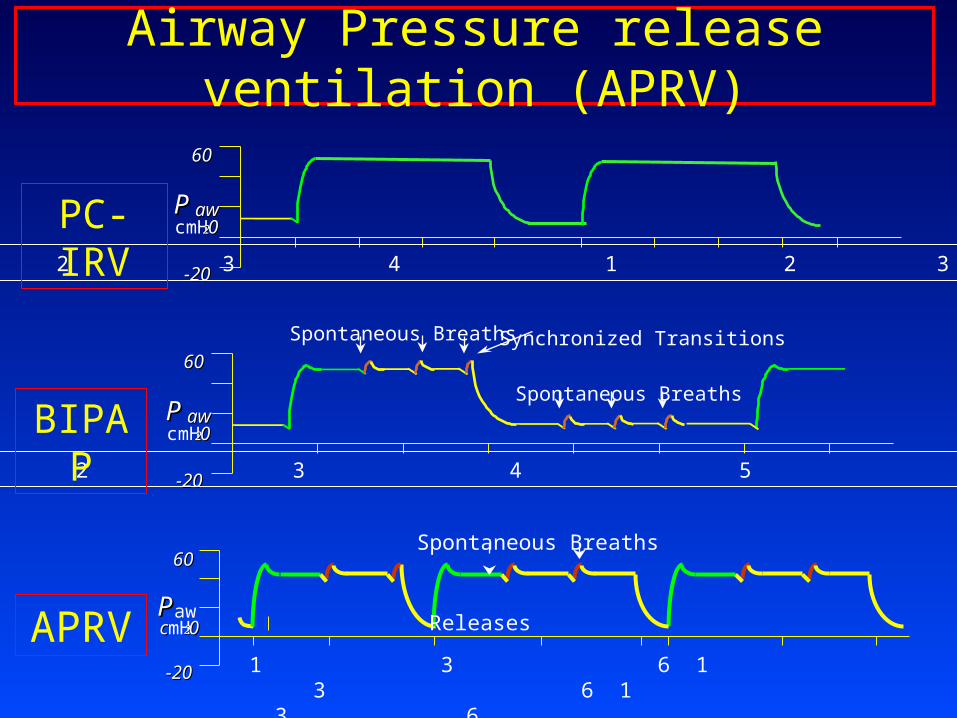
Airway Pressure release ventilation (APRV)
Synchronized TransitionsSpontaneous Breaths
Spontaneous BreathsPP awawcmH2200
6060
-20-20 1 2 3 4 5 6 7
PPawccmH2200
6060
-20-20 1 3 6 1 3 6 1 3 6
Spontaneous Breaths
Releases
PP awawcmH2200
6060
-20-20 1 2 3 4 1 2 3 4
PC-IRV
BIPAP
APRV
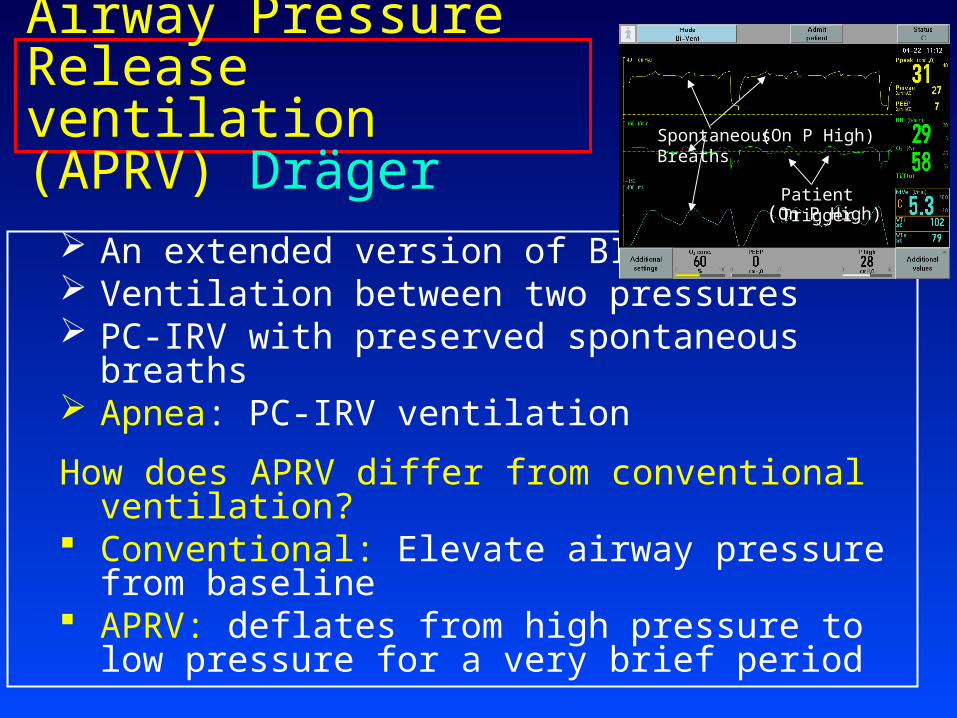
Airway Pressure Release ventilation (APRV) Dräger
An extended version of BIPAP Ventilation between two pressures PC-IRV with preserved spontaneous breaths Apnea: PC-IRV ventilation
How does APRV differ from conventional ventilation?
Conventional: Elevate airway pressure from baseline
APRV: deflates from high pressure to low pressure for a very brief period
Spontaneous Breaths
Patient Trigger(On P High)
(On P High)
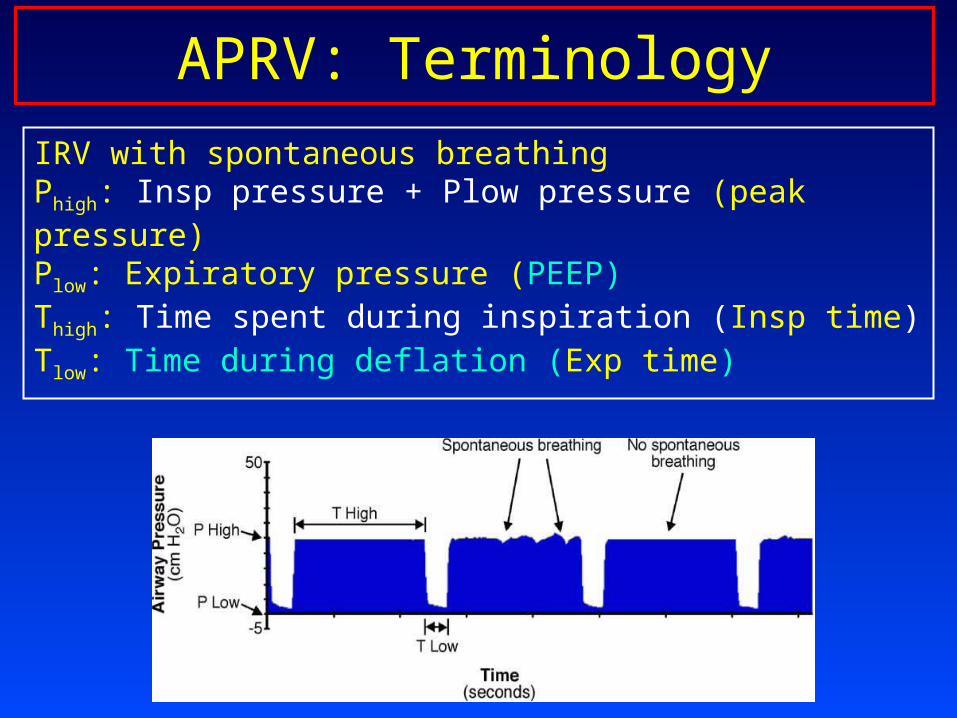
APRV: Terminology
IRV with spontaneous breathingPhigh: Insp pressure + Plow pressure (peak pressure)Plow: Expiratory pressure (PEEP)Thigh: Time spent during inspiration (Insp time)Tlow: Time during deflation (Exp time)
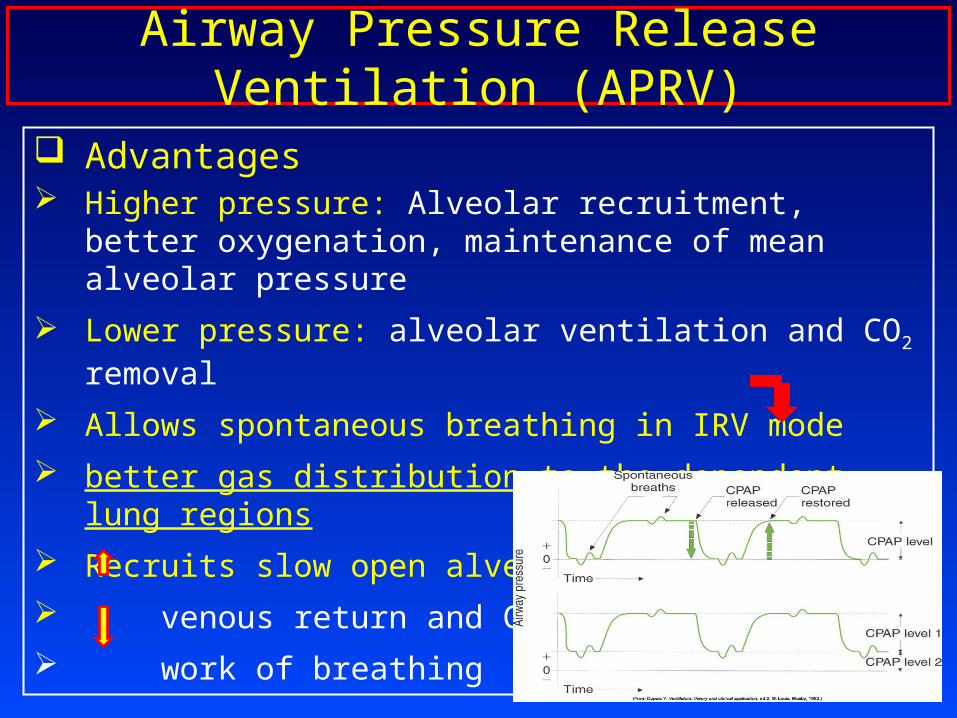
Airway Pressure Release Ventilation (APRV)
Advantages Higher pressure: Alveolar recruitment, better
oxygenation, maintenance of mean alveolar pressure
Lower pressure: alveolar ventilation and CO2 removal
Allows spontaneous breathing in IRV mode better gas distribution to the dependent lung regions Recruits slow open alveoli venous return and CO work of breathing

Airway Pressure Release Ventilation (APRV)
Indication ARDS Hypoxemia Atelectasis high PEEP
Settings P high plateau pressure of conventional
ventilation T high Inspiratory time (5.5-6.5 sec) P low 0 cm H20(PEEP) (intentional auto-PEEP) T Low 0.4-0.8 sec
T Low should be equal to 40%-50% of peak expiratory flowdo not let expiratory flow returning to zero
Airway Pressure Release Ventilation (APRV)
Disadvantages and Risks Variable VT with change in lung compliance and
resistance Could be harmful to patients with high expiratory
resistance (i.e., COPD or asthma) Caution: hemodynamically unstable patients Increase RV after load, and PHT Spontaneous breath during T low: Increase WOB Worsening of air-leak (BPF) Auto-PEEP is usually present
PC ventilationPS ventilation
SIMV
Adaptive support ventilation
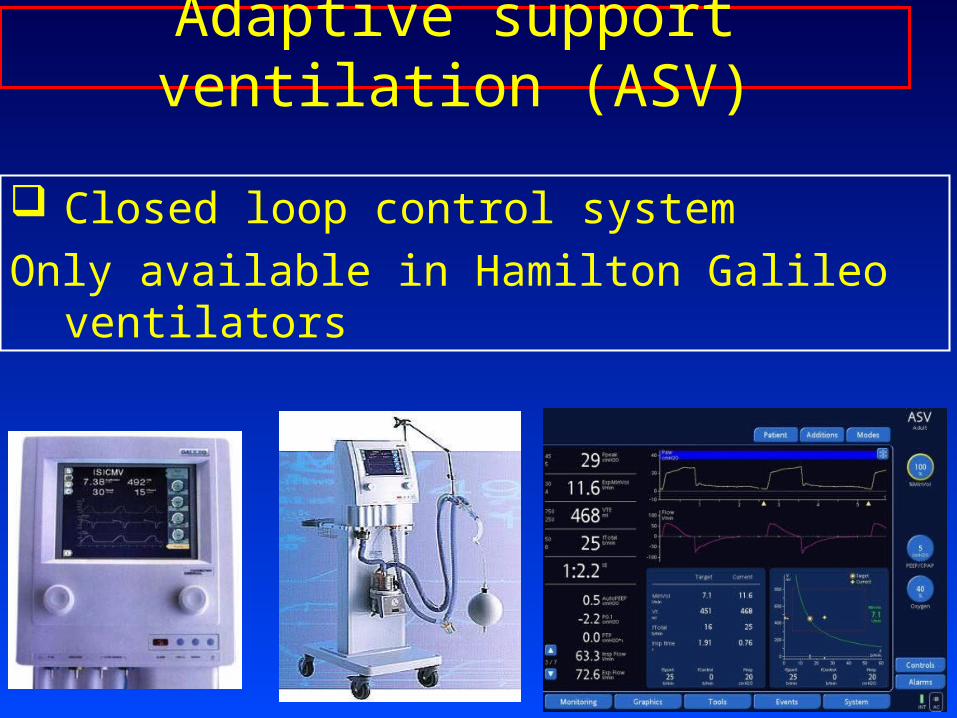
Adaptive support ventilation (ASV)
Closed loop control systemOnly available in Hamilton Galileo ventilators
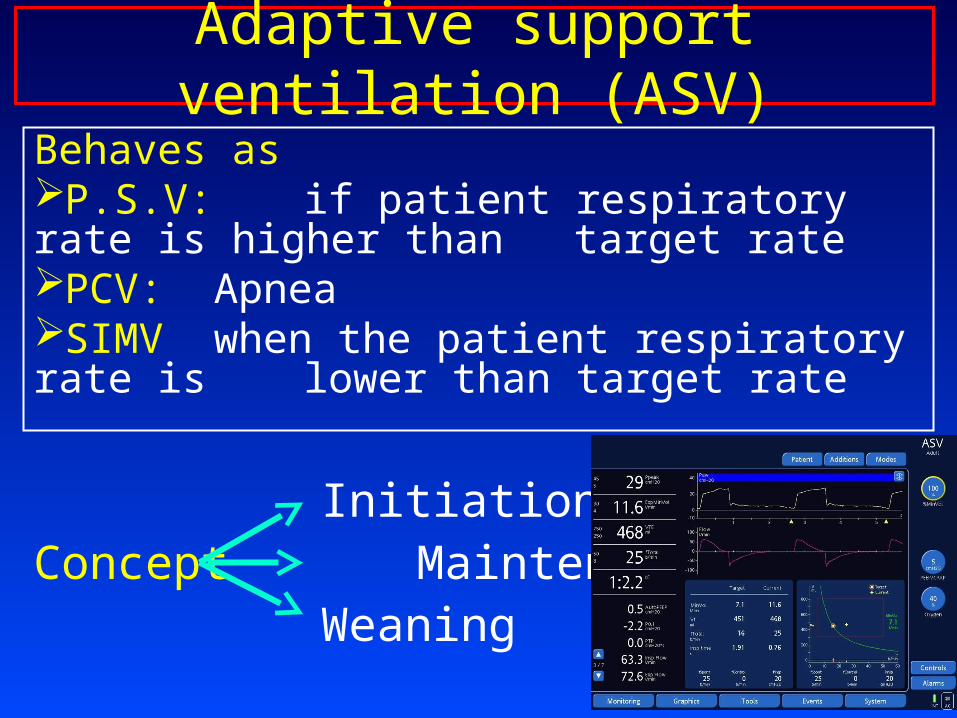
Adaptive support ventilation (ASV)Behaves asP.S.V: if patient respiratory rate is higher than
target ratePCV: ApneaSIMV when the patient respiratory rate is
lower than target rate
InitiationConcept Maintenance
Weaning
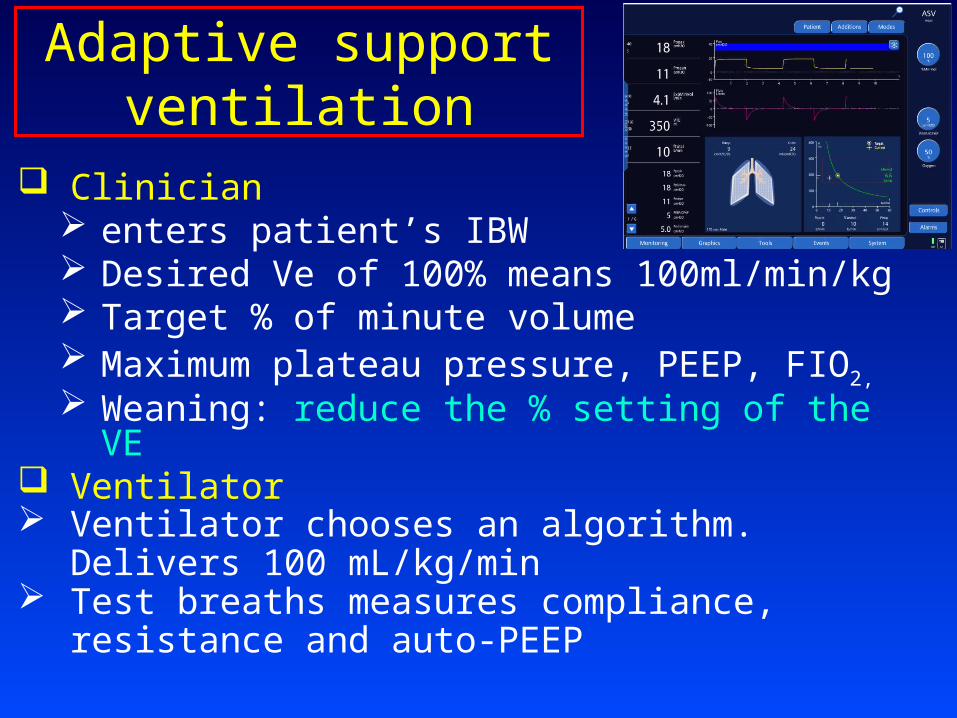
Adaptive support ventilation
Clinician enters patient’s IBW Desired Ve of 100% means 100ml/min/kg Target % of minute volume Maximum plateau pressure, PEEP, FIO2, Weaning: reduce the % setting of the VE
Ventilator Ventilator chooses an algorithm.
Delivers 100 mL/kg/min Test breaths measures compliance, resistance
and auto-PEEP

Adaptive Support ventilation: Advantages
Guaranteed VT and VE Minimal patient WOB Ventilator adapts to the patient Prevents tachypnea, auto-PEEP, and
dyspnea Weaning is done automatically Variable flow to meet patient demand Decelerating flow waveform Breath by breath analysis

Adaptive support ventilation: Disadvantages
Does not allow direct programing of VT, RR, I:E ratio Inability to recognize and adjust to changes in
alveolar VD Possible respiratory muscle atrophy Varying mean airway pressure Patients with COPD, a longer TE may be required Sudden increase in respiratory rate and demand
may result in a decrease in ventilator support Algorithm tends to ventilate with low VT & high RR
Related Documents


![Dr. Venugopal Arumuru · Dr. Venugopal Arumuru Room N 03/2016–[To] Assistant Professor, IIT Bhubaneswar, India 09/2014–02/2016 Lead Engineer/Technologist, GE Measurement & Control,](https://static.cupdf.com/doc/110x72/5f05eed37e708231d41572a6/dr-venugopal-dr-venugopal-arumuru-room-n-032016ato-assistant-professor-iit.jpg)