© 2011 National Safety Council 21-1 PEDIATRIC PATIENTS LESSON 21

© 2011 National Safety Council 21-1 PEDIATRIC PATIENTS LESSON 21.
Dec 14, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
© 2011 National Safety Council 21-1
PEDIATRIC PATIENTSLESSON 21
© 2011 National Safety Council 21-2
Introduction
• 5-10% of emergency responses involve children
• Children maybe unable to tell you what happened
• Because parents, family members or caretakers are often frightened and worried, communication is particularly important
• Size and anatomical difference make care different

© 2011 National Safety Council 21-3
Interacting with Infants, Children and Caretakers
• Prevent anxiety and panic in child and caretakers
• Tell child your name
• Say you are there to help
• Be especially sensitive to child’s feelings
• Ensure a parent or caretaker has been called
© 2011 National Safety Council 21-4
Interacting with Infants, Children and Caretakers (continued)
• Stay at child’s level, be friendly and calm
• Observe child for clues about how best to be reassuring
• Young child may be comforted by favorite toy or touch
• Always be honest with child and caretakers
• Keep patient and caretakers informed
© 2011 National Safety Council 21-5
Interacting with Infants, Children and Caretakers (continued)
• Don’t separate child from caretaker
• Approach slowly from a safe distance
• Talk with both caretaker and child
• Observe child and caretaker before touching child
• Remain calm
© 2011 National Safety Council 21-6
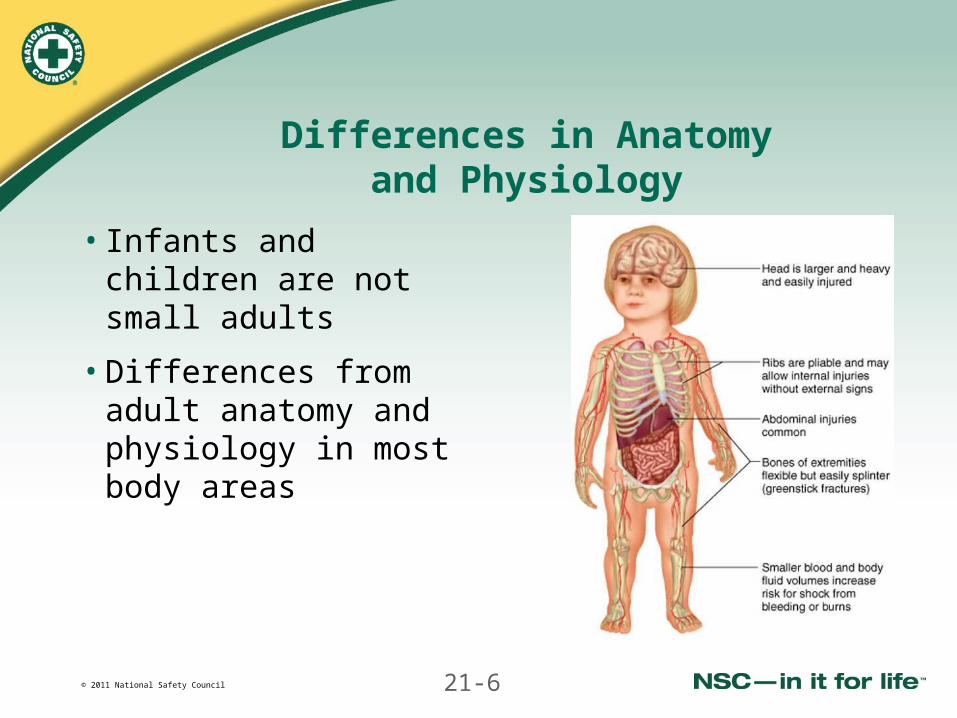
Differences in Anatomyand Physiology
• Infants and children are not small adults
• Differences from adult anatomy and physiology in most body areas
© 2011 National Safety Council 21-7
Head and Neck
• Smaller airway easily blocked
• Tongue relatively larger, can easily block airway
• When opening airway, don’t hyperextend neck
• Pad beneath shoulders to prevent flexion of neck
• Suctioning secretions from nose can improve breathing problems
• Head of infant or young child relatively larger and heavier
• “Soft spots” (fontanels) put head at greater risk
© 2011 National Safety Council 21-8
Chest and Abdomen
• Children compensate for respiratory problems or shock for short periods
• Compensation followed by rapid decompensation
• Use of accessory muscles a clear sign of breathing problem
• Slow pulse rate generally indicates hypoxia
© 2011 National Safety Council 21-9
Chest and Abdomen (continued)
• More susceptible to hypothermia
• Blood loss may be fatal
• More easily dehydrated (diarrhea or vomiting)
• Internal injuries are more likely with trauma
© 2011 National Safety Council 21-10
Extremities
• Bones easily fracturedby trauma
© 2011 National Safety Council 21-11
Assessing Infants and Children
• Assessment uses same steps as for adults
• Correct problems threatening airway, breathing or circulation as soon as found
• Assessment varies based on age and nature of problem
• Reassess continuously until emergency care is transferred
© 2011 National Safety Council 21-12
Scene Size-Up
• Begin by observing scene
• Note how child and caretakers interact
• Gather information from caretakers
• Observe the environment
• Note location and position in which patient is found
© 2011 National Safety Council 21-13
General Impression: Pediatric Triangle
• You can often tell how ill or severely injured child is from a distance in 15-30 seconds
• Remember 3 key elements: Consider child’s general
appearance Assess child’s work
of breathing Assess skin color
• These observations also help assess child’s mental status

© 2011 National Safety Council 21-14
Assess Mental Status
• Quality of crying or speaking
• Emotional state
• Behavior
• Response to caretakers
• How attentive child is to you
© 2011 National Safety Council 21-15
Possible Causes of Abnormal Findings in Triangle Assessment
• Respiratory distress or failure
• Shock
• Cardiopulmonary failure or arrest
• Other abnormal conditions
© 2011 National Safety Council 21-16
Primary Assessment
• Primary assessment follows same steps as adult
© 2011 National Safety Council 21-17
Responsiveness, Breathing, Circulation

© 2011 National Safety Council 21-18
Responsiveness
• Responsive if purposively moving, crying or speaking, or coughing
• Unless obviously responsive, tap child on shoulder and shout, “Are you OK?” or flick foot of infant
• Unresponsiveness is potentially life-threatening condition summon additional EMS resources
• If child is responsive, assess level using AVPU scale
• Assess pupil size, equality and reaction to light
• Check whether all extremities are moving equally
© 2011 National Safety Council 21-19
Breathing
• While assessing for responsiveness, look for normal breathing
• Child who can speak, cough or make other sounds is breathing and has heartbeat
• Reflex gasping (agonal respirations) is not normal breathing
• Lack of breathing may be caused by cardiac arrest, an obstructed airway or other causes
• If patient is not breathing normally, quickly check for pulse
© 2011 National Safety Council 21-20
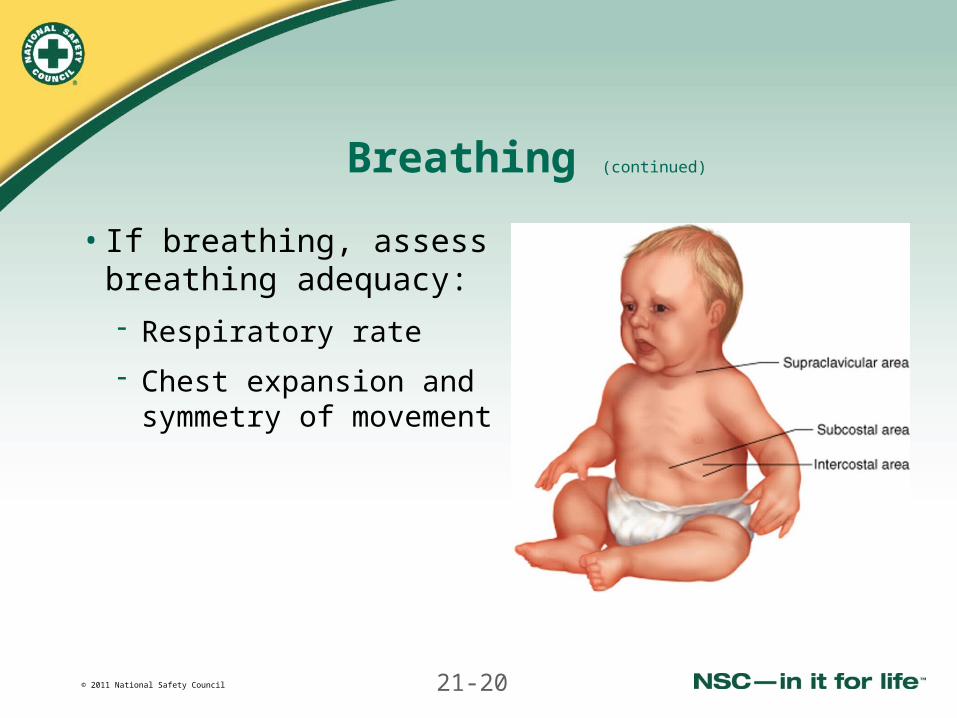
Breathing (continued)
• If breathing, assess breathing adequacy:
Respiratory rate
Chest expansion and symmetry of movement
© 2011 National Safety Council 21-21
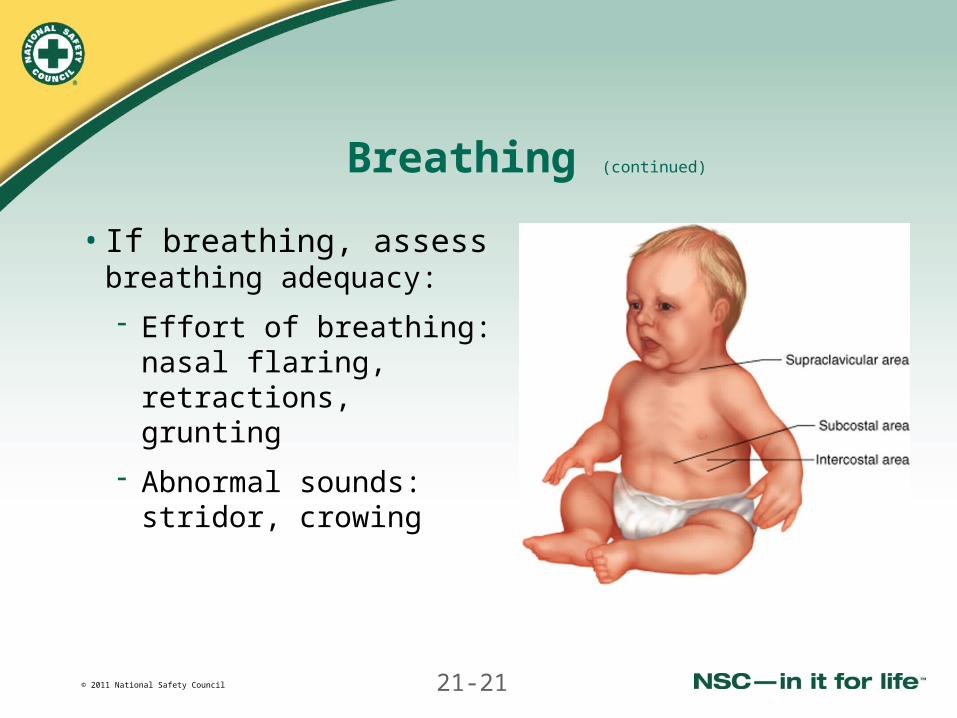
Breathing (continued)
• If breathing, assess breathing adequacy:
Effort of breathing: nasal flaring, retractions, grunting
Abnormal sounds: stridor, crowing
© 2011 National Safety Council 21-22
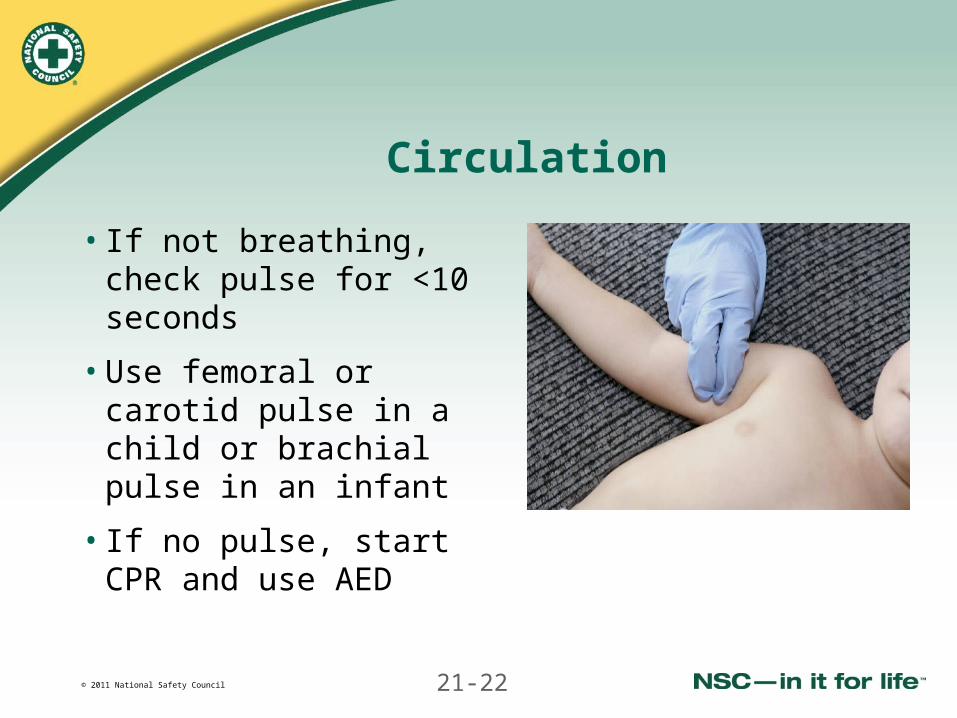
Circulation
• If not breathing, check pulse for <10 seconds
• Use femoral or carotid pulse in a child or brachial pulse in an infant
• If no pulse, start CPR and use AED
© 2011 National Safety Council 21-23
Circulation (continued)
• Assess pulse rate and strength
• Assess skin color, temperature and condition
• Reduced circulation indicated by:
- Pale, ashen or cyanotic skin color
- Cool, clammy skin
- Capillary refill time ≥2 seconds
• Begin CPR if the pulse is less than 60 beats/minute
• Assess for signs of shock and treat
© 2011 National Safety Council 21-24
Check for Severe Bleeding
• Decompensation can occur quickly in an infant or child with blood loss
• Control external bleeding immediately with direct pressure
© 2011 National Safety Council 21-25
History
• Communicate at level with child
• Gather SAMPLE information from caretakers
• Pay particular attention to signs and symptoms and their duration:
- Fever
- Activity level
- Recent eating and drinking and urine output
- Vomiting, diarrhea or abdominal pain
© 2011 National Safety Council 21-26
Vital Signs
• Vital signs of infants and children are normally different from adults
• Changes may occur quickly in infants and children, especially with decompensation
• Falling blood pressure is a late sign of shock
© 2011 National Safety Council 21-27
Normal Vital Signs
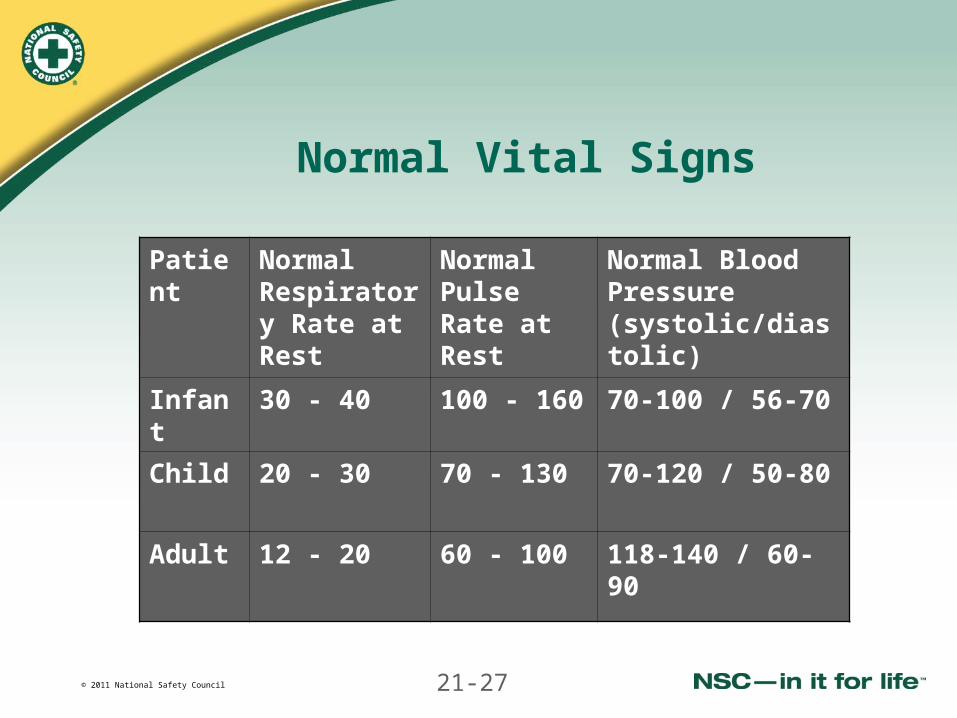
Patient Normal Respiratory Rate at Rest
Normal Pulse Rate at Rest
Normal Blood Pressure (systolic/diastolic)
Infant 30 - 40 100 - 160 70-100 / 56-70
Child 20 - 30 70 - 130 70-120 / 50-80
Adult 12 - 20 60 - 100 118-140 / 60-90
© 2011 National Safety Council 21-28
Physical Examination
• Maintain spinal immobilization in trauma or unresponsive patient
• Support head when moving infant
• Expose skin to look for injuries, but promptly cover child to prevent hypothermia; cover infant’s head
• Assess anterior fontanel on top of skull
• Examine from toe to head
© 2011 National Safety Council 21-29
Physical Examination (continued)
Especially assess:
• The head for bruising or swelling
• The ears for drainage suggestive of trauma or infection
• The mouth for loose teeth, identifiable odors and bleeding
• The neck for abnormal bruising
• The chest and back for bruise, injuries and rashes
• Extremities for deformities, swelling and pain on movement
© 2011 National Safety Council 21-30
Airway Management
• Opening airway
• Suctioning
• Using airway adjuncts
© 2011 National Safety Council 21-31
Opening the Airway of Pediatric Patients
• Be careful not to hyperextend neck when using head tiltchin lift to open airway of infant
• Put folded towel under back and shoulders for better positioning of airway
• Look inside mouth of an unresponsive infant for obstructing object
• Use jaw thrust technique for trauma patients
• Suction airway if needed
© 2011 National Safety Council 21-32
Suctioning
• Using gauze pad sweep mouth or suction
• Don’t insert tip of rigid catheter deeper than baseof tongue
• For newborn, don’t suction longer than 3-5 seconds at a time
• With an older infant or child, don’t suction longer than 10 seconds at a time
© 2011 National Safety Council 21-33
Airway Adjuncts
• Use oral airway if no gag reflex
• Remove airway if child gags, coughs, etc.
• Oral airway not for initial ventilations
• Device keeps airway open
• Select proper size
• Nasal airways are not usually inserted in children by EMRs
© 2011 National Safety Council 21-34
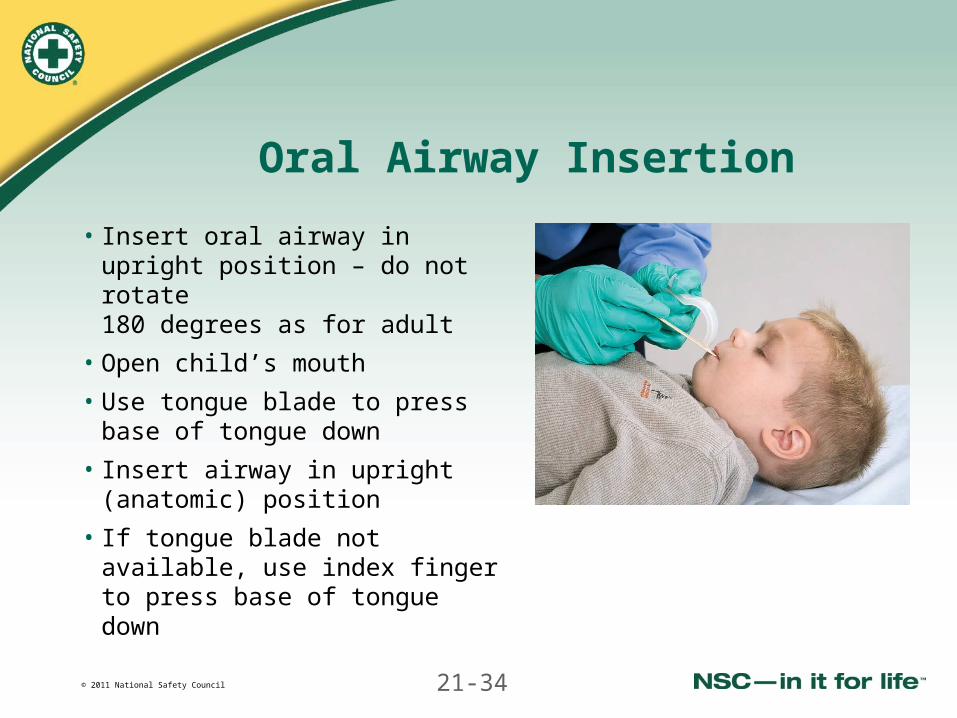
Oral Airway Insertion
• Insert oral airway in upright position – do not rotate 180 degrees as for adult
• Open child’s mouth
• Use tongue blade to press base of tongue down
• Insert airway in upright (anatomic) position
• If tongue blade not available, use index finger to press base of tongue down
© 2011 National Safety Council 21-35
Respiratory Emergencies
© 2011 National Safety Council 21-36
Respiratory Emergencies
• Airway obstructions
• Respiratory distress and arrest
• Respiratory infections
• Asthma
© 2011 National Safety Council 21-37
Signs and Symptoms of Mild Airway Obstructions
• Infant or child is alert and sitting
• Hear stridor, crowing, noisy breathing
• Retractions on inspiration
• Skin pink with good peripheral perfusion
• Strong pulse
© 2011 National Safety Council 21-38
Emergency Care for Mild Airway Obstructions
• Allow child to assume position of comfort
• Assist a younger child to sit up, not lie down
• Do not agitate child
• Encourage continued coughing to dislodge object
• Follow local protocol for oxygen administration
© 2011 National Safety Council 21-39
Signs and Symptoms of Severe Airway Obstructions
• No crying or speaking
• Weak and ineffective cough
• Cyanosis
• Cough that becomes ineffective
• Increased respiratory difficulty and stridor
• Altered mental status; unresponsiveness
© 2011 National Safety Council 21-40
Emergency Care for Severe Airway Obstructions
• Attempt to clear airway (finger sweep and suctioning)
• Use alternating back blows (slaps) and chest compressions in responsive infant
• Use abdominal thrusts in responsive child
• Give CPR to unresponsive infant or child
© 2011 National Safety Council 21-41
Emergency Care for Severe Airway Obstructions (continued)
• Check for object in mouth before giving a breath
• Remove any object you see
• Never perform blind finger sweep
• Attempt artificial ventilations with mouth-to-mask technique
© 2011 National Safety Council 21-42
Respiratory Distress and Arrest
• Respiratory distress is difficulty breathing
• Respiratory distress frequently leads to respiratory arrest
© 2011 National Safety Council 21-43
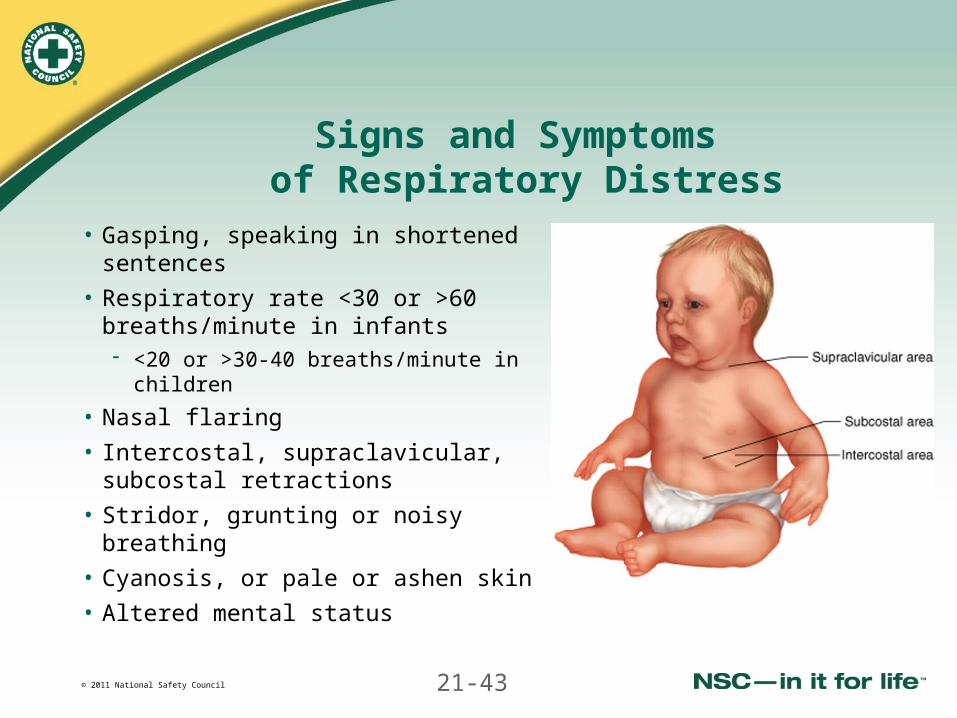
Signs and Symptoms of Respiratory Distress
• Gasping, speaking in shortened sentences
• Respiratory rate <30 or >60 breaths/minute in infants <20 or >30-40 breaths/minute in
children
• Nasal flaring
• Intercostal, supraclavicular, subcostal retractions
• Stridor, grunting or noisy breathing
• Cyanosis, or pale or ashen skin
• Altered mental status
© 2011 National Safety Council 21-44
Emergency Care for Respiratory Distress
• Perform standard patient care
• Allow child to assume position of comfort
• Ensure appropriate position of head and neck
• Follow local protocol for oxygen administration
© 2011 National Safety Council 21-45
Blow-by Oxygen
• Responsive infant or child may resist mask on face
• Use blow-by oxygen delivery technique
• Have caretaker hold mask about 2 inches from face
© 2011 National Safety Council 21-46
Signs and Symptoms of Respiratory Arrest
• Breathing rate:
- <20 breaths/minute in an infant
- <10 breaths/minute in a child
• Limp muscle tone
• Unresponsiveness
• Slow or absent pulse
• Weak or absent distal pulses
• Cyanosis
© 2011 National Safety Council 21-47
Emergency Care forRespiratory Arrest
• Perform standard patient care
• Provide ventilations by mouth or mask
• Follow local protocol for oxygen administration
• Monitor pulse and provide CPR if needed
© 2011 National Safety Council 21-48
Respiratory Infections
• Common in childhood
• Range from minor to life threatening
• May affect upper or lower airways
• Result from infection, foreign bodies, allergic conditions
© 2011 National Safety Council 21-49
Signs and Symptoms of Respiratory Problems
• Rapid breathing
• Noisy breathing
• Retractions
• Mental status changes
© 2011 National Safety Council 21-50
Croup
• Viral infection of upper/lower airway
• More frequently occurs in winter months and in evening
• More common in younger children
• Often preceded by being ill 1-2 days with or without fever
• Generally not life-threatening
© 2011 National Safety Council 21-51
Signs and Symptoms of Croup
• Hoarseness
• Stridor
• “Barking” cough
• Difficulty breathing
© 2011 National Safety Council 21-52
Emergency Care for Croup
• Perform standard patient care
• Difficult to distinguish from life-threatening epiglottitis
• If croup persistent, child should see physician
• Give care for respiratory distress
• Follow local protocol for humidified oxygen
© 2011 National Safety Council 21-53
Epiglottitis
• Rare, life-threatening infection of epiglottis
• Epiglottis swells and airway completely obstructed
• Occurs more frequently in children older than 4
© 2011 National Safety Council 21-54
Signs and Symptomsof Epiglottitis
• Child appears ill and frightened
• High fever
• Child is sitting up to breathe
• Saliva may drool from the child’s mouth
© 2011 National Safety Council 21-55
Emergency Care for Epiglottitis
• Perform standard patient care
• Don’t examine mouth or place OPA
• Allow child to remain in comfortable position
• Give care for respiratory distress
• Follow local protocol for oxygen administration
• Ensure immediate transport
© 2011 National Safety Council 21-56
Bronchiolitis
• Common cause of respiratory distress in young children
• Also called respiratory syncytial virus
• Viral infection of smaller airways causing respiratory distress and occasional hypoxia
© 2011 National Safety Council 21-57
Signs and Symptoms of Bronchiolitis
• Fever
• Nasal congestion
• Increased work of breathing with retractions and use of accessory muscles
• Markedly abnormal lung sounds with crackles and wheezes together
• May be cyanotic
© 2011 National Safety Council 21-58
Emergency Care for Bronchiolitis
• Perform standard patient care
• Give care for respiratory distress
• Follow local protocol for humidified oxygen
• If patient has asthma medication inhaler, follow local protocol
© 2011 National Safety Council 21-59
Asthma
• Common medical problem in children
• Causes periodic attacks of difficulty breathing
• Results from an abnormal spasm of lower airways
• Attacks range from minor to life threatening
© 2011 National Safety Council 21-60
Signs and Symptoms of Asthma Attack
• Difficulty breathing, rapid irregular breathing
• Coughing, wheezing
• Exhaustion
• In severe attack:
- Altered mental status
- Cyanosis
© 2011 National Safety Council 21-61
Emergency Care for Asthma Attack
• Perform standard patient care
• Give care for respiratory distress
• Follow local protocol for humidified oxygen
• If patient has asthma medication inhaler, follow local protocol to assist
© 2011 National Safety Council 21-62
Shock
© 2011 National Safety Council 21-63
Shock
• Commonly occurs from bleeding, traumatic injury, and fluid loss from prolonged vomiting or diarrhea
• May occur rapidly in infants and quickly become life-threatening
• May be delayed in children who then suddenly decompensate
• Common cause of cardiac arrest in infants and children
© 2011 National Safety Council 21-64
Signs and Symptoms of Shock
• Rapid (early) or slow (late) weak pulse or absent pulse
• Unequal central and peripheral pulses
• Poor skin perfusion, delayed capillary refill
• Cool, clammy, pale skin
• Rapid respiratory rate (early shock)
• Altered mental status
© 2011 National Safety Council 21-65
Emergency Care for Shock
• Perform standard patient care
• Control any bleeding
• Follow local protocol for oxygen administration
• Monitor pulse carefully and provide CPR if needed
• Raise legs if spinal or traumatic injury is not suspected
• Keep patient warm but not overheated
• Monitor vital signs frequently while awaiting EMS
© 2011 National Safety Council 21-66
Seizures
© 2011 National Safety Council 21-67
Causes of Seizures
• High fever
• Epilepsy
• Infections
• Head injuries
• Poisoning
• Low oxygen levels
• Low blood sugar
• Other causes
© 2011 National Safety Council 21-68
Seizures
• Potentially life-threatening
• You don’t need to know cause to give care
• Febrile seizures common in children <5 years
• Most will be over by the time you arrive at scene
• After a seizure (except a febrile seizure), child appears sleepy and confused

© 2011 National Safety Council 21-69
Assessing Seizures
• Perform standard assessment
• Assess for injuries that may occur
• Gather the history from caretakers:
- Has child had prior seizure(s)?
- Is this child’s usual seizure pattern? How long did it last?
- Does child take seizure medication?
- Could child have ingested any other medication or potential toxins?
© 2011 National Safety Council 21-70
Signs and Symptoms of Seizures
• Altered mental status
• Muscle twitching, convulsions, rigid extremities
• May be brief or prolonged
• Loss of bowel and bladder control
© 2011 National Safety Council 21-71
Emergency Care for Seizures
• Perform standard patient care
• Place patient on floor and protect patient from environment
• Loosen any constricting clothing, remove eyeglasses
• Ask bystanders (except caretakers) to leave
• Ensure airway remains open
• Never restrain patient
• Don’t put anything in mouth
© 2011 National Safety Council 21-72
Emergency Care for Seizures(continued)
• If patient is bluish, ensure airway is open and give ventilations
• After seizure, place an unresponsive patient in recovery position
• Be prepared to suction to maintain airway
• Follow local protocol for oxygen administration
• Report assessment findings to additional EMS personnel
© 2011 National Safety Council 21-73
Altered Mental Status
© 2011 National Safety Council 21-74
Causes of Altered Mental Status
• Low blood sugar
• Poisoning
• Seizures
• Infection
• Head trauma
• Any condition that causes decreased oxygen levels
© 2011 National Safety Council 21-75
Assessing Altered Mental Status
• Perform standard assessment
• Ask caretakers about any history of diabetes, seizures or recent trauma
• Monitor patient’s vital signs
© 2011 National Safety Council 21-76
Signs and Symptoms of Altered Mental Status in an Infant or Child
• Drowsiness
• Confusion, agitation
• Behavior described as unusual by caretakers
© 2011 National Safety Council 21-77
Emergency Care for Altered Mental Status
• Perform standard patient care
• Place unresponsive patient in recovery position (if no trauma suspected)
• Follow local protocol for oxygen administration
© 2011 National Safety Council 21-78
Sudden Infant Death Syndrome
© 2011 National Safety Council 21-79
Sudden Infant Death Syndrome
• Sudden Infant Death Syndrome (SIDS) is the unexpected, sudden death of a normal, healthy infant during sleep
• Causes not well understood
• Leading cause of death between 1 week and 1 year of age in United States
• Peak incidence occurs at 2-4 months of age
© 2011 National Safety Council 21-80
Sudden Infant Death Syndrome(continued)
• More common during winter months and in males
• Not due to external suffocation from blankets or pillows
• Not related to child abuse or vomiting and aspiration of stomach contents

© 2011 National Safety Council 21-81
Assessing SIDS
• Perform standard assessment• Complete primary assessment and care for life-threatening
conditions• If infant is still alive, take history and perform secondary
assessment • In addition, ask caretakers about circumstances:
- When was infant put to bed?- When was infant last seen?- What position was infant in when found? - How did infant look when found?- Was there anything unusual in environment?- Infant’s general health recently?
© 2011 National Safety Council 21-82
Signs and Symptoms of SIDS
• Cardiac and respiratory arrest
• Skin cyanotic or mottled
• Most commonly discovered in early morning
© 2011 National Safety Council 21-83
Emergency Care for SIDS
• Perform standard patient care
• Take body substance isolation precautions
• Try to resuscitate infant unless the body is stiff
• Lividity is normal, not sign of abuse
• Comfort, calm and reassure caretakers
• Avoid any comments that might suggest blame to caretakers

© 2011 National Safety Council 21-84
Trauma
© 2011 National Safety Council 21-85
Trauma
• Common emergency in childhood
• Leading cause of death in children
• Blunt trauma causes the most injuries
• Pattern of injury may be different from that in adults
© 2011 National Safety Council 21-86
Common Causes of Trauma
• Motor vehicle crashes
- Unrestrained infants and children have head/neck injuries
- Restrained infants and children have abdominal and lower spine injuries
- Infant and booster seats often improperly fastened
© 2011 National Safety Council 21-87
Common Causes of Trauma(continued)
• Being struck by a vehicle while riding a bicycle
• Being struck by a vehicle while walking
• Falls from a height or diving into shallow water
• Burns
• Sports injuries to head and neck
• Child abuse and neglect
© 2011 National Safety Council 21-88
Common Types of Injury
• Anatomical differences make certain types of injury more likely
• Head injuries
• Abdominal injuries
• Extremity injuries
• Burns
© 2011 National Safety Council 21-89
Assessing Trauma
• Perform standard assessment
• Examine responsive child from toe to head
• Suspect certain types of injuries based on MOI
• Smaller amounts of blood loss can result in shock; signs of shock may occur later
© 2011 National Safety Council 21-90
Emergency Care for Trauma
• Perform standard patient care
• Use jaw thrust to open airway
- Use head tilt–chin lift if unsuccessful
• Suction airway as needed
• Manually stabilize head and neck
© 2011 National Safety Council 21-91
Emergency Care for Trauma (continued)
• Manually stabilize extremity injuries
• Treat shock
• Maintain normal body temperature (hypothermia more likely in shock in children)
• Follow local protocol for oxygen administration
• Ensure transport as soon as possible
© 2011 National Safety Council 21-92
Child Abuse and Neglect
© 2011 National Safety Council 21-93
Suspected Child Abuse and Neglect
• Abuse: an intentional improper and excessive action injuring or causing harm
• May include psychological or emotional abuse and sexual abuse
• Neglect: failing to provide basic needs
© 2011 National Safety Council 21-94
Who is Abused?
• Any child, although some are more likely to be abused
• Child abuser can come from any geographic, religious, ethnic, occupational, educational or socioeconomic group
• Abuser is usually a caretaker or someone in role of parent
• Most abusers of children were themselves abused as children
© 2011 National Safety Council 21-95
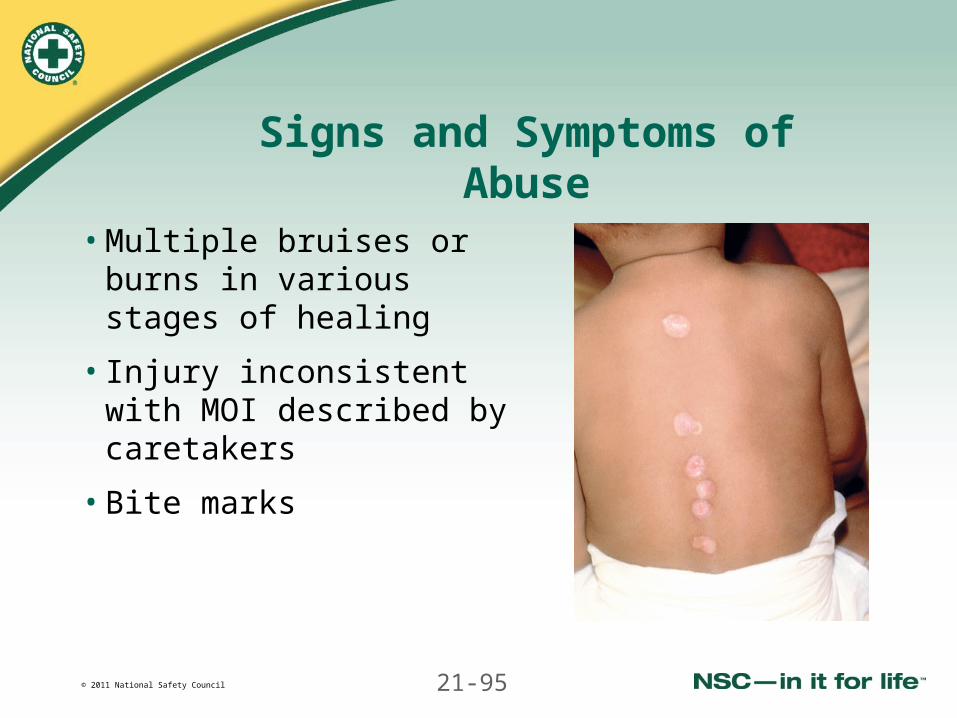
Signs and Symptoms of Abuse
• Multiple bruises or burns in various stages of healing
• Injury inconsistent with MOI described by caretakers
• Bite marks
© 2011 National Safety Council 21-96
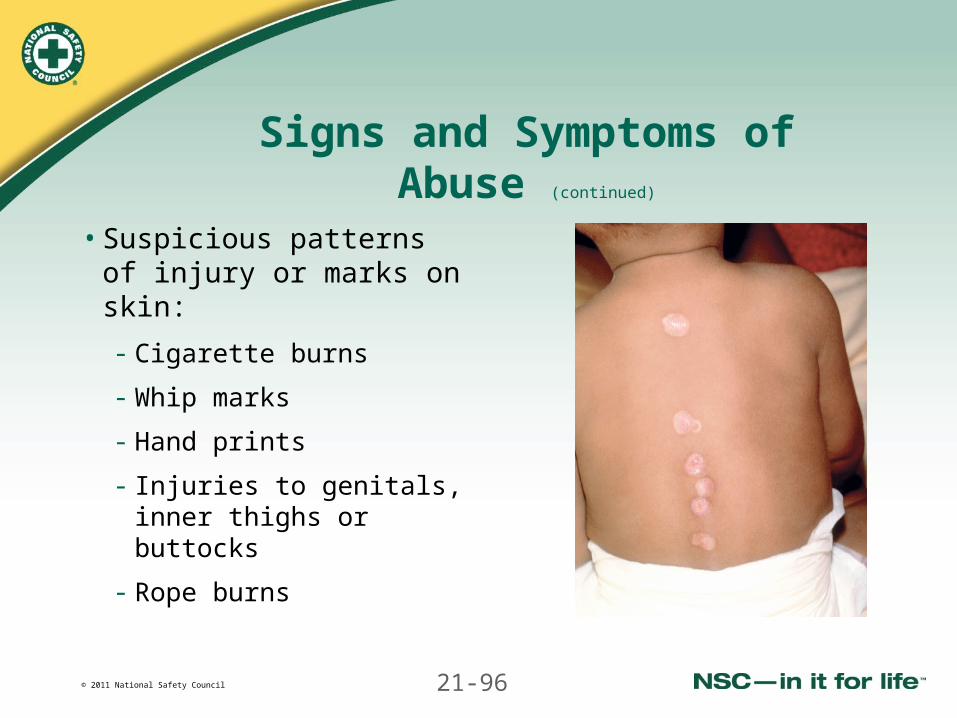
Signs and Symptoms of Abuse (continued)
• Suspicious patterns of injury or marks on skin:
- Cigarette burns
- Whip marks
- Hand prints
- Injuries to genitals, inner thighs or buttocks
- Rope burns
© 2011 National Safety Council 21-97
Signs and Symptoms of Abuse(continued)
• Repeated calls to same address
• Unusual burns
- Scalding
- A glove or dip pattern
- Burns inconsistent with history presented
- Untreated burns
• Caretakers inappropriately unconcerned
• Caretakers with uncontrollable anger
© 2011 National Safety Council 21-98
Signs and Symptoms of Abuse(continued)
• Conflicting stories
• Child fearful to discuss how injury occurred
• Child’s obvious fear of caretaker
• Obvious or suspected fractures in child younger than 2
• More injuries than are usually seen at same age
• Injuries scattered on many areas of the body
© 2011 National Safety Council 21-99
Signs and Symptoms of Neglect
• Lack of adult supervision
• Child appears malnourished
• Clothing inappropriate for environment
• Unsafe living environment
• Signs of drug or alcohol abuse
• Untreated chronic illness (asthmatic with no medications)
• Untreated soft-tissue injuries
• Delayed call for help
© 2011 National Safety Council 21-100
Assessing Suspected Abuse or Neglect
• Perform standard assessment
• Obtain as much information as possible
• Document all information on patient report
© 2011 National Safety Council 21-101
Emergency Care When Abuse is Suspected
• Perform standard patient care
• Don’t accuse caretakers in the field
• Treat patient’s injuries appropriately
• Protect child from further abuse, if necessary
• Report objective information to EMS unit
© 2011 National Safety Council 21-102
Emergency Care When Abuse is Suspected (continued)
• Save evidence of physical or sexual abuse
• File a report as required by state law and local protocol:
- Remain objective
- Report what you see and hear
- Do not comment on what you think
• Maintain confidentiality about the call
© 2011 National Safety Council 21-103
Shaken Baby Syndrome
• Pattern of injury resulting when caretaker shakes infant
• Also occurs in young children
• Infant may have severe internal injuries, including brain or spinal injuries
• Infant may be unresponsive or experiencing seizures
© 2011 National Safety Council 21-104
Emergency Care forShaken Baby Syndrome
• Perform standard patient care
• Manually stabilize the head and neck
• Follow local protocol for oxygen administration
• Ensure transport as soon as possible
© 2011 National Safety Council 21-105
Emergency Medical Responder Stress
• Death or serious injury can cause strong emotional reactions and stress
• Stress is likely in instances of serious child abuse or neglect
• Providing care while family members or caretakers are very emotional is stressful
© 2011 National Safety Council 21-106
Emergency Medical Responder Stress (continued)
• Don’t react personally to others’ emotions or behavior
• Realize that many patients may die regardless of care provided
• Talk with family and friends
• Seek professional help
• CISM programs are available
Related Documents











