© 2004 Current Medicine Group Ltd FISIOLOGIA DIGESTIVA (BCM II) FISIOLOGIA DIGESTIVA (BCM II) Clase 12: Diarrea Clase 12: Diarrea Dr. Michel Baró Aliste Dr. Michel Baró Aliste

© 2004 Current Medicine Group Ltd FISIOLOGIA DIGESTIVA (BCM II) Clase 12: Diarrea Dr. Michel Baró Aliste.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
© 2004 Current Medicine Group Ltd
FISIOLOGIA DIGESTIVA (BCM II)FISIOLOGIA DIGESTIVA (BCM II)
Clase 12: Diarrea Clase 12: Diarrea
Dr. Michel Baró AlisteDr. Michel Baró Aliste
© 2004 Current Medicine Group Ltd
DefinicionesDefiniciones
Diarrea: aumento de la frecuencia y/o volumen de las deposicionesDiarrea: aumento de la frecuencia y/o volumen de las deposiciones
Mayor a 200 g/díaMayor a 200 g/día
PseudodiarreaPseudodiarrea
IncontinenciaIncontinencia
Aguda (<2 semanas)Aguda (<2 semanas)
Crónica (>4 semanas)Crónica (>4 semanas)
© 2004 Current Medicine Group Ltd
Tipos de DiarreaTipos de Diarrea
-Osmótica (malabsortivas)-Osmótica (malabsortivas)
-Secretora (alteración de transporte de electrolitos)-Secretora (alteración de transporte de electrolitos)
-Alteración de la motilidad-Alteración de la motilidad
-Inflamatoria (disenterías)-Inflamatoria (disenterías)
© 2004 Current Medicine Group Ltd
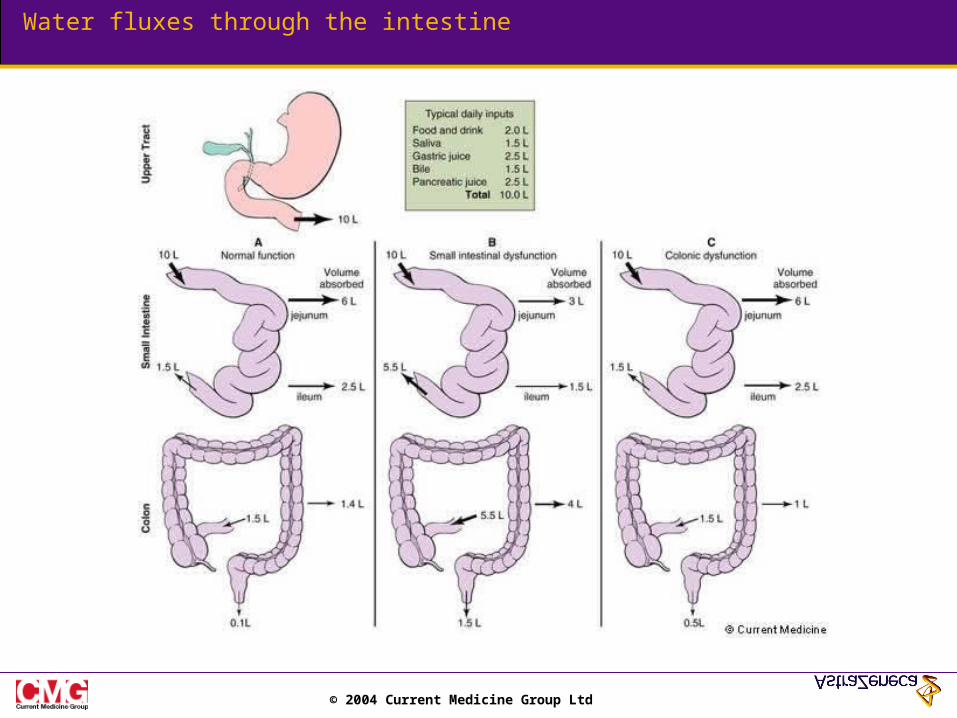
Water fluxes through the intestine
© 2004 Current Medicine Group Ltd
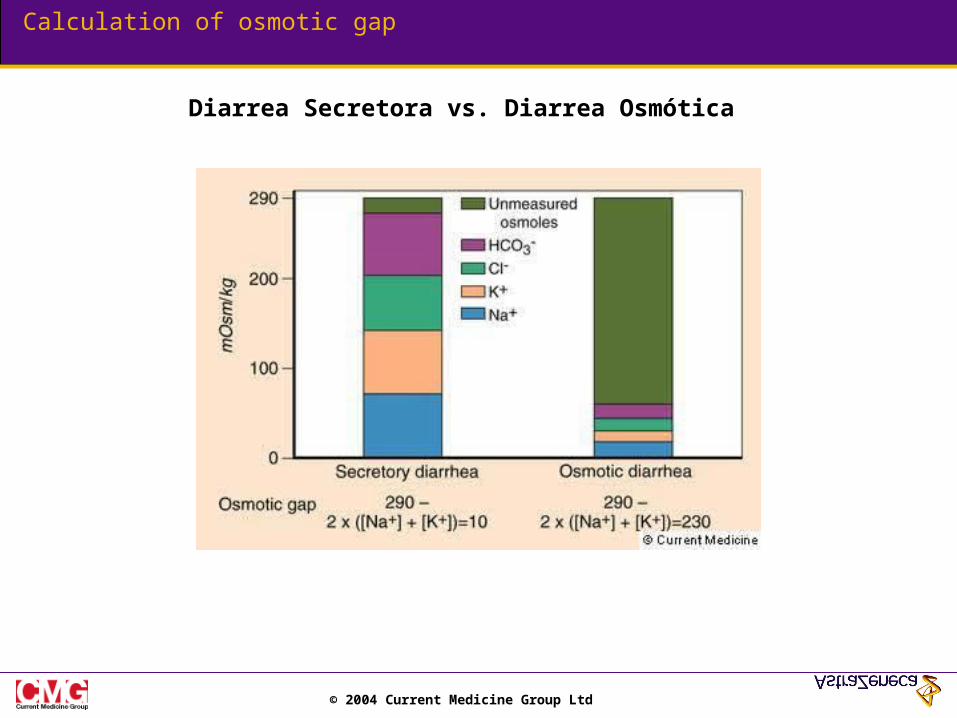
Calculation of osmotic gap
Diarrea Secretora vs. Diarrea Osmótica
© 2004 Current Medicine Group Ltd
Typical features of secretory diarrhea
TABLE 4 - 5. TYPICAL FEATURES OF SECRETORY DIARRHEA
Voluminous, watery stools
Little or no fecal osmotic gap, stool pH near 7.0
Usually persists during fasting
Usually no pus, blood, or excess fat in stools
© 2004 Current Medicine Group Ltd
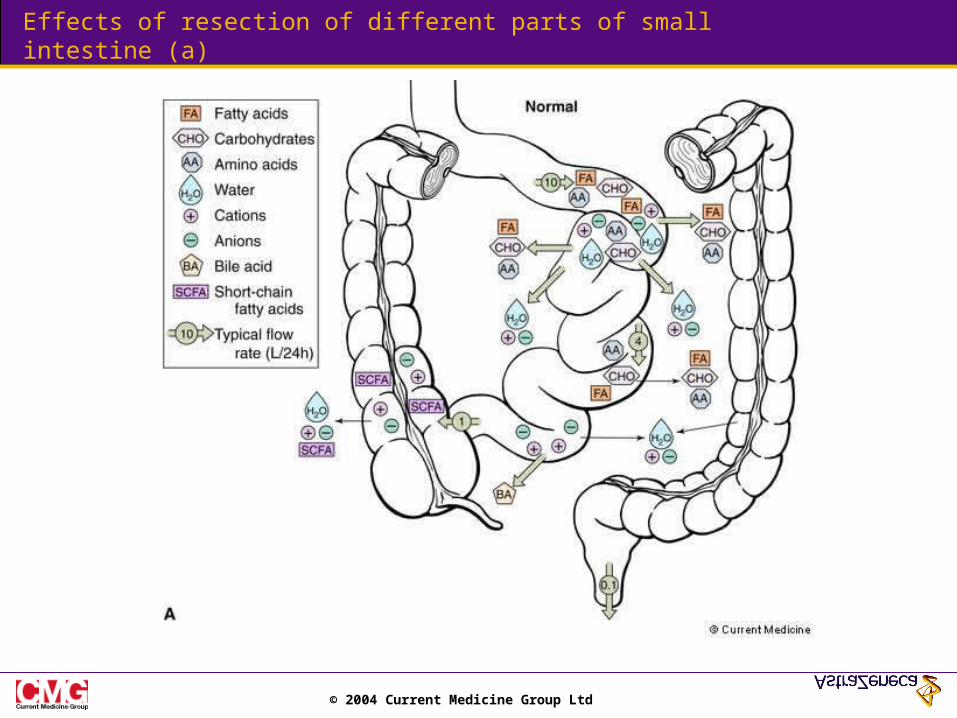
Effects of resection of different parts of small intestine (a)
© 2004 Current Medicine Group Ltd
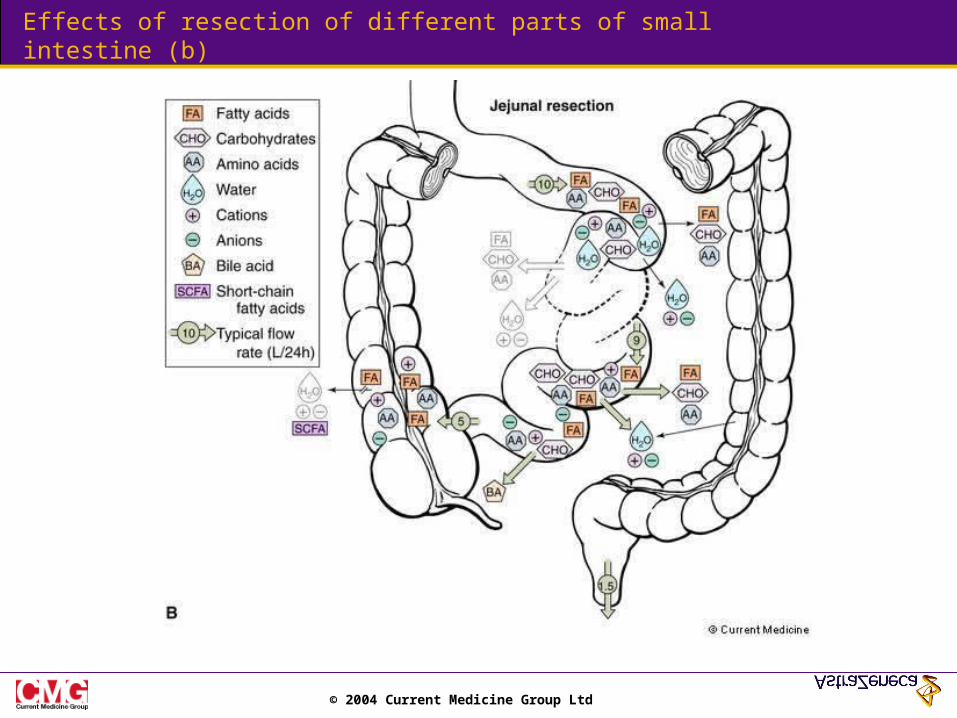
Effects of resection of different parts of small intestine (b)
© 2004 Current Medicine Group Ltd
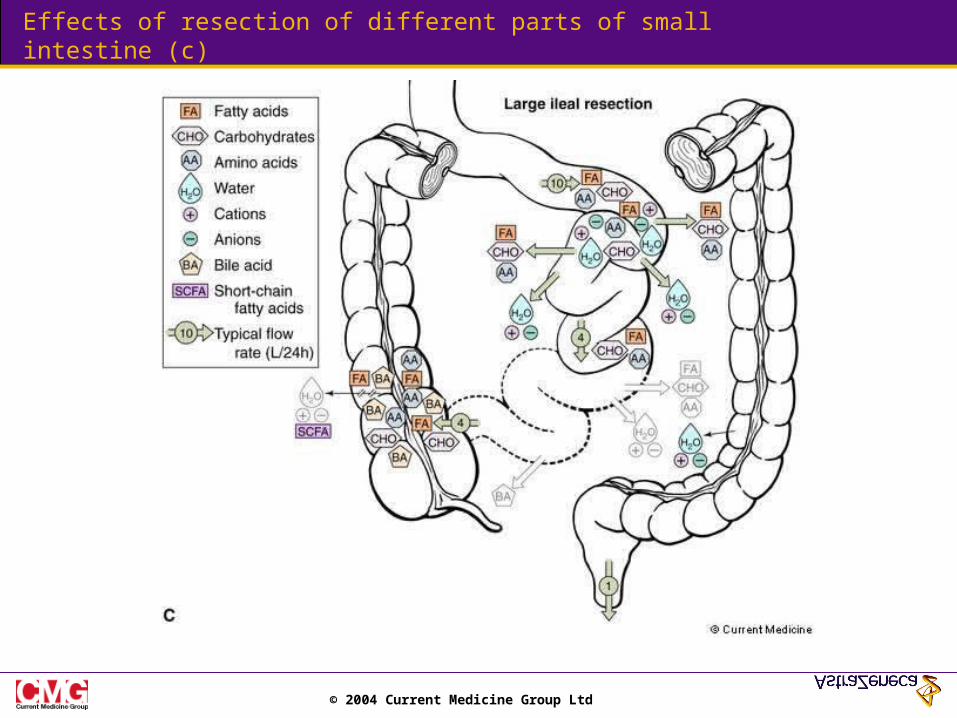
Effects of resection of different parts of small intestine (c)
© 2004 Current Medicine Group Ltd
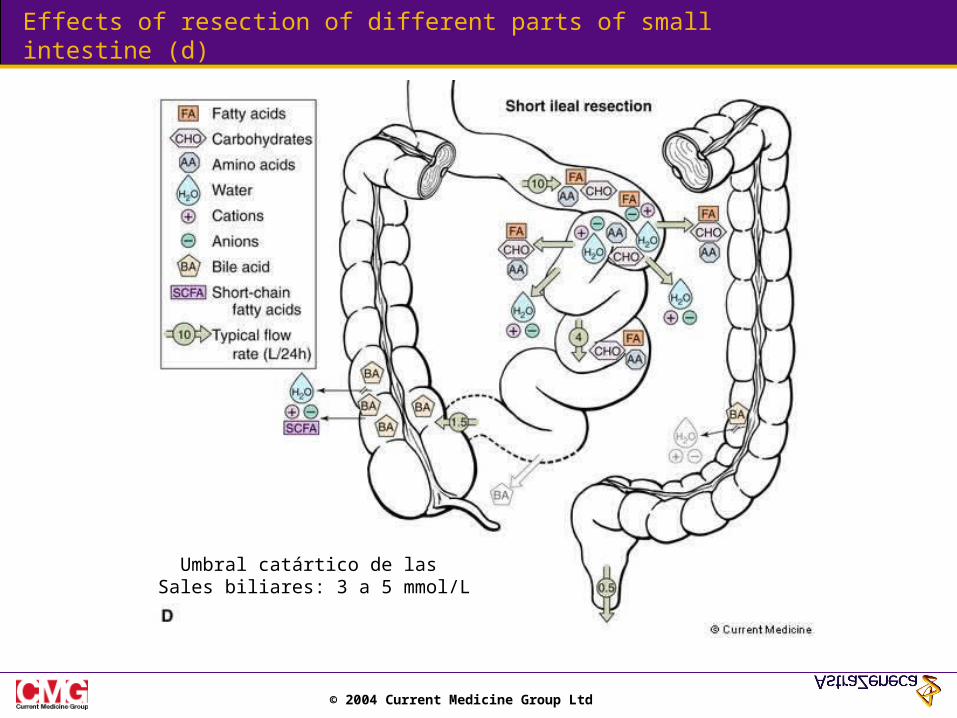
Effects of resection of different parts of small intestine (d)
Umbral catártico de las Sales biliares: 3 a 5 mmol/L
© 2004 Current Medicine Group Ltd
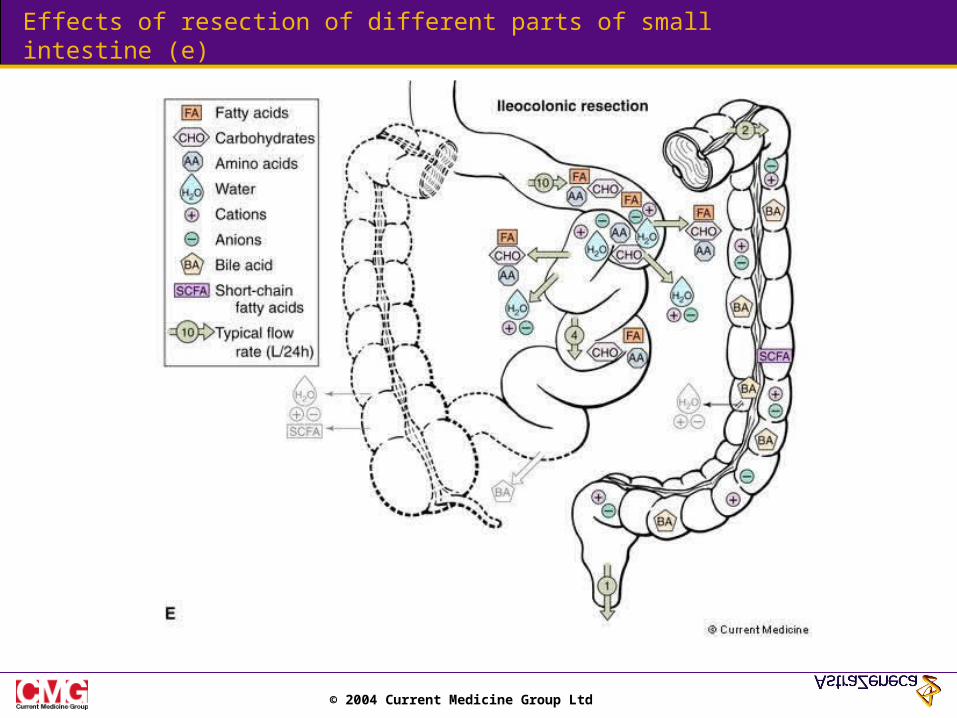
Effects of resection of different parts of small intestine (e)
© 2004 Current Medicine Group Ltd
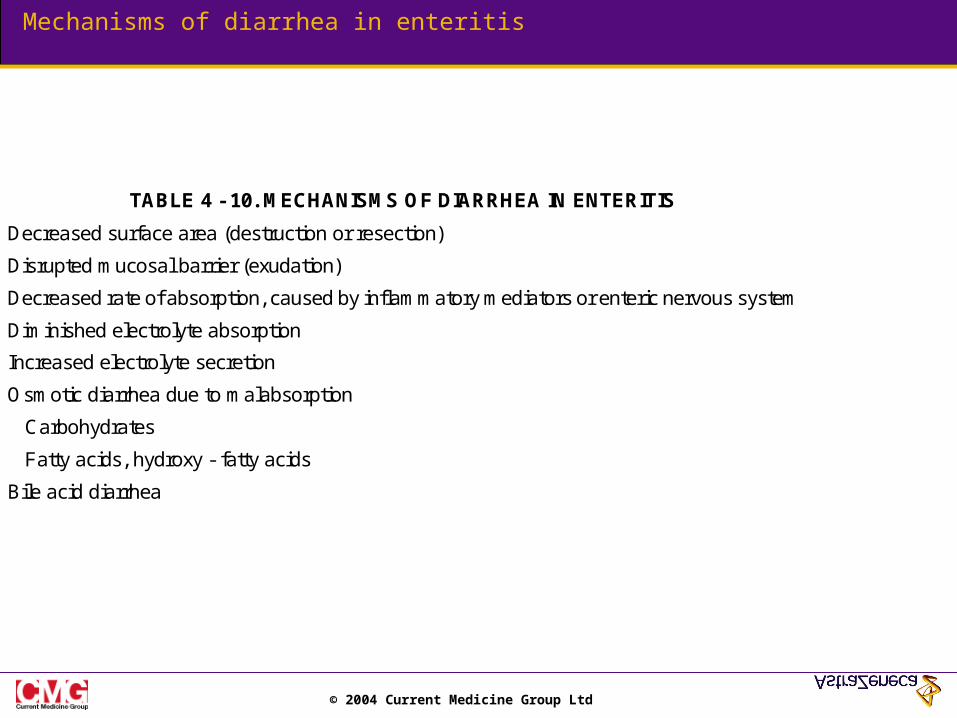
Mechanisms of diarrhea in enteritis
TABLE 4 - 10. MECHANISMS OF DIARRHEA IN ENTERITIS
Decreased surface area (destruction or resection)
Disrupted mucosal barrier (exudation)
Decreased rate of absorption, caused by inflammatory mediators or enteric nervous system
Diminished electrolyte absorption
Increased electrolyte secretion
Osmotic diarrhea due to malabsorption
Carbohydrates
Fatty acids, hydroxy - fatty acids
Bile acid diarrhea
© 2004 Current Medicine Group Ltd
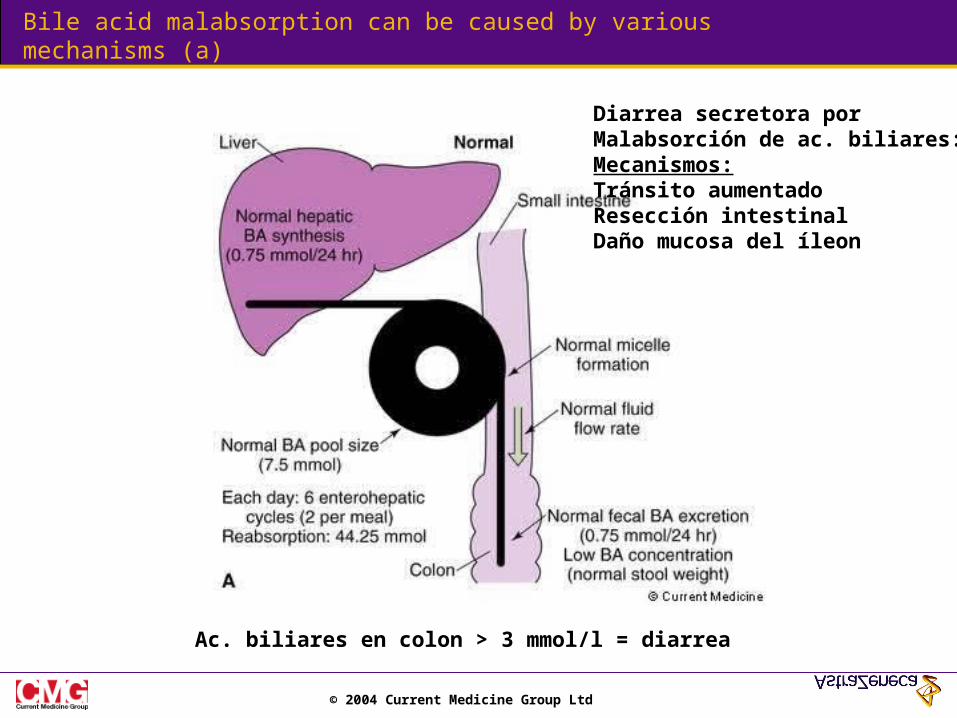
Bile acid malabsorption can be caused by various mechanisms (a)
Ac. biliares en colon > 3 mmol/l = diarrea
Diarrea secretora porMalabsorción de ac. biliares:Mecanismos:Tránsito aumentadoResección intestinalDaño mucosa del íleon
© 2004 Current Medicine Group Ltd
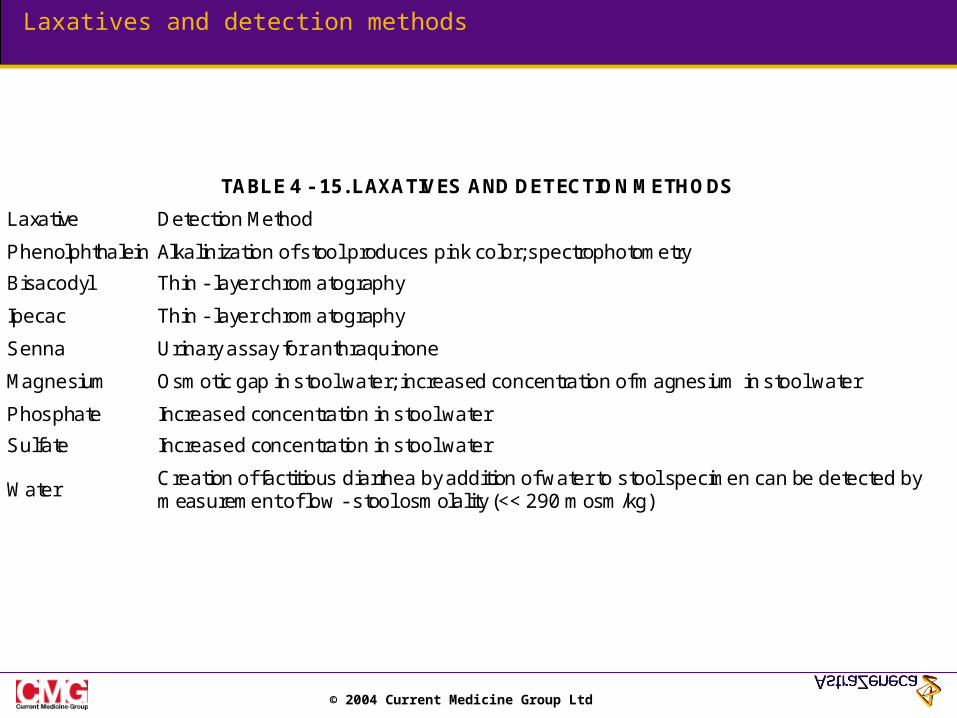
Laxatives and detection methods
TABLE 4 - 15. LAXATIVES AND DETECTION METHODS
Laxative Detection Method
Phenolphthalein Alkalinization of stool produces pink color; spectrophotometry
Bisacodyl Thin - layer chromatography
Ipecac Thin - layer chromatography
Senna Urinary assay for anthraquinone
Magnesium Osmotic gap in stool water; increased concentration of magnesium in stool water
Phosphate Increased concentration in stool water
Sulfate Increased concentration in stool water
Water Creation of factitious diarrhea by addition of water to stool specimen can be detected by measurement of low - stool osmolality (<< 290 mosm/kg)
© 2004 Current Medicine Group Ltd
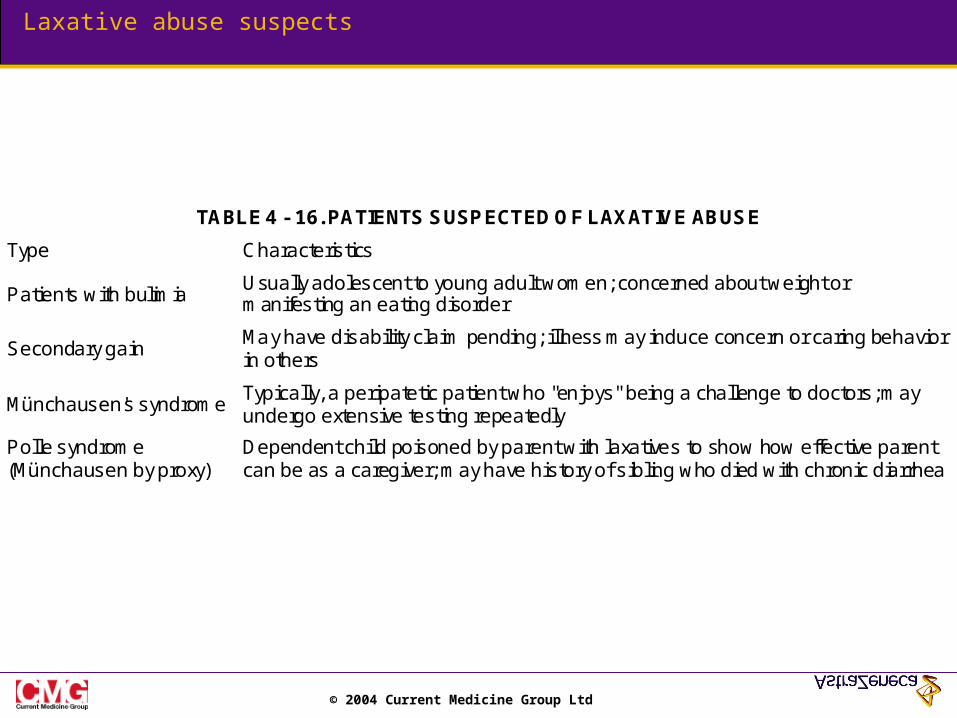
Laxative abuse suspects
TABLE 4 - 16. PATIENTS SUSPECTED OF LAXATIVE ABUSE
Type Characteristics
Patients with bulimia Usually adolescent to young adult women; concerned about weight or manifesting an eating disorder
Secondary gain May have disability claim pending; illness may induce concern or caring behavior in others
Münchausen's syndrome Typically, a peripatetic patient who "enjoys" being a challenge to doctors; may undergo extensive testing repeatedly
Polle syndrome (Münchausen by proxy)
Dependent child poisoned by parent with laxatives to show how effective parent can be as a caregiver; may have history of sibling who died with chronic diarrhea
© 2004 Current Medicine Group Ltd
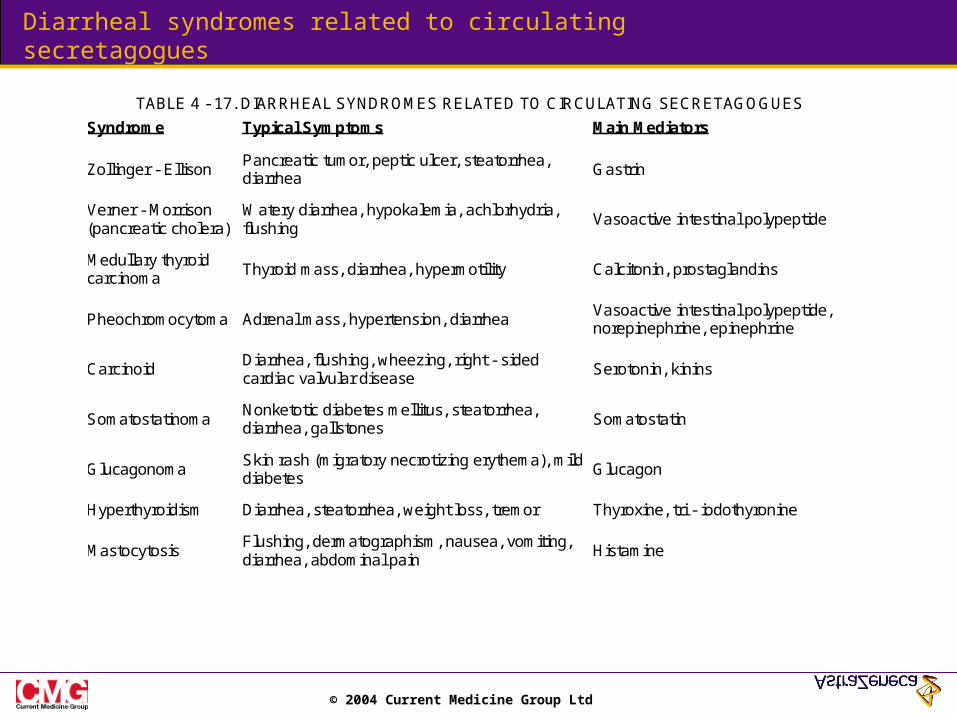
Diarrheal syndromes related to circulating secretagogues
TABLE 4 - 17. DIARRHEAL SYNDROMES RELATED TO CIRCULATING SECRETAGOGUES
Syndrome Typical Symptoms Main Mediators
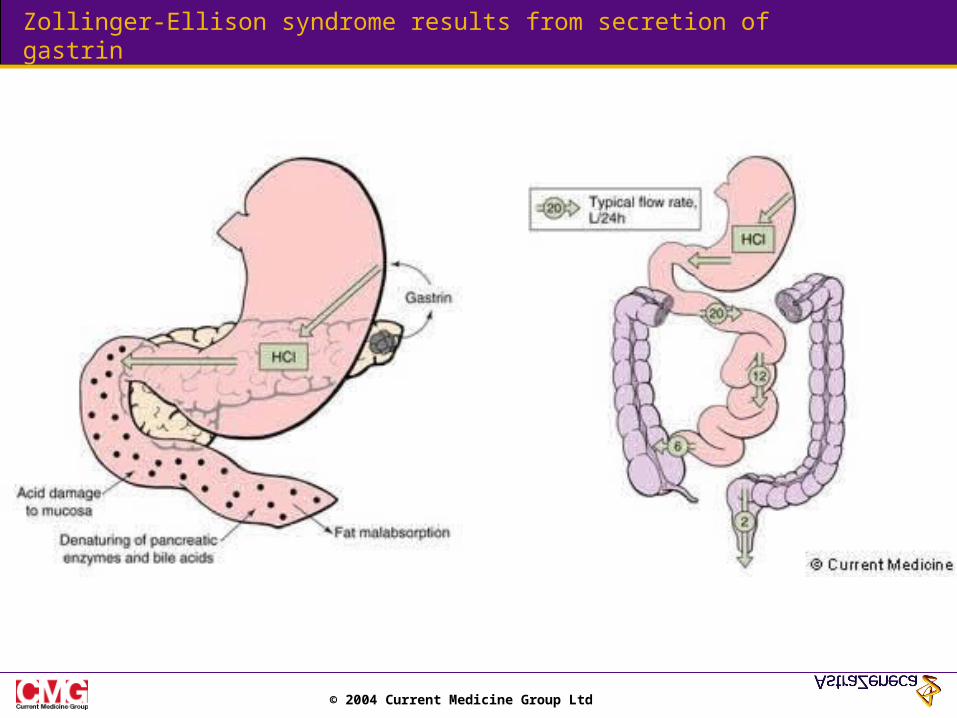
Zollinger - Ellison Pancreatic tumor, peptic ulcer, steatorrhea, diarrhea
Gastrin
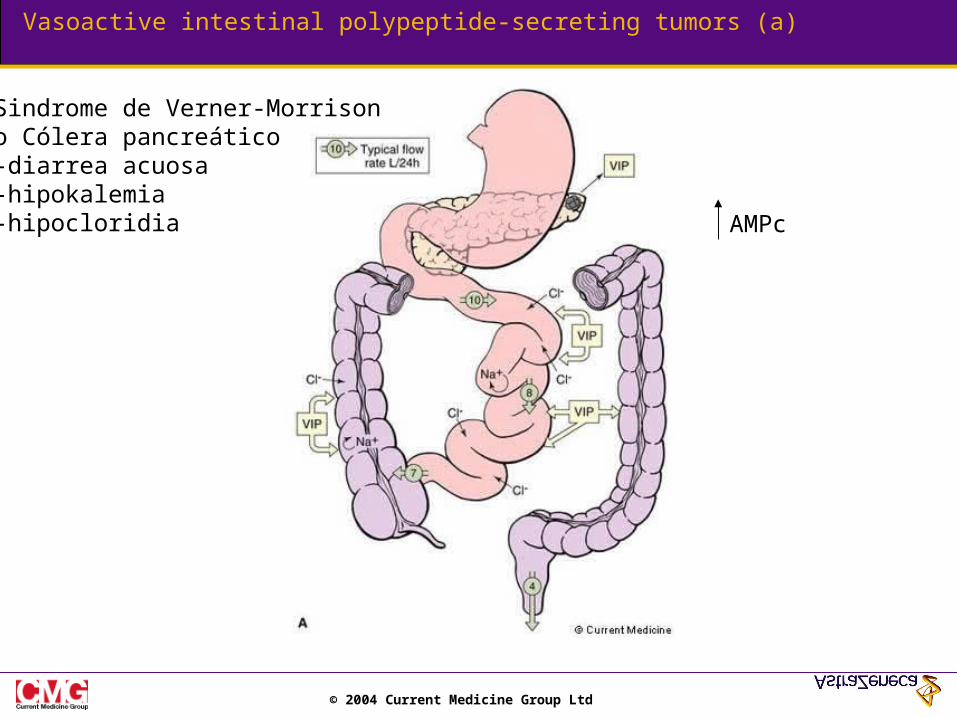
Verner - Morrison (pancreatic cholera)
Watery diarrhea, hypokalemia, achlorhydria, flushing
Vasoactive intestinal polypeptide
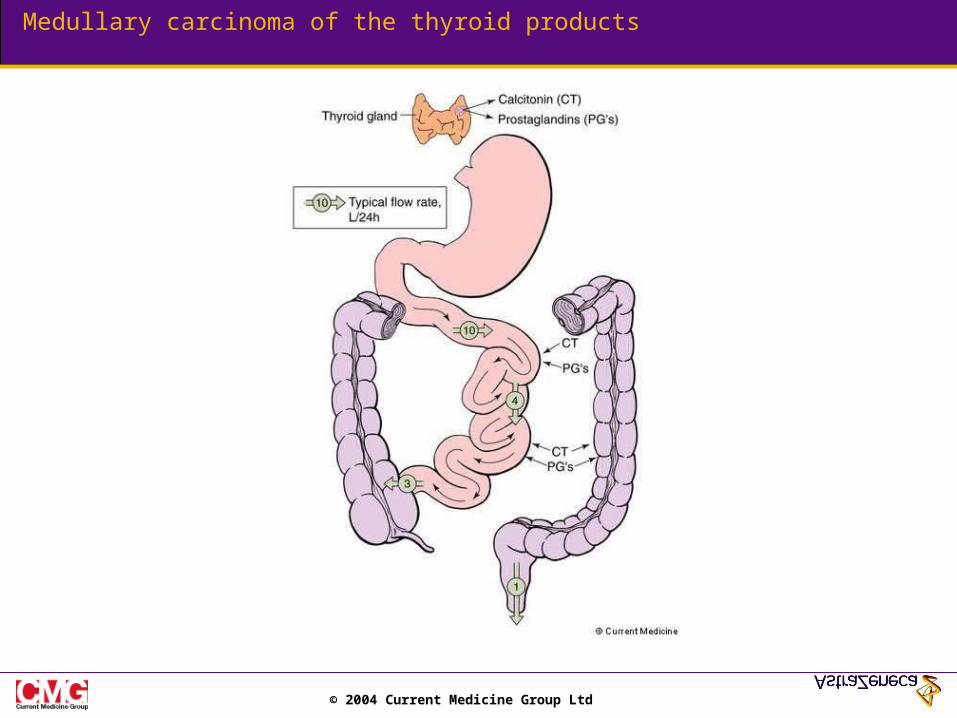
Medullary thyroid carcinoma
Thyroid mass, diarrhea, hypermotility Calcitonin, prostaglandins
Pheochromocytoma Adrenal mass, hypertension, diarrhea Vasoactive intestinal polypeptide, norepinephrine, epinephrine
Carcinoid Diarrhea, flushing, wheezing, right - sided cardiac valvular disease
Serotonin, kinins
Somatostatinoma Nonketotic diabetes mellitus, steatorrhea, diarrhea, gallstones
Somatostatin
Glucagonoma Skin rash (migratory necrotizing erythema), mild diabetes
Glucagon
Hyperthyroidism Diarrhea, steatorrhea, weight loss, tremor Thyroxine, tri - iodothyronine
Mastocytosis Flushing, dermatographism, nausea, vomiting, diarrhea, abdominal pain
Histamine
© 2004 Current Medicine Group Ltd
Zollinger-Ellison syndrome results from secretion of gastrin
© 2004 Current Medicine Group Ltd
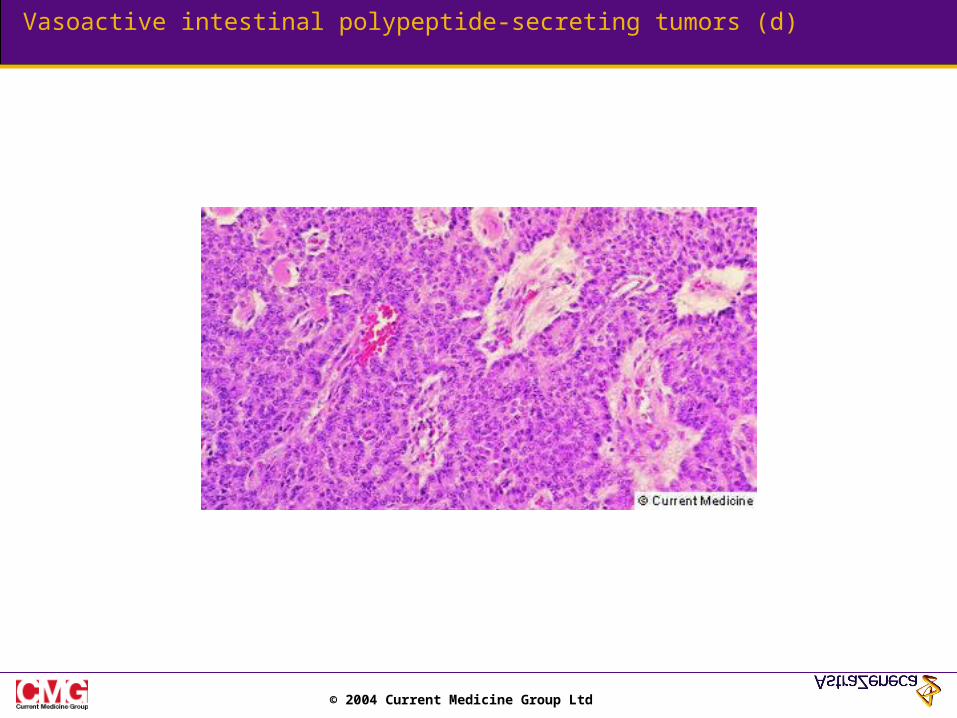
Vasoactive intestinal polypeptide-secreting tumors (a)
Sindrome de Verner-Morrisono Cólera pancreático-diarrea acuosa-hipokalemia-hipocloridia AMPc
© 2004 Current Medicine Group Ltd
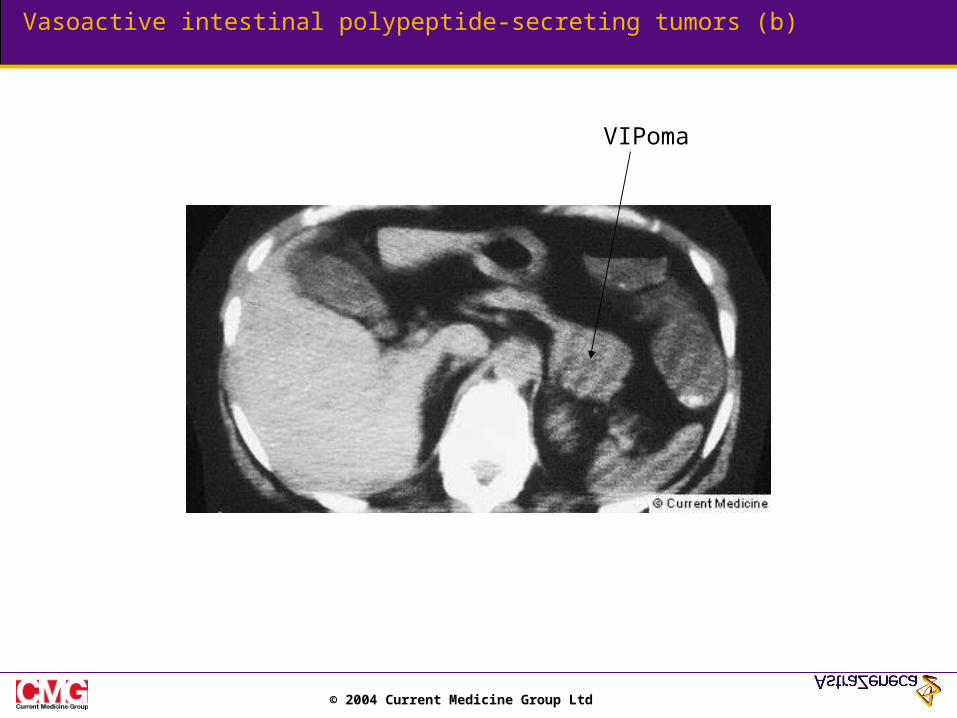
Vasoactive intestinal polypeptide-secreting tumors (b)
VIPoma
© 2004 Current Medicine Group Ltd
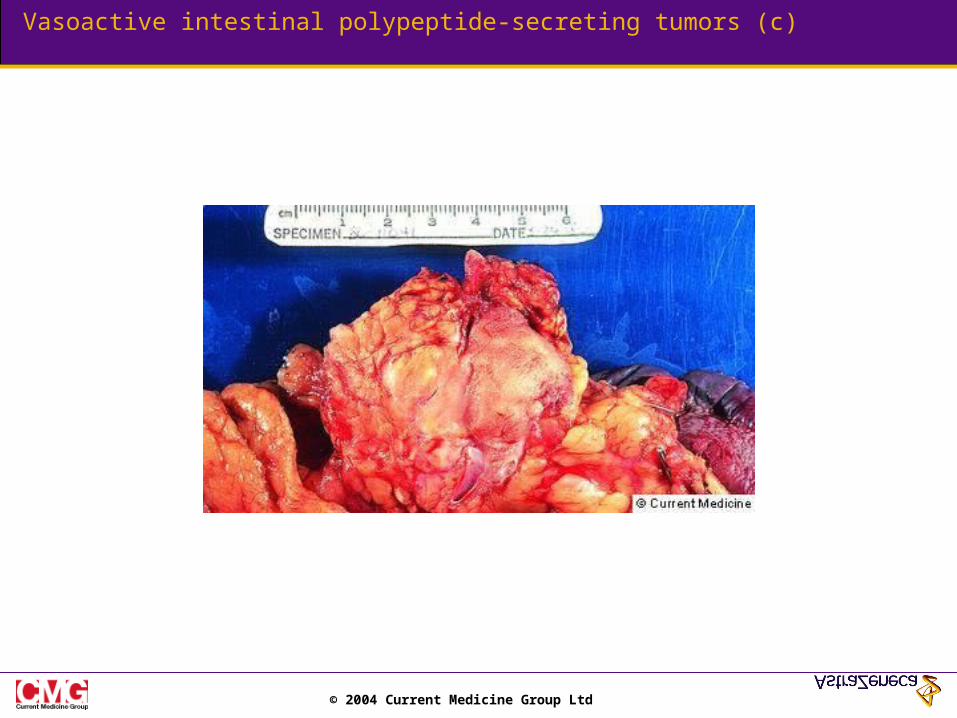
Vasoactive intestinal polypeptide-secreting tumors (c)
© 2004 Current Medicine Group Ltd
Vasoactive intestinal polypeptide-secreting tumors (d)
© 2004 Current Medicine Group Ltd
Medullary carcinoma of the thyroid products
© 2004 Current Medicine Group Ltd
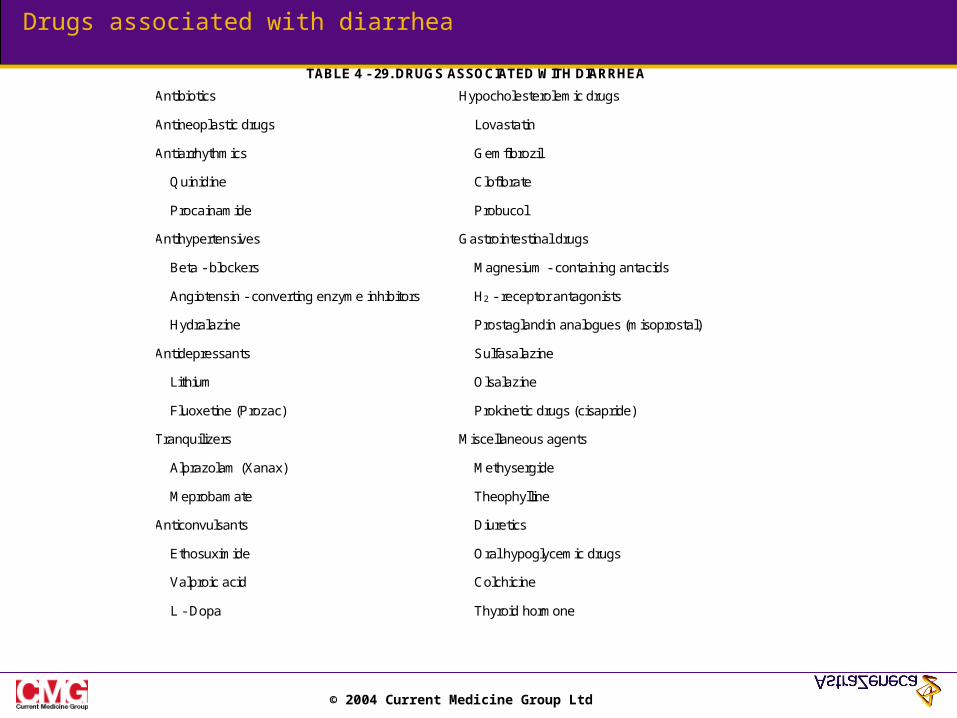
Drugs associated with diarrhea
TABLE 4 - 29. DRUGS ASSOCIATED WITH DIARRHEA
Antibiotics Hypocholesterolemic drugs
Antineoplastic drugs Lovastatin
Antiarrhythmics Gemfibrozil
Quinidine Clofibrate
Procainamide Probucol
Antihypertensives Gastrointestinal drugs
Beta - blockers Magnesium - containing antacids
Angiotensin - converting enzyme inhibitors H2 - receptor antagonists
Hydralazine Prostaglandin analogues (misoprostal)
Antidepressants Sulfasalazine
Lithium Olsalazine
Fluoxetine (Prozac) Prokinetic drugs (cisapride)
Tranquilizers Miscellaneous agents
Alprazolam (Xanax) Methysergide
Meprobamate Theophylline
Anticonvulsants Diuretics
Ethosuximide Oral hypoglycemic drugs
Valproic acid Colchicine
L - Dopa Thyroid hormone
© 2004 Current Medicine Group Ltd
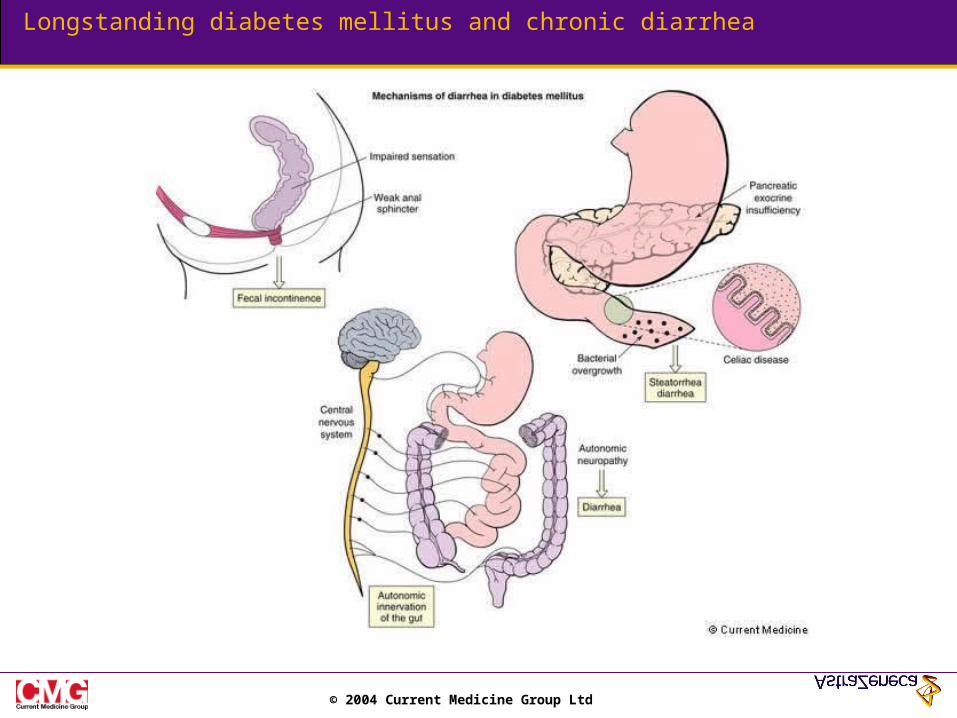
Longstanding diabetes mellitus and chronic diarrhea
© 2004 Current Medicine Group Ltd
Malabsorción - Esteatorrea
© 2004 Current Medicine Group Ltd
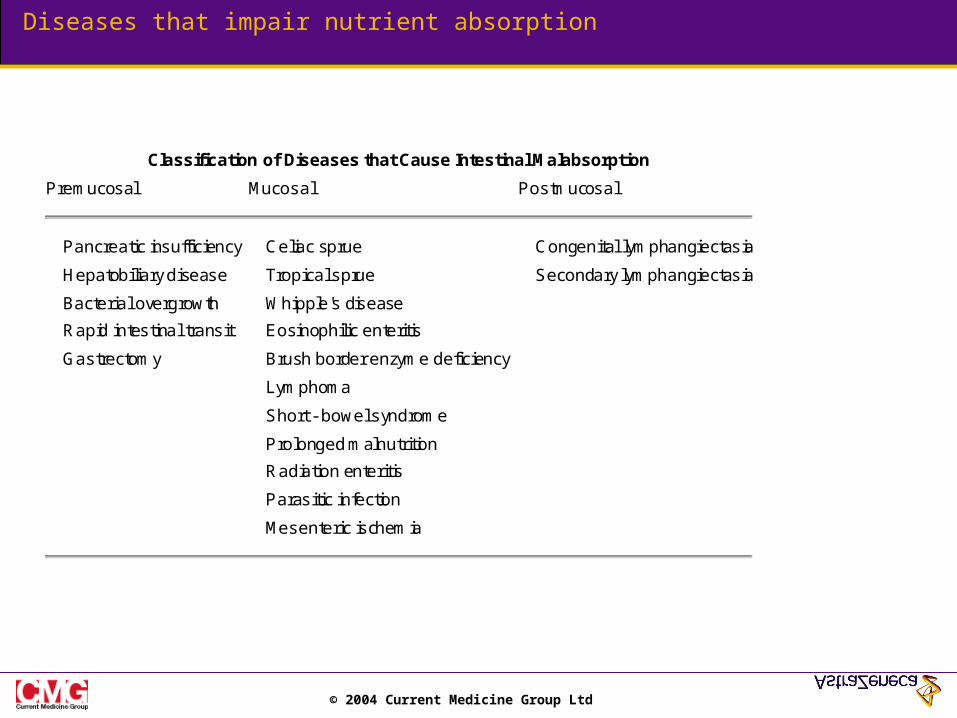
Diseases that impair nutrient absorption
Classification of Diseases that Cause Intestinal Malabsorption
Premucosal Mucosal Postmucosal
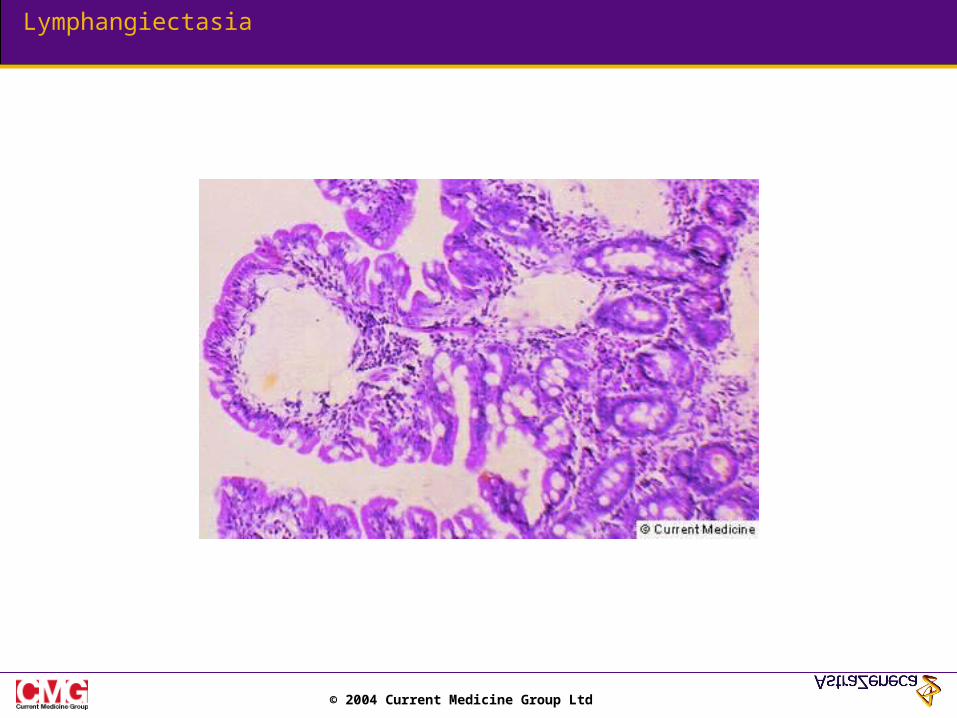
Pancreatic insufficiency Celiac sprue Congenital lymphangiectasia
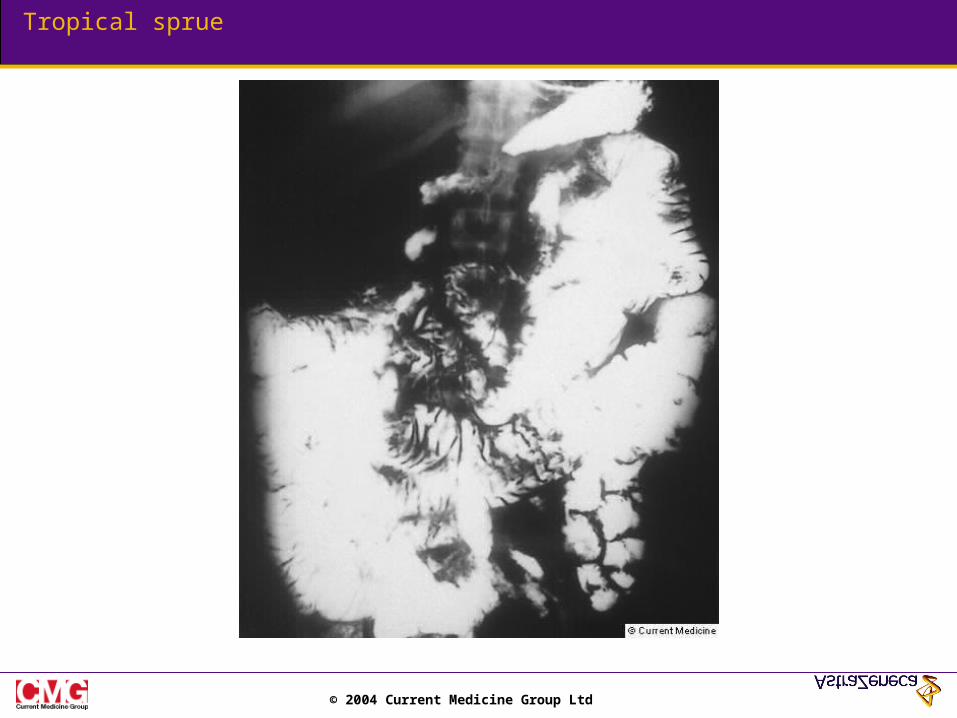
Hepatobiliary disease Tropical sprue Secondary lymphangiectasia
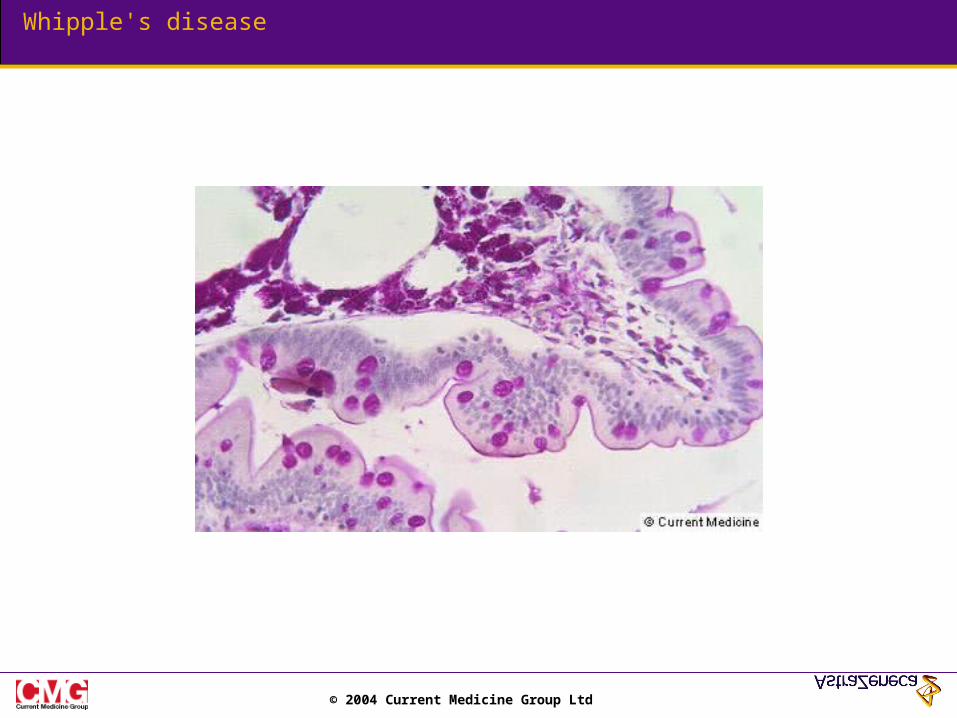
Bacterial overgrowth Whipple's disease
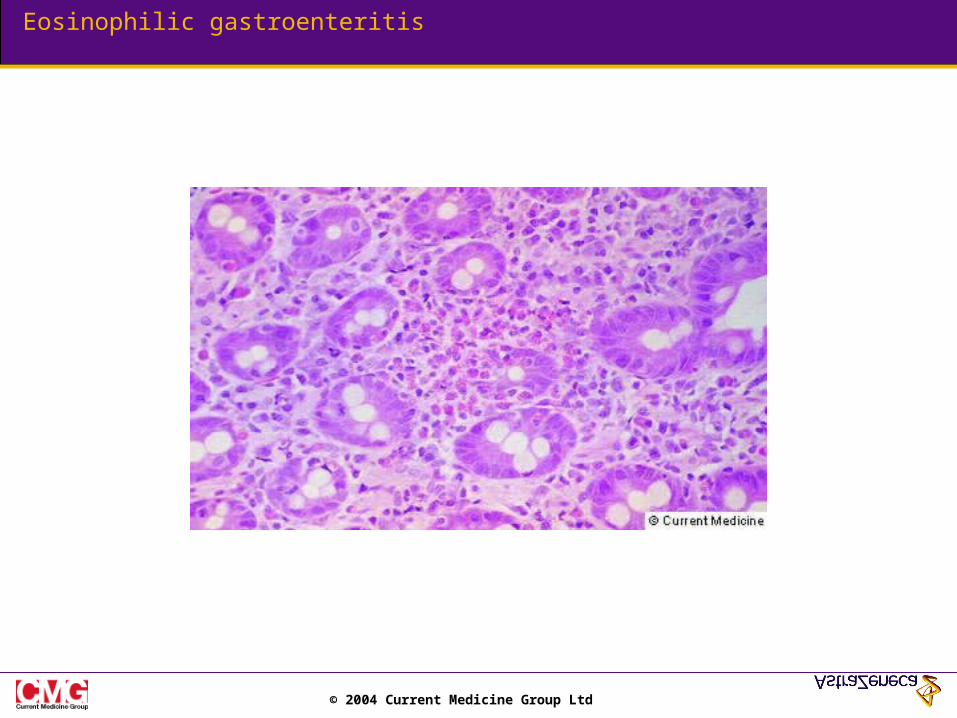
Rapid intestinal transit Eosinophilic enteritis
Gastrectomy Brush border enzyme deficiency
Lymphoma
Short - bowel syndrome
Prolonged malnutrition
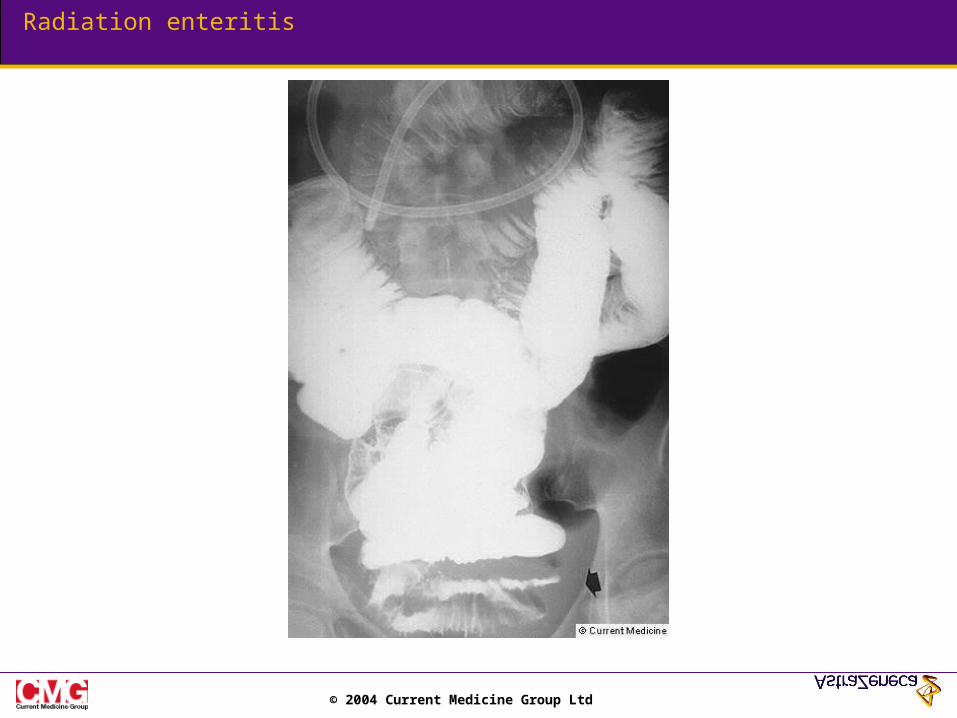
Radiation enteritis
Parasitic infection
Mesenteric ischemia
© 2004 Current Medicine Group Ltd
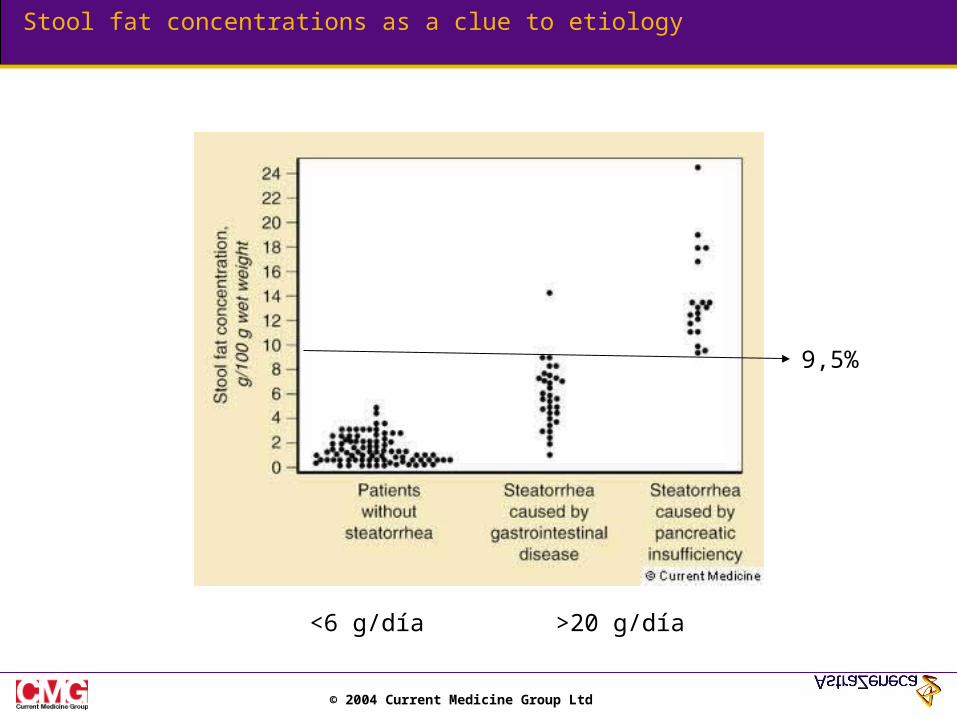
Stool fat concentrations as a clue to etiology
<6 g/día >20 g/día
9,5%
© 2004 Current Medicine Group Ltd
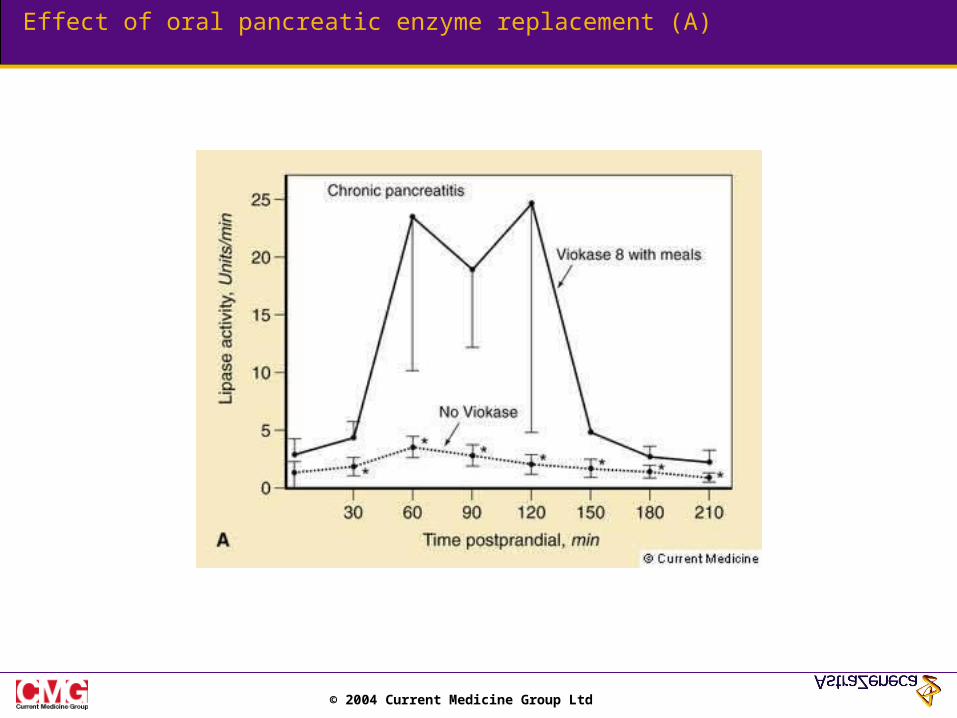
Effect of oral pancreatic enzyme replacement (A)
© 2004 Current Medicine Group Ltd
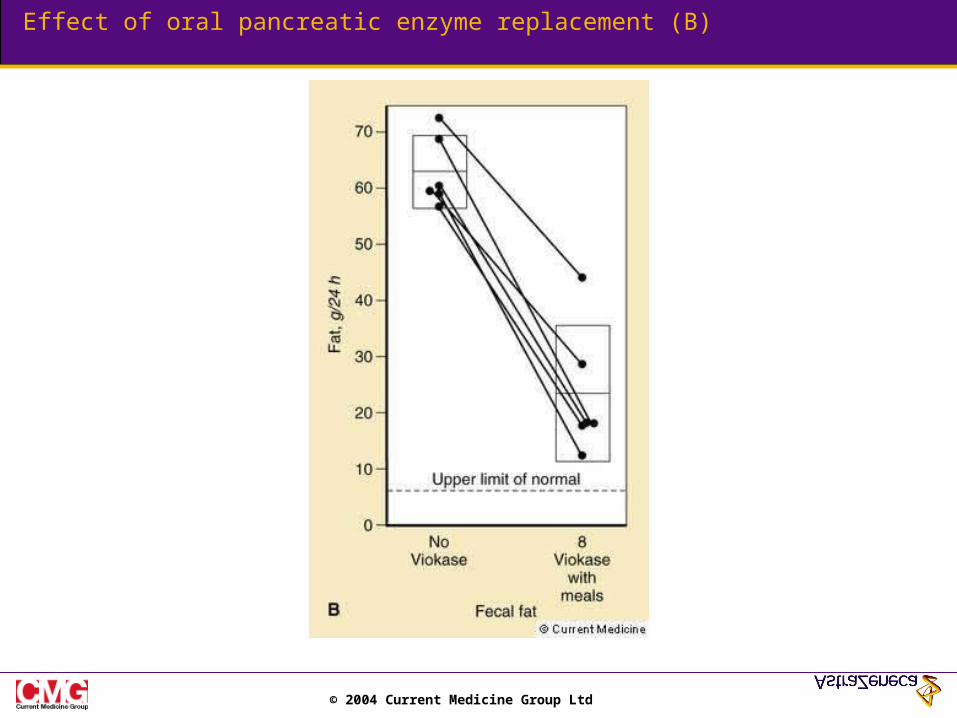
Effect of oral pancreatic enzyme replacement (B)
© 2004 Current Medicine Group Ltd
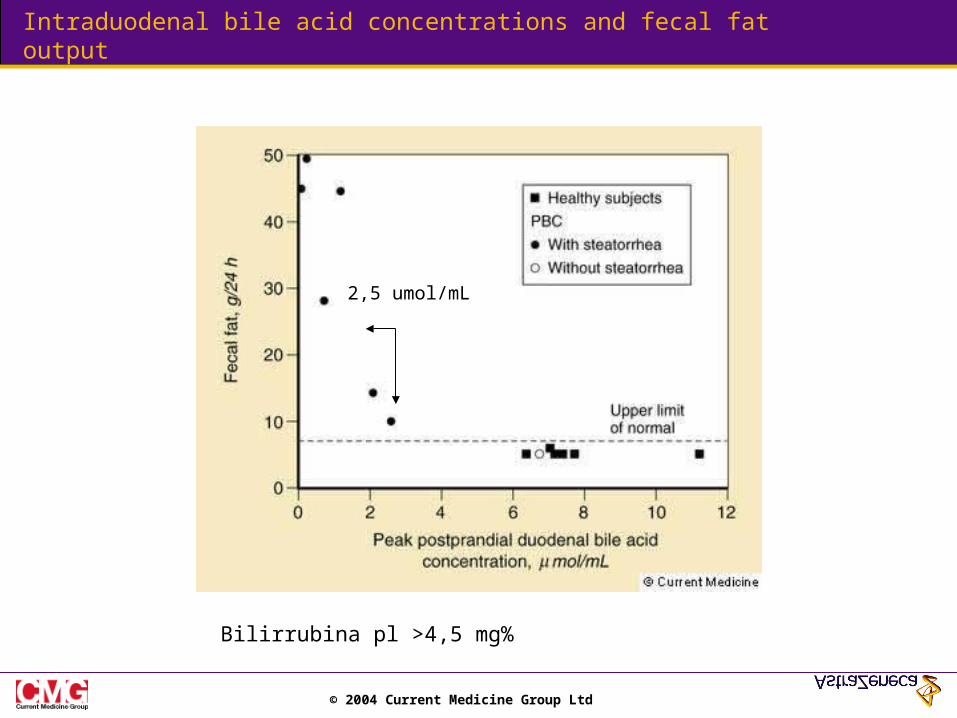
Intraduodenal bile acid concentrations and fecal fat output
2,5 umol/mL
Bilirrubina pl >4,5 mg%
© 2004 Current Medicine Group Ltd
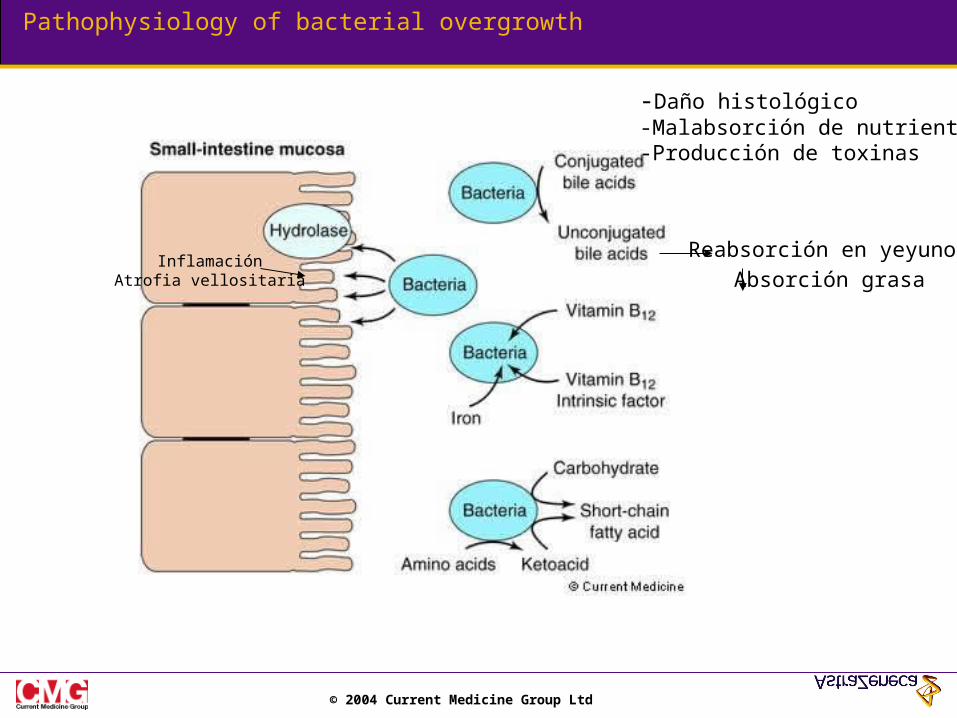
Pathophysiology of bacterial overgrowth
InflamaciónAtrofia vellositaria
-Daño histológico-Malabsorción de nutrientes-Producción de toxinas
Reabsorción en yeyuno
Absorción grasa
© 2004 Current Medicine Group Ltd
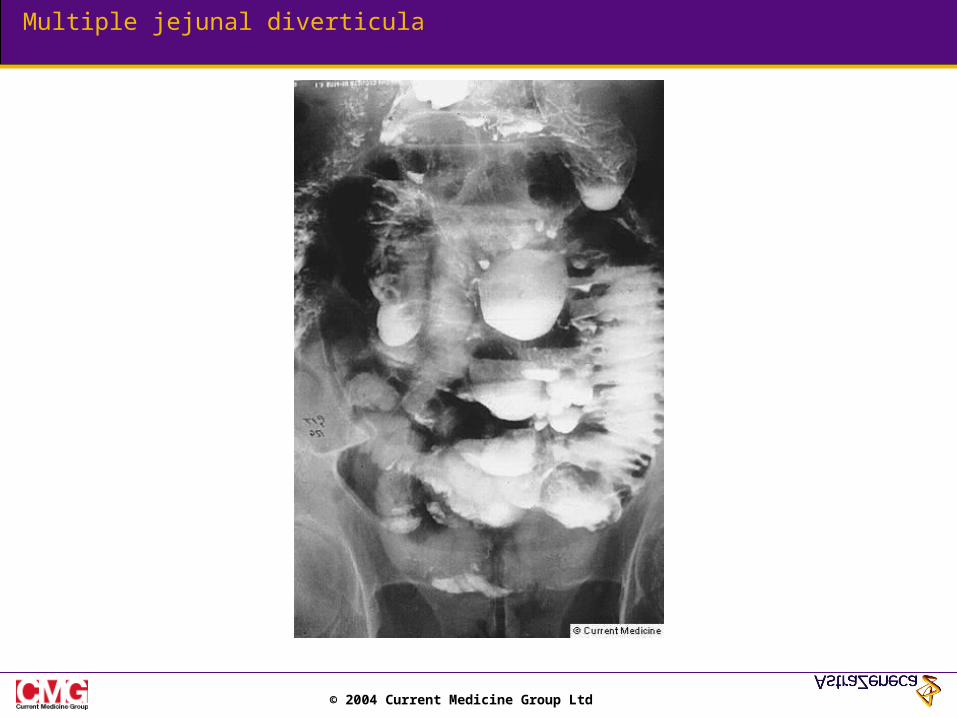
Multiple jejunal diverticula

© 2004 Current Medicine Group Ltd
Multiple small bowel diverticula
© 2004 Current Medicine Group Ltd
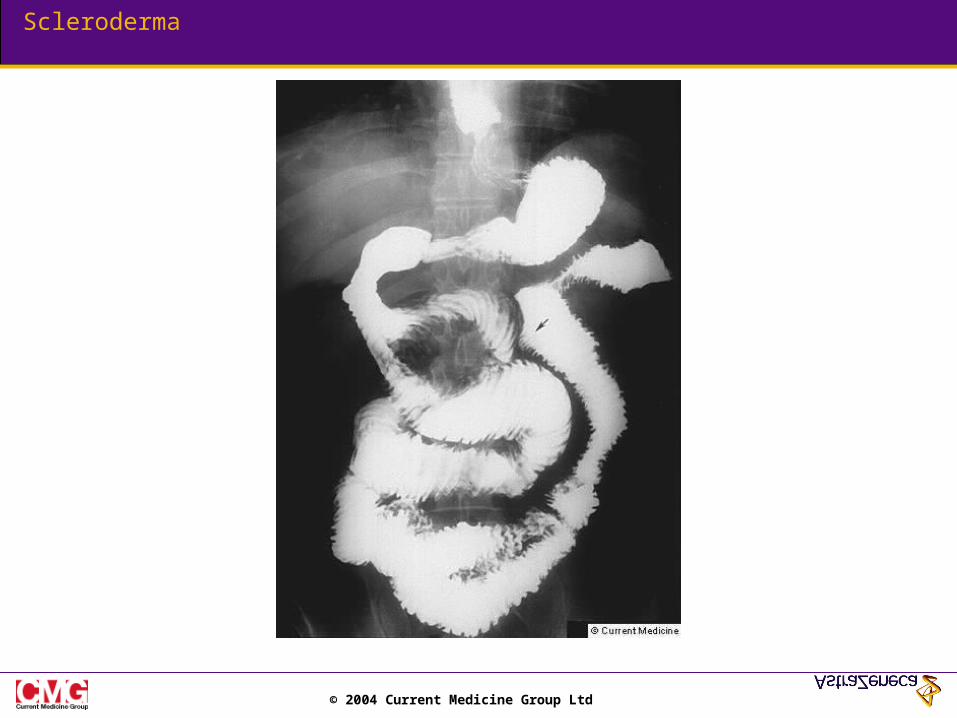
Scleroderma
© 2004 Current Medicine Group Ltd
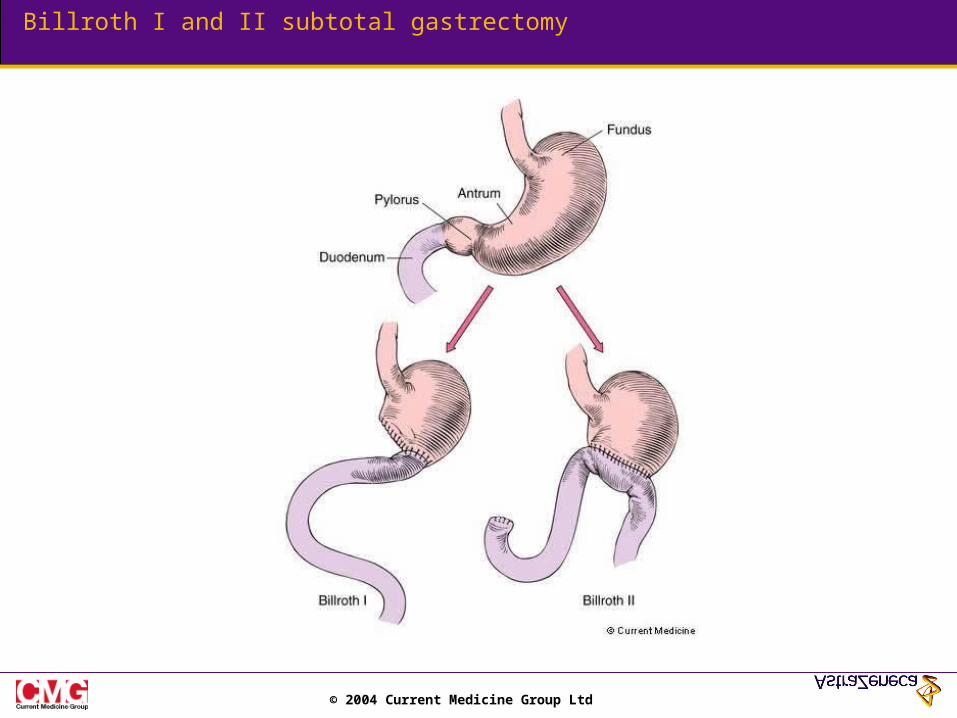
Billroth I and II subtotal gastrectomy
© 2004 Current Medicine Group Ltd
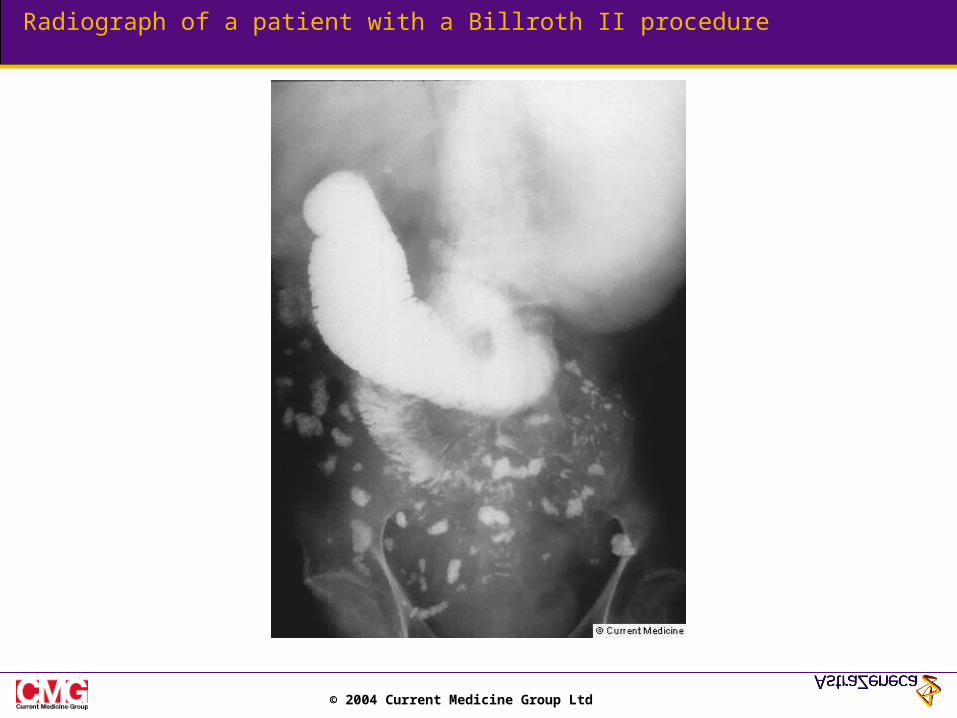
Radiograph of a patient with a Billroth II procedure
© 2004 Current Medicine Group Ltd
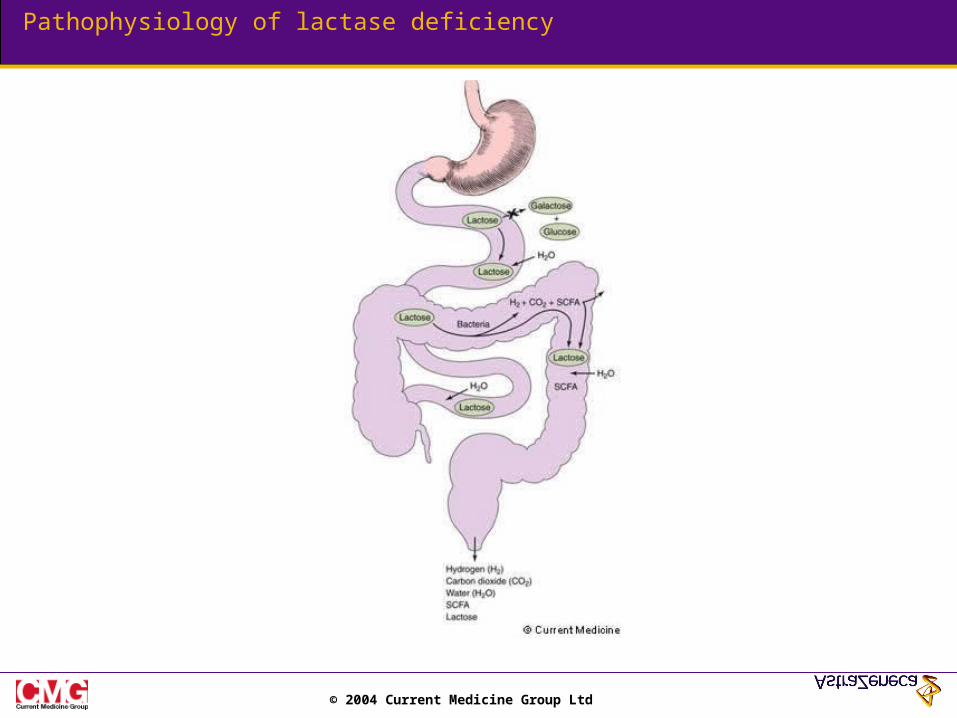
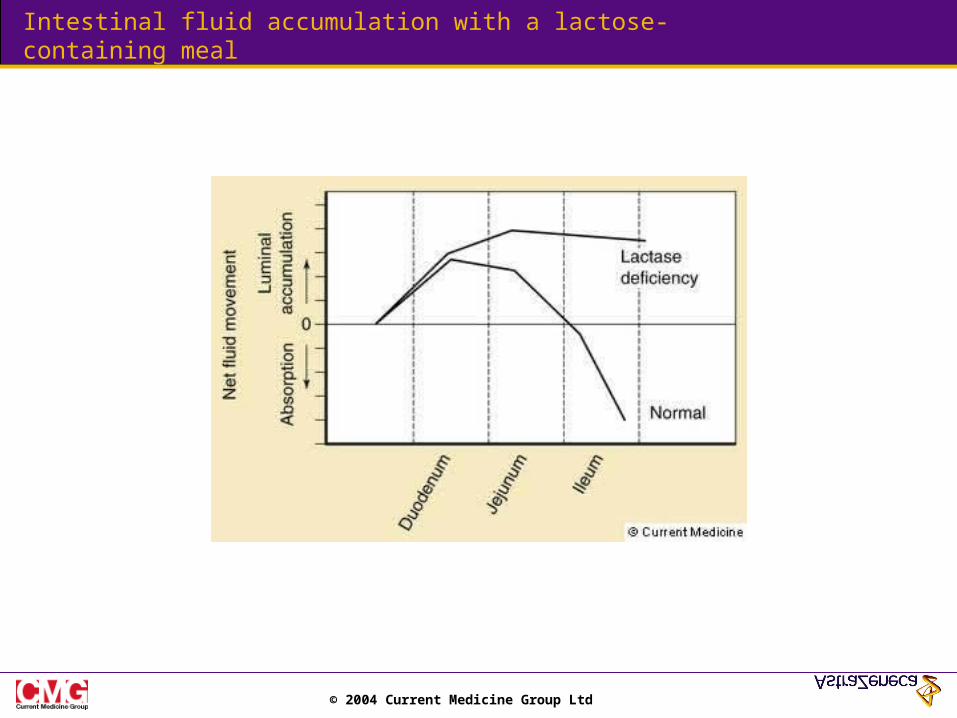
Pathophysiology of lactase deficiency
© 2004 Current Medicine Group Ltd
Intestinal fluid accumulation with a lactose-containing meal
© 2004 Current Medicine Group Ltd
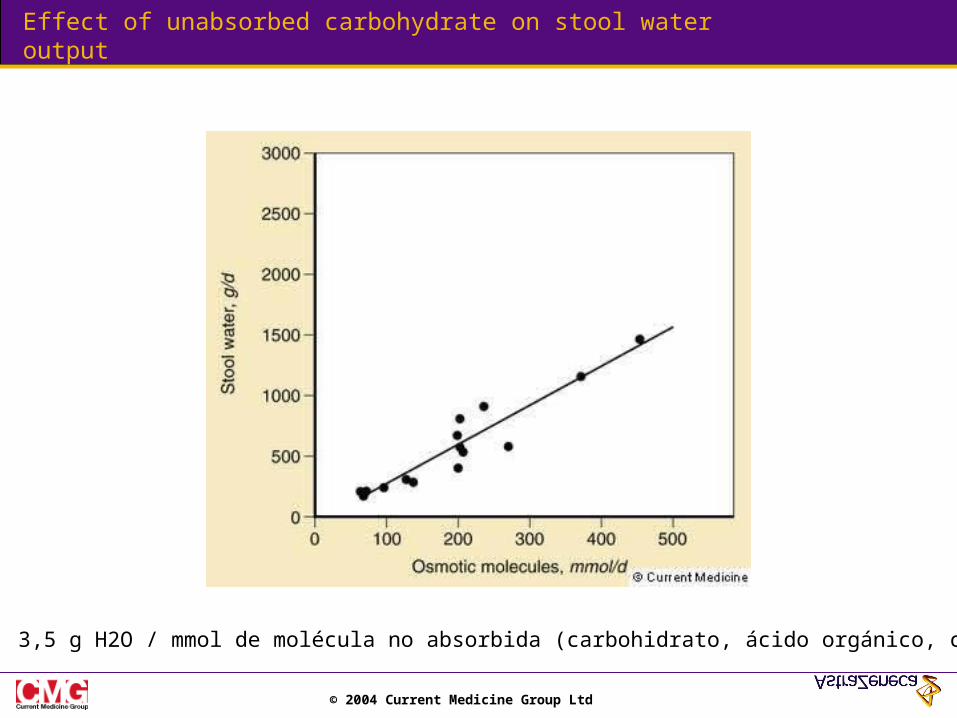
Effect of unabsorbed carbohydrate on stool water output
3,5 g H2O / mmol de molécula no absorbida (carbohidrato, ácido orgánico, catión)
© 2004 Current Medicine Group Ltd
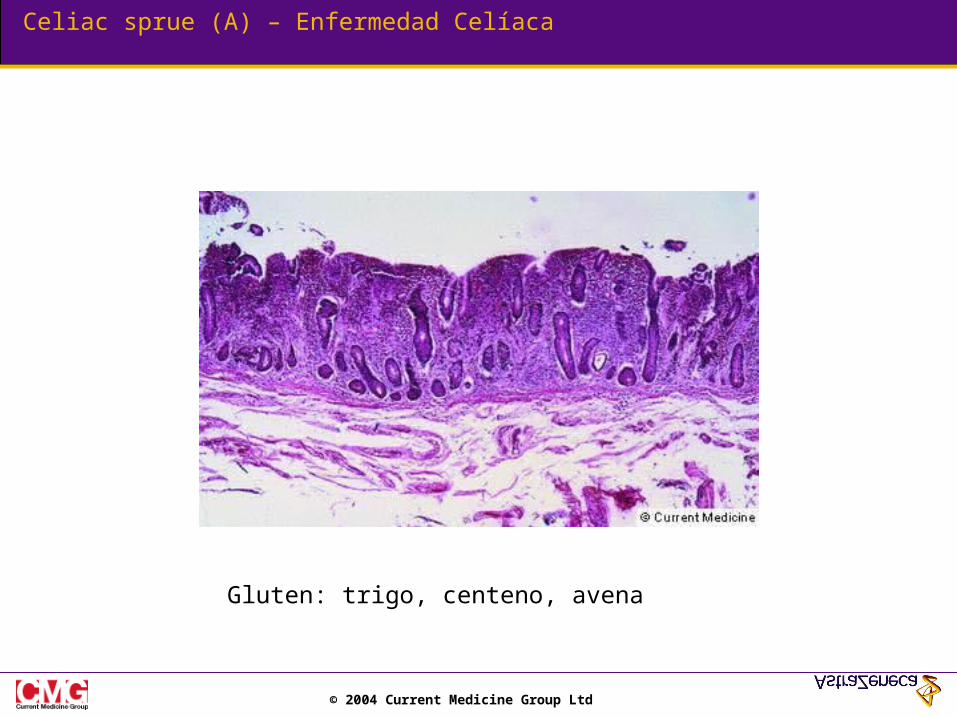
Celiac sprue (A) – Enfermedad Celíaca
Gluten: trigo, centeno, avena

© 2004 Current Medicine Group Ltd
Celiac sprue (B)
Tres meses después de dieta libre de gluten
© 2004 Current Medicine Group Ltd
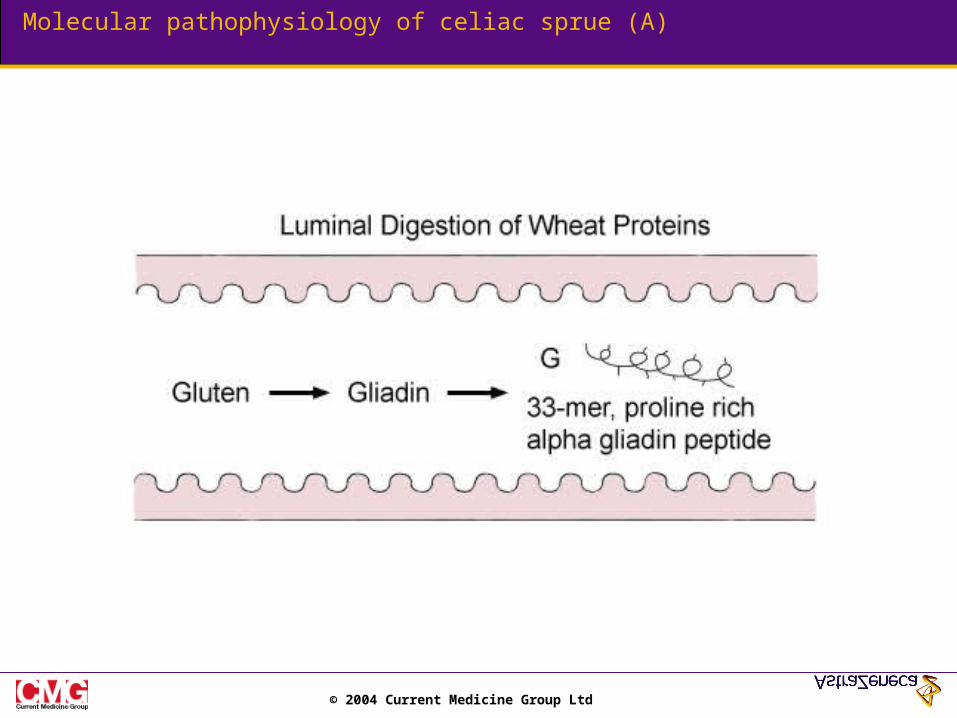
Molecular pathophysiology of celiac sprue (A)
© 2004 Current Medicine Group Ltd
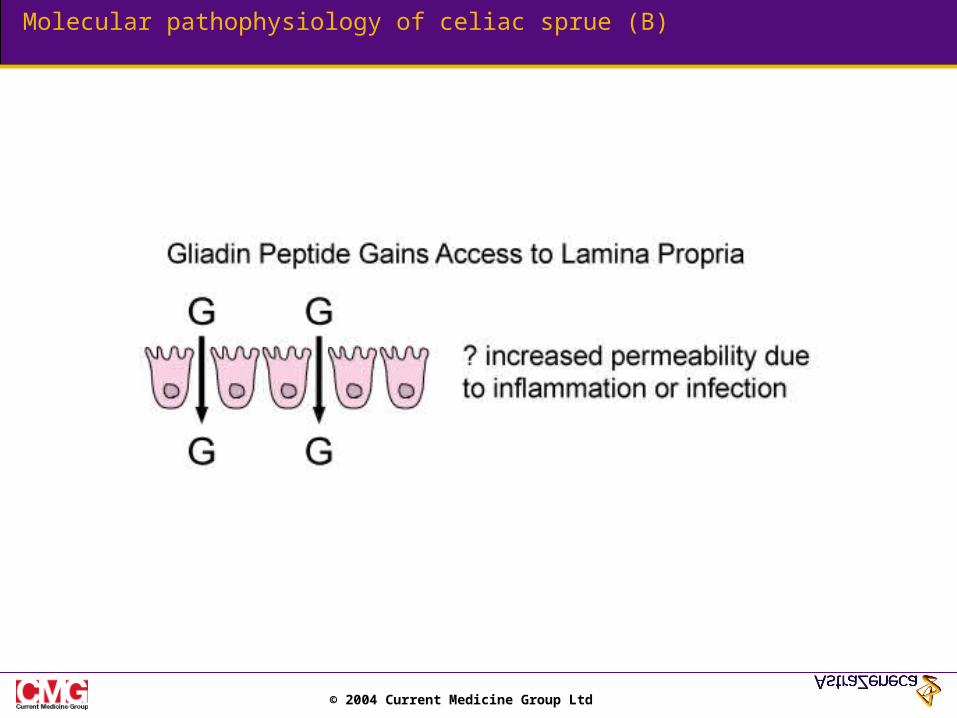
Molecular pathophysiology of celiac sprue (B)
© 2004 Current Medicine Group Ltd
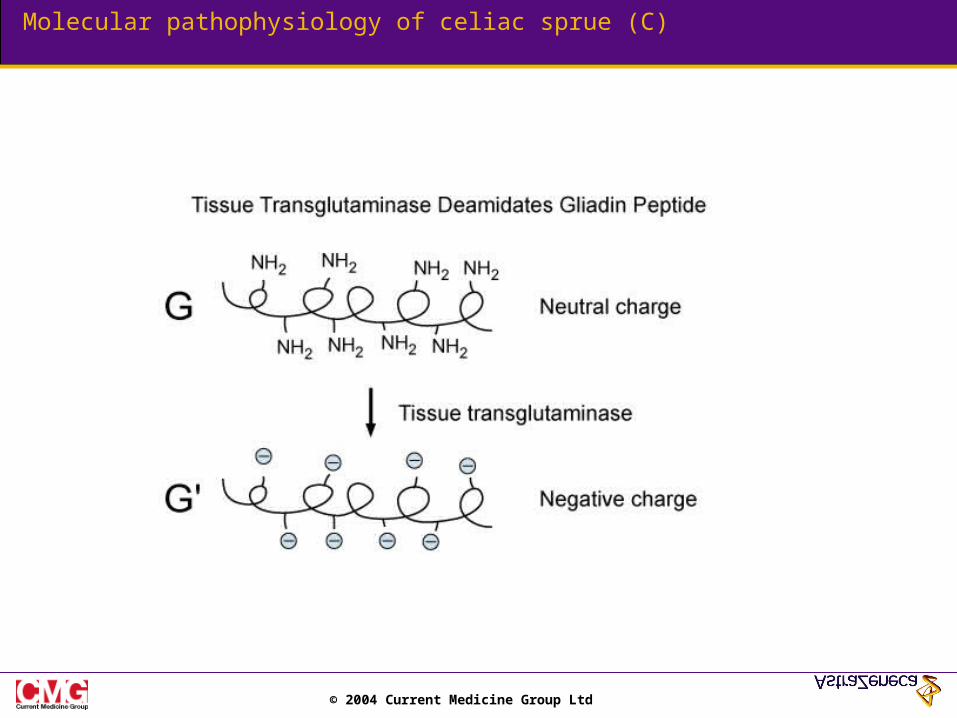
Molecular pathophysiology of celiac sprue (C)
© 2004 Current Medicine Group Ltd
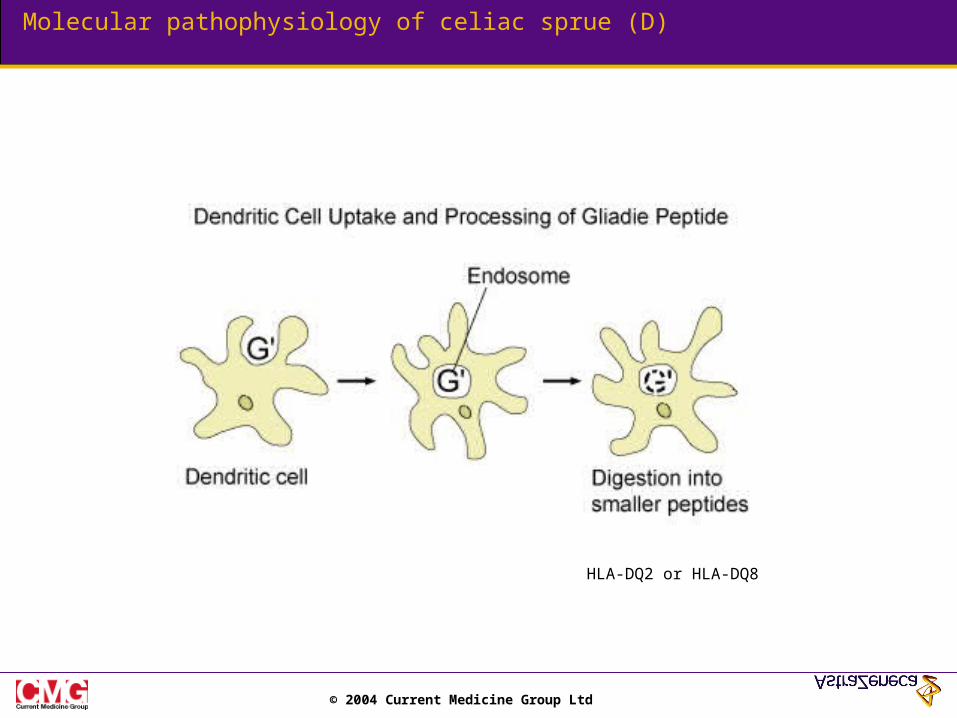
Molecular pathophysiology of celiac sprue (D)
HLA-DQ2 or HLA-DQ8
© 2004 Current Medicine Group Ltd
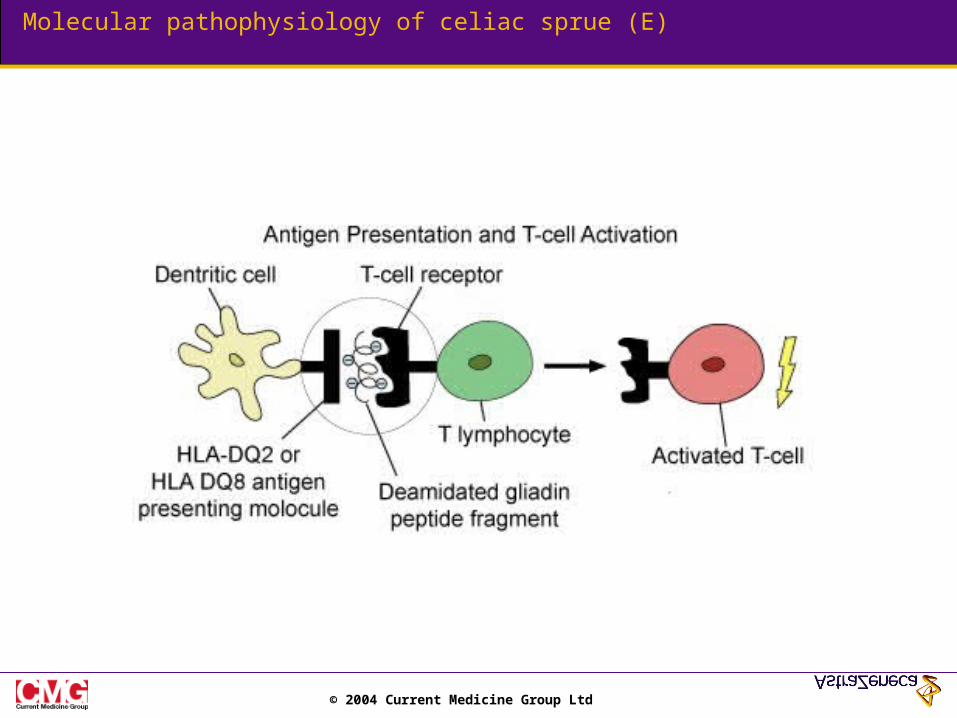
Molecular pathophysiology of celiac sprue (E)
© 2004 Current Medicine Group Ltd
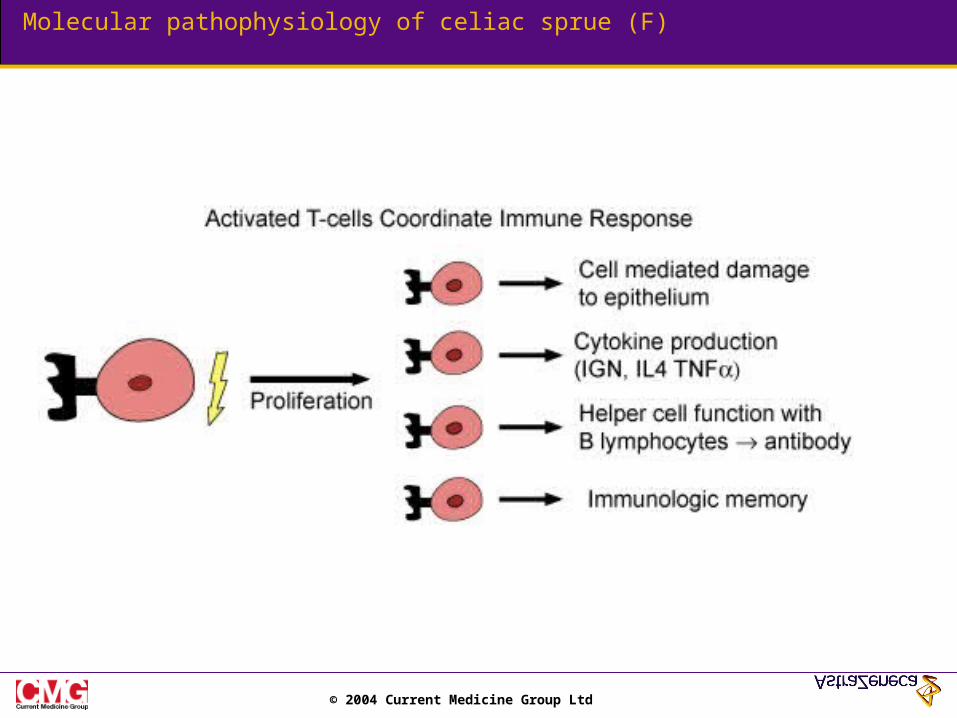
Molecular pathophysiology of celiac sprue (F)
© 2004 Current Medicine Group Ltd
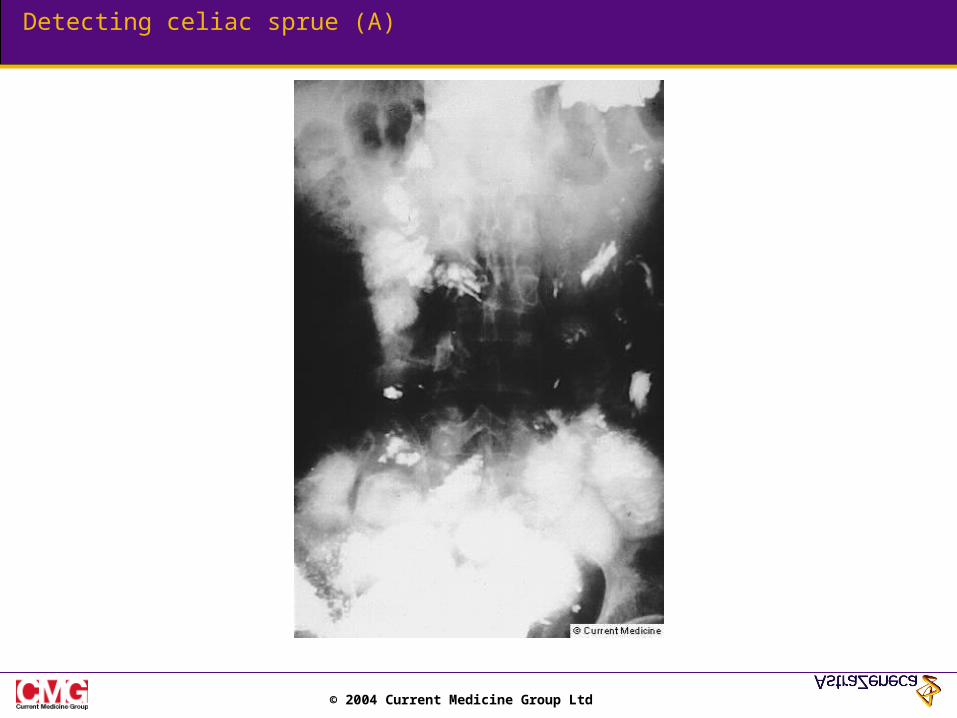
Detecting celiac sprue (A)
© 2004 Current Medicine Group Ltd
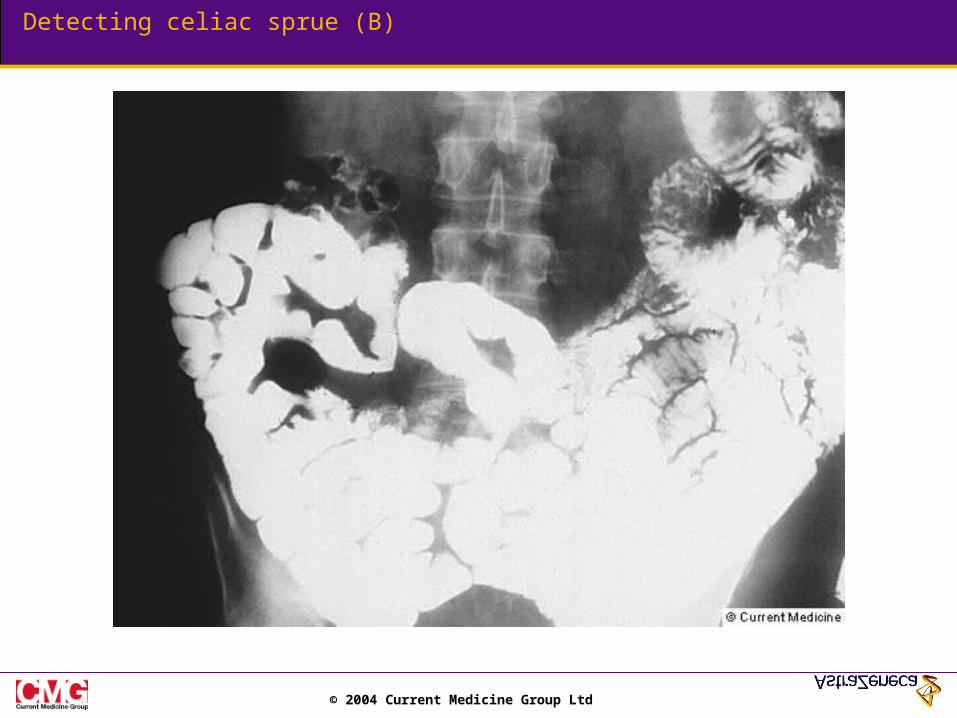
Detecting celiac sprue (B)
© 2004 Current Medicine Group Ltd
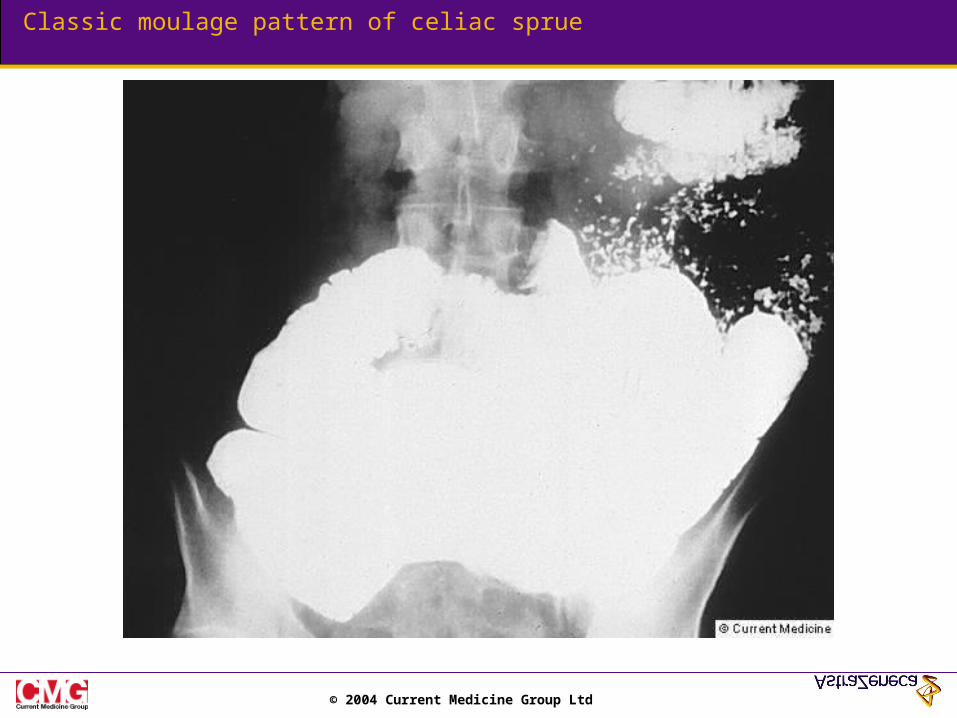
Classic moulage pattern of celiac sprue
© 2004 Current Medicine Group Ltd
Tropical sprue
© 2004 Current Medicine Group Ltd
Whipple's disease
© 2004 Current Medicine Group Ltd
Eosinophilic gastroenteritis
© 2004 Current Medicine Group Ltd
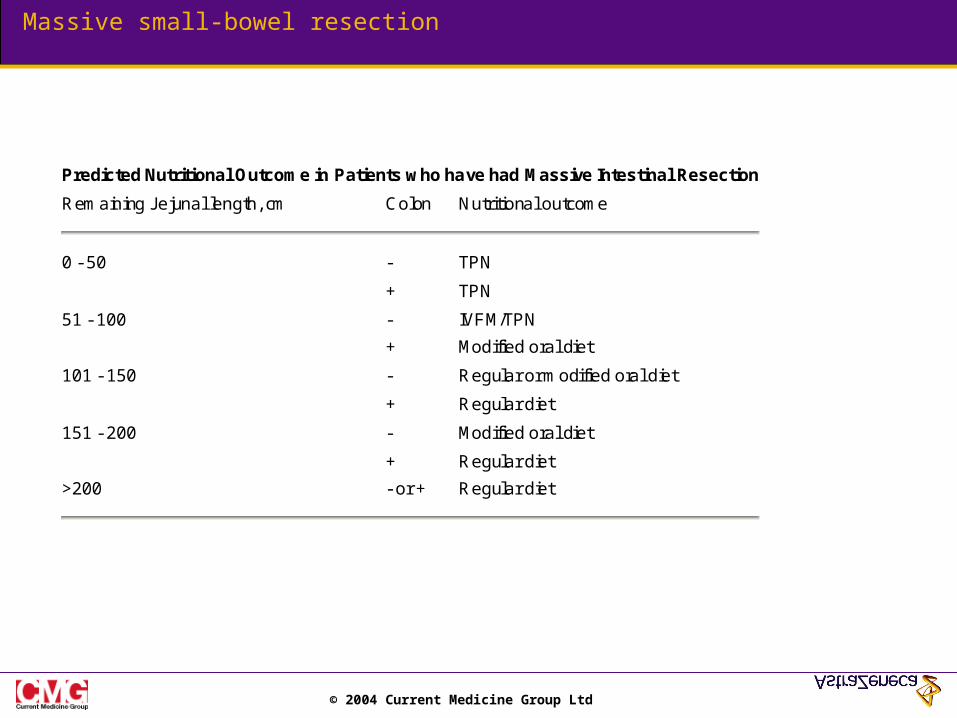
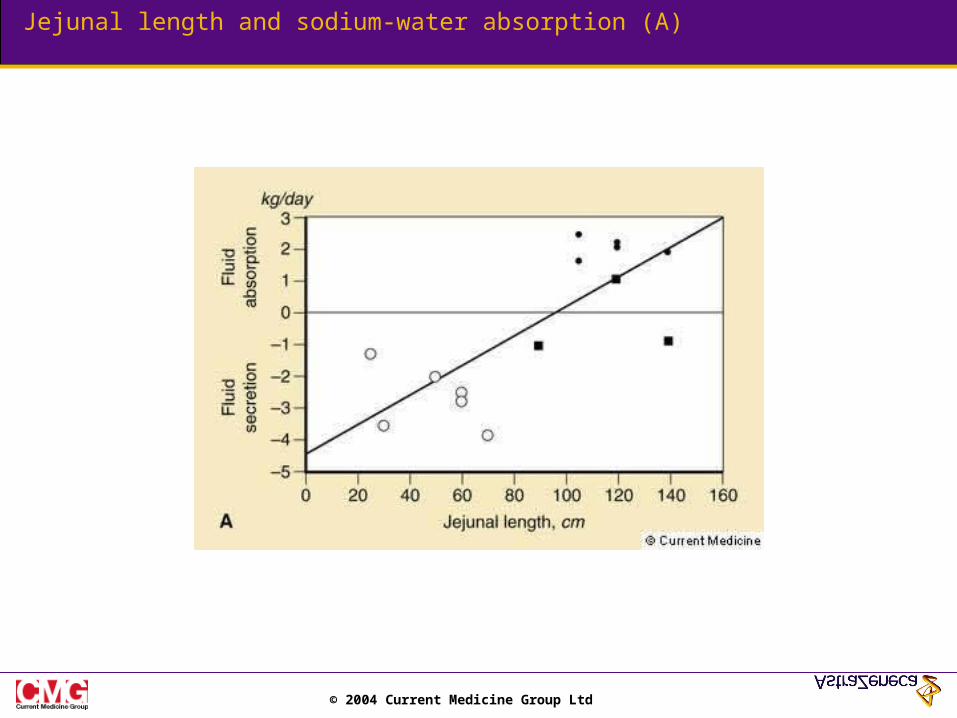
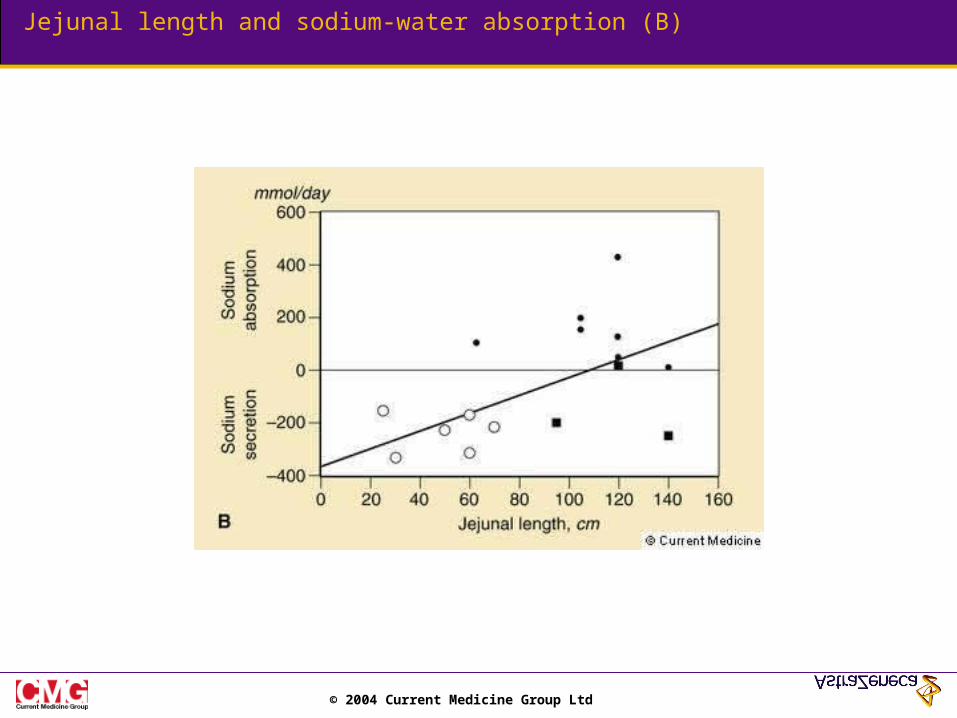
Massive small-bowel resection
Predicted Nutritional Outcome in Patients who have had Massive Intestinal Resection
Remaining Jejunal length, cm Colon Nutritional outcome
0 - 50 - TPN
+ TPN
51 - 100 - IVFM/TPN
+ Modified oral diet
101 - 150 - Regular or modified oral diet
+ Regular diet
151 - 200 - Modified oral diet
+ Regular diet
>200 - or + Regular diet
© 2004 Current Medicine Group Ltd
Jejunal length and sodium-water absorption (A)
© 2004 Current Medicine Group Ltd
Jejunal length and sodium-water absorption (B)
© 2004 Current Medicine Group Ltd
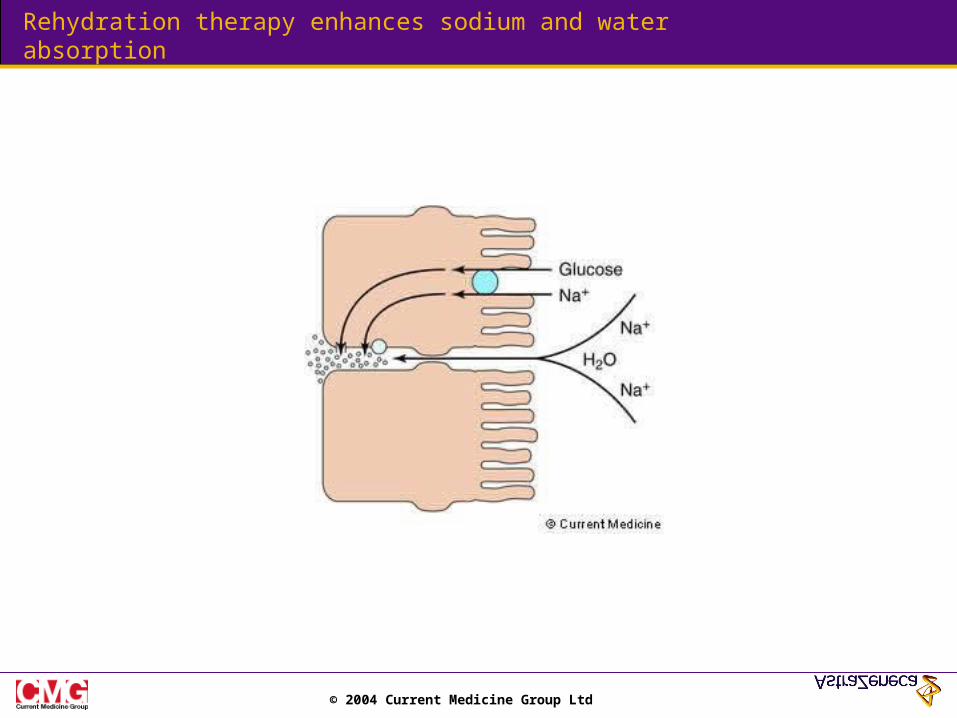
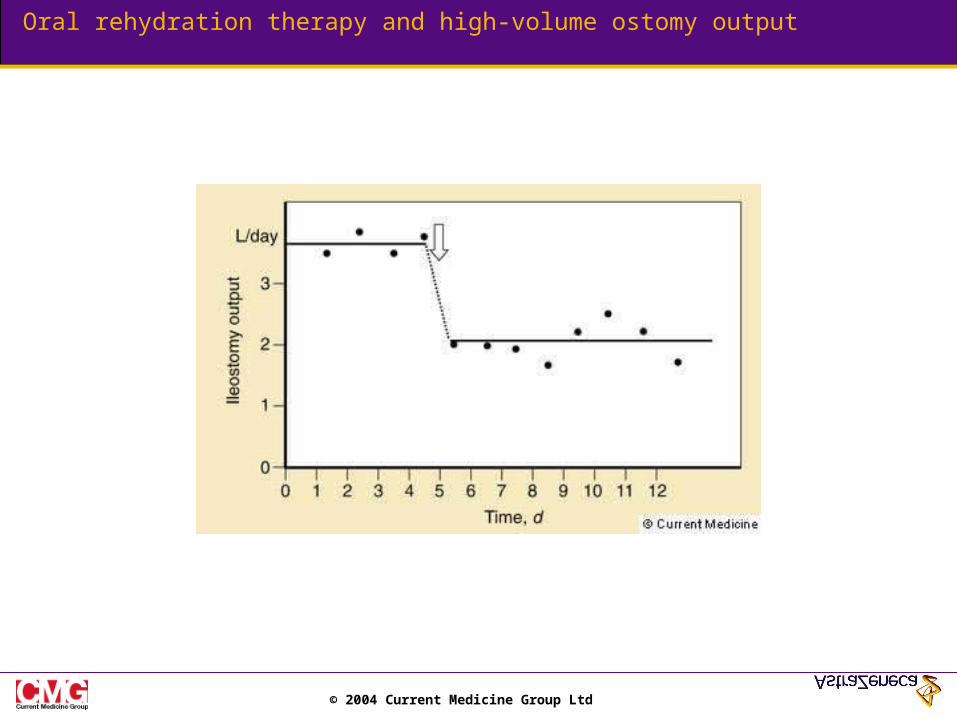
Rehydration therapy enhances sodium and water absorption
© 2004 Current Medicine Group Ltd
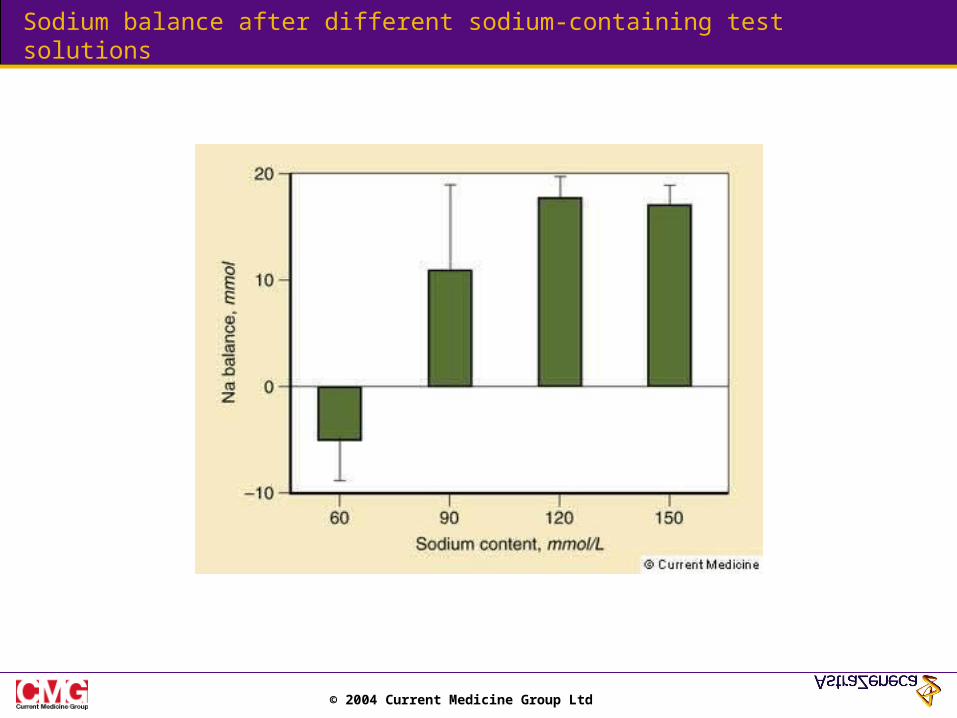
Sodium balance after different sodium-containing test solutions
© 2004 Current Medicine Group Ltd
Oral rehydration therapy and high-volume ostomy output
© 2004 Current Medicine Group Ltd
Radiation enteritis
© 2004 Current Medicine Group Ltd
Lymphangiectasia
© 2004 Current Medicine Group Ltd
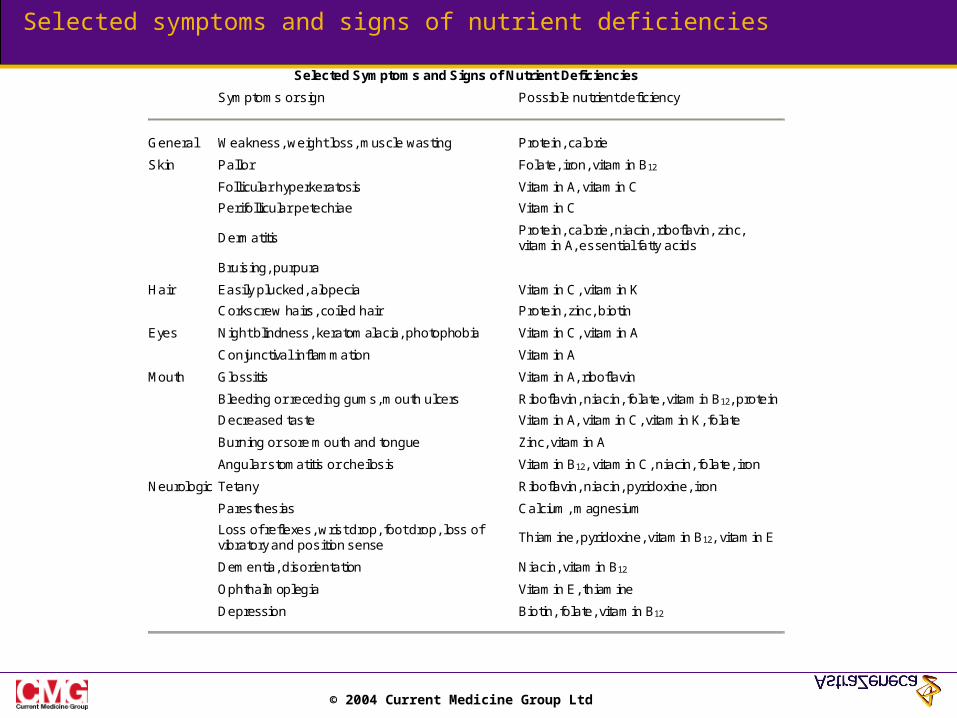
Selected symptoms and signs of nutrient deficiencies
Selected Symptoms and Signs of Nutrient Deficiencies
Symptoms or sign Possible nutrient deficiency
General Weakness, weight loss, muscle wasting Protein, calorie
Skin Pallor Folate, iron, vitamin B12
Follicular hyperkeratosis Vitamin A, vitamin C
Perifollicular petechiae Vitamin C
Dermatitis Protein, calorie, niacin, riboflavin, zinc, vitamin A, essential fatty acids
Bruising, purpura
Hair Easily plucked, alopecia Vitamin C, vitamin K
Corkscrew hairs, coiled hair Protein, zinc, biotin
Eyes Night blindness, keratomalacia, photophobia Vitamin C, vitamin A
Conjunctival inflammation Vitamin A
Mouth Glossitis Vitamin A, riboflavin
Bleeding or receding gums, mouth ulcers Riboflavin, niacin, folate, vitamin B12, protein
Decreased taste Vitamin A, vitamin C, vitamin K, folate
Burning or sore mouth and tongue Zinc, vitamin A
Angular stomatitis or cheilosis Vitamin B12, vitamin C, niacin, folate, iron
Neurologic Tetany Riboflavin, niacin, pyridoxine, iron
Paresthesias Calcium, magnesium
Loss of reflexes, wrist drop, foot drop, loss of vibratory and position sense
Thiamine, pyridoxine, vitamin B12, vitamin E
Dementia, disorientation Niacin, vitamin B12
Ophthalmoplegia Vitamin E, thiamine
Depression Biotin, folate, vitamin B12
© 2004 Current Medicine Group Ltd
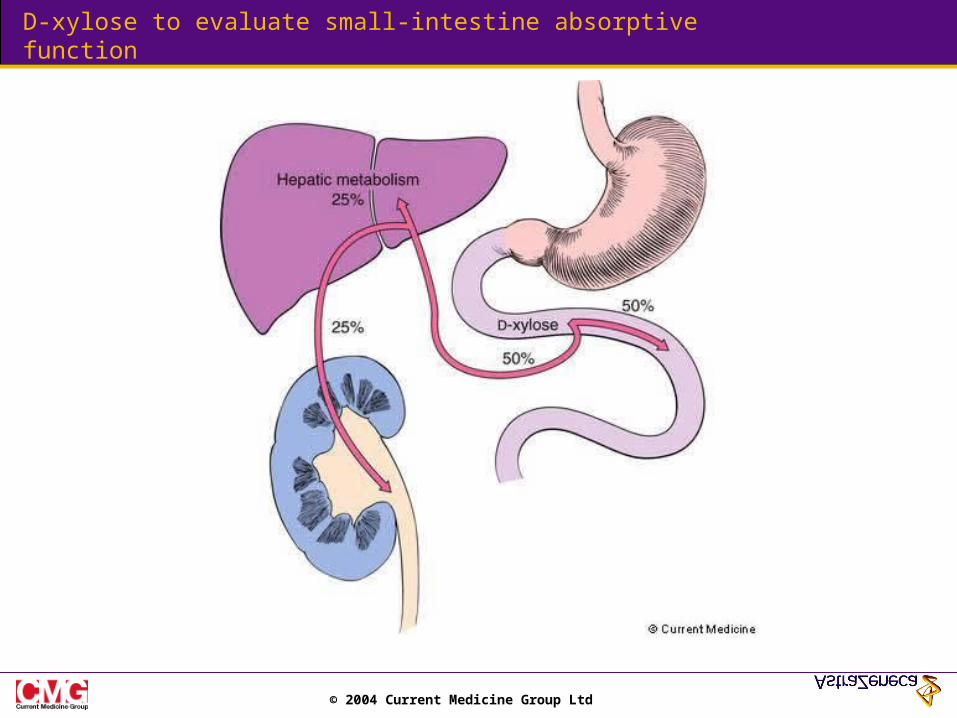
D-xylose to evaluate small-intestine absorptive function
© 2004 Current Medicine Group Ltd
Enfermedad Inflamatoria Intestinal
•Colitis Ulcerosa•Enfermedad de Crohn
© 2004 Current Medicine Group Ltd
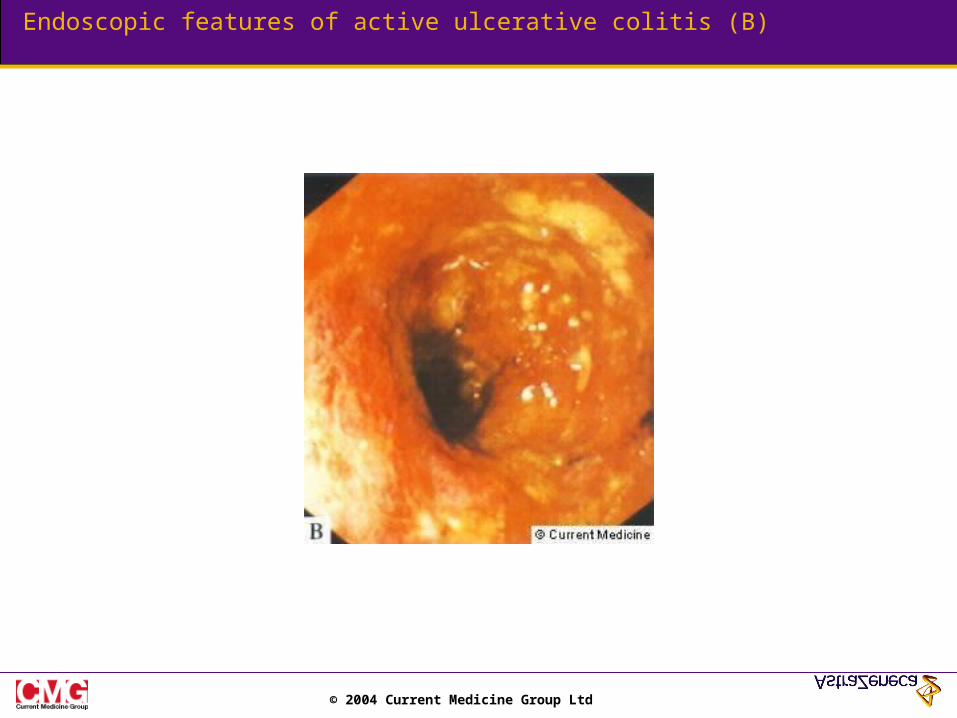
Endoscopic features of active ulcerative colitis (B)
© 2004 Current Medicine Group Ltd
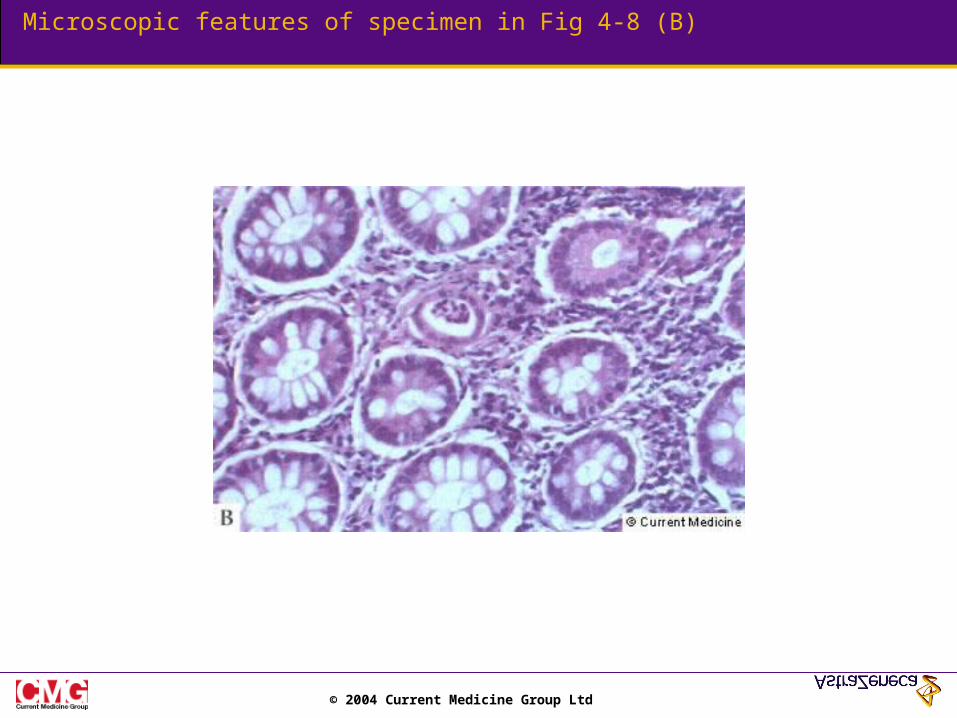
Microscopic features of specimen in Fig 4-8 (B)
© 2004 Current Medicine Group Ltd
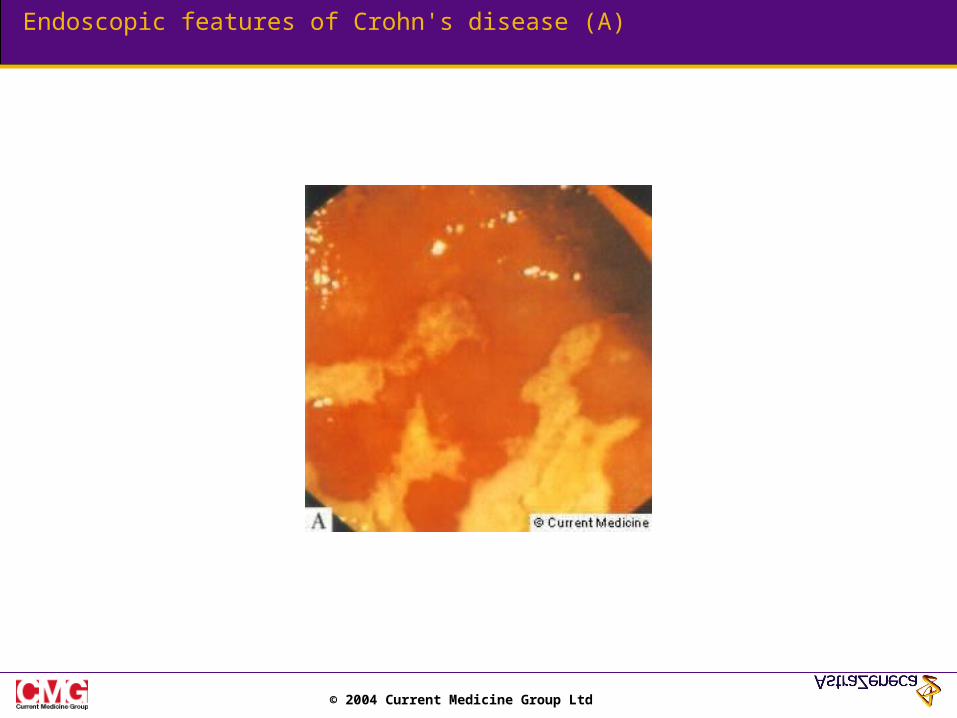
Endoscopic features of Crohn's disease (A)
© 2004 Current Medicine Group Ltd
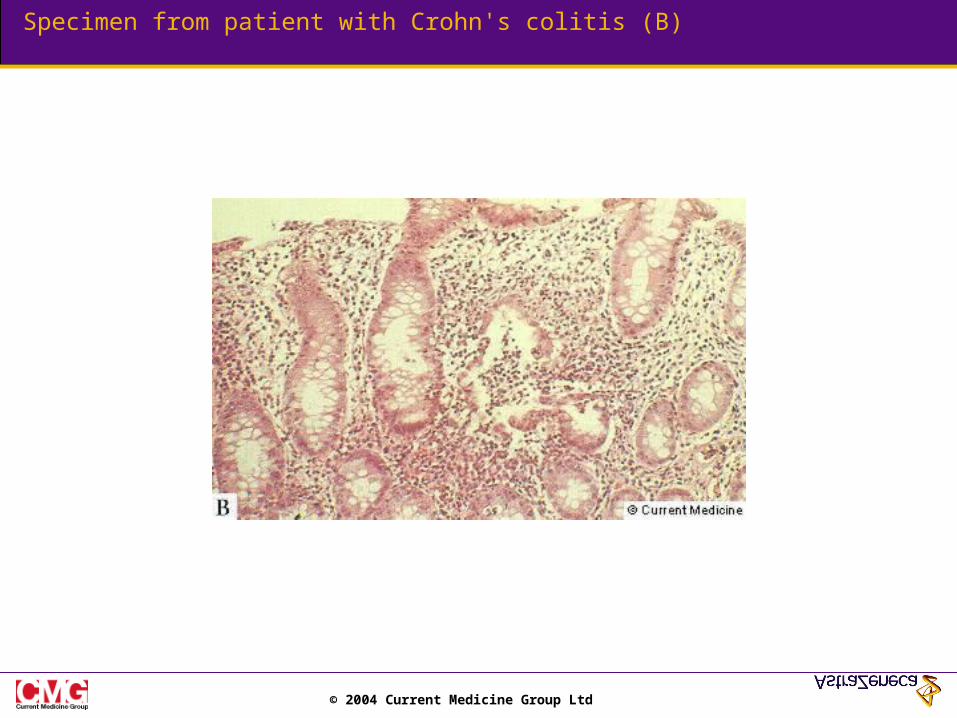
Specimen from patient with Crohn's colitis (B)
© 2004 Current Medicine Group Ltd
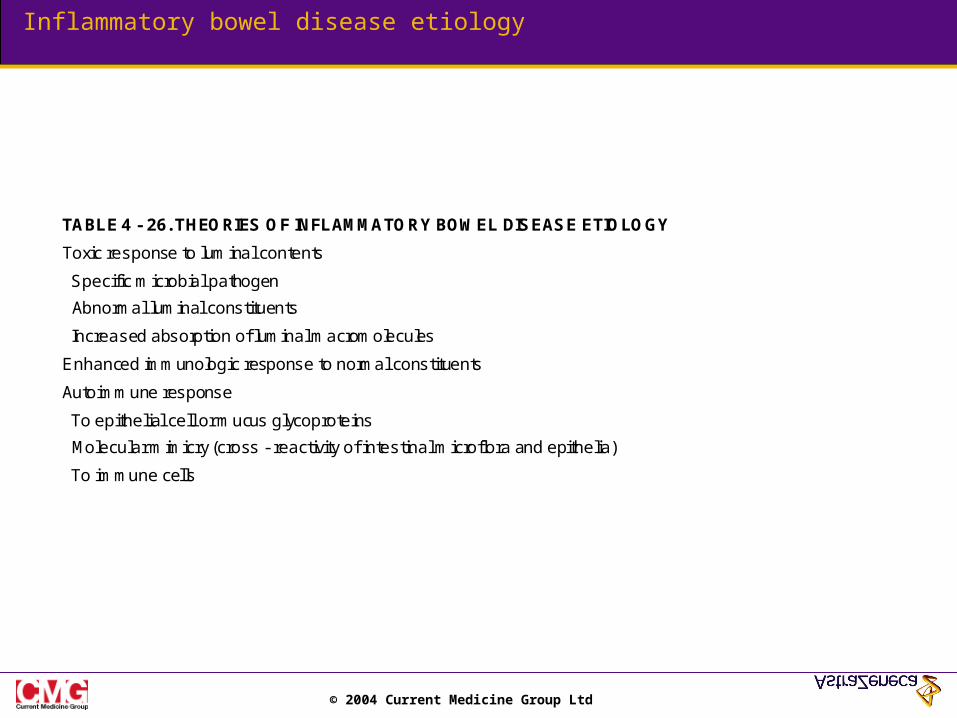
Inflammatory bowel disease etiology
TABLE 4 - 26. THEORIES OF INFLAMMATORY BOWEL DISEASE ETIOLOGY
Toxic response to luminal contents
Specific microbial pathogen
Abnormal luminal constituents
Increased absorption of luminal macromolecules
Enhanced immunologic response to normal constituents
Autoimmune response
To epithelial cell or mucus glycoproteins
Molecular mimicry (cross - reactivity of intestinal microflora and epithelia)
To immune cells
© 2004 Current Medicine Group Ltd
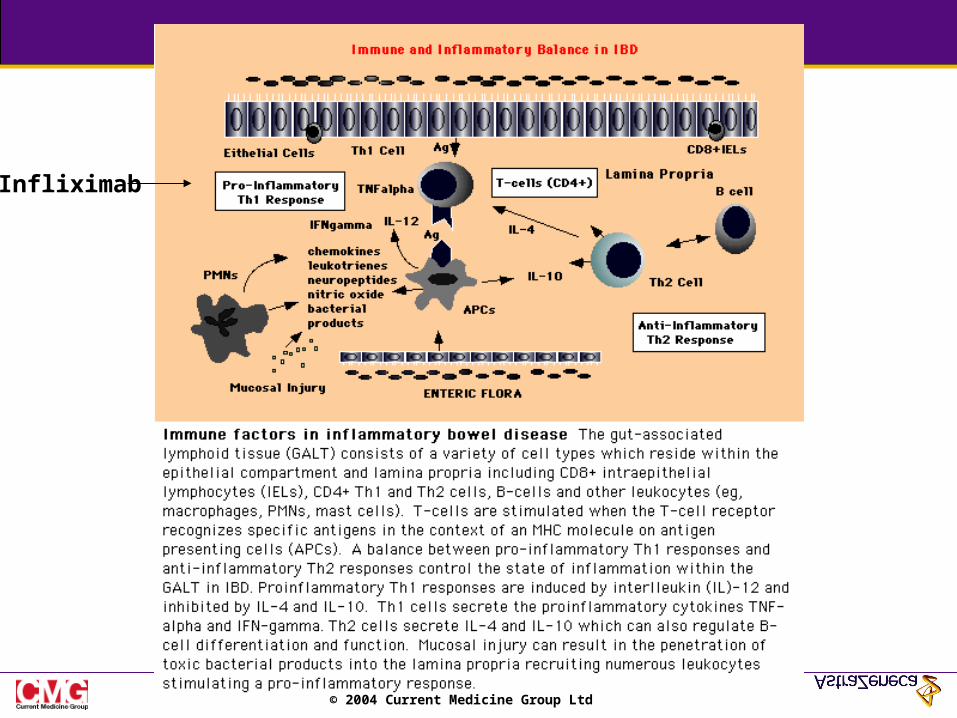
Infliximab
© 2004 Current Medicine Group Ltd
Related Documents











